Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
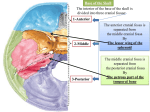
Gross Anatomy: 1:00 - 2:00 Scribe: Teresa Kilborn Monday, January 12, 2009 Proof: Ashley Holladay Dr. Tubbs Cranial Cavity Page 1 of 7 Abbreviations ACF- Anterior Cranial Fossa, MCF- Middle Cranial Fossa, PCF- Posterior Cranial Fossa, CNCranial nerves, ICA- Internal Carotid Artery **where audio picked up I. Video[S2]: II. Picture [S3] III. Picture of Cranial Fossa [S4] a. You will become very knowledgeable of the inside and outside of the skull. b. Basic way to fit the various parts together is to talk about ACF, MCF, and PCF- Think of it like a set of steps. c. Notice that in the floor there are various fossa and foramina, through which vessels and nerves travel. d. Base of ACF is the housing for the left and right frontal lobes. e. **The main way we get to the orbit, we drill through the floor of the ACF (later said that this was a manmade process). f. The MCF, on the left and right sides holds the left and right temporal lobes that sit right above your external ear. g. The PCF houses the brain stem and the cerebellum. h. In the ACF, one landmark is a spicule of bone that protrudes in a vertical plane called the crysta galli, or the cock of the cone (the cone of the cock is on a rooster’s head) the crysta galli is part of the ethmoid bone, you think more of them when you think of the ethmoid sinuses, but this is superior projection of that bone. i. Importantly, on either side of the crysta galli is a porus shelf called the Cribriform plate. It is porous or has holes in it so that the 1st cranial nerve can come up through the nasal cavity and enters the intercranium. The first cranial nerve has to do with smell. j. Posteriorly is a ridge of bone is called the lesser wing of the sphenoid. The sphenoid bone is fused between the ACF and PCF. Sphenoid means something that is wedged between two things. k. The lesser wing of the sphenoid is a landmark for the boundary between the ACF and the anterior part of the MCF. l. Posterior separation of the MCF is ridges called the petrus ridges. Petra means bone or rocky. Petrus ridge or bone is part of the temporal bone. Between the lesser wing of the sphenoid and the petrus is the MCF. m. Behind the petrus ridge on both sides is the PCF. n. In MCF, is a slit, just inferior to the lesser wing of the sphenoid, called the superior orbital fissure. The superior orbital fissure is important because it allows CNs to go into and out of the orbit. o. Optic nerve does not go through the superior orbital fissure to get to the orbit, but instead travels through the optic canal. It is a short canal, about 11 mm in length. It carries the optic nerve and a small branch that supplies the inside of the orbit called the ophthalmic artery. p. Posteriorly, an oval and rounded shaped foramen- the names are the foramen ovale and foramen rotundum. A branch of the trigeminal nerve will travel through the superior orbital fissure, a branch will travel through foramen rotundum, and one through the foramen ovale. One cranial nerve utilizes all of those defects in the floor of the cranial fossa. All in the floor of the MCF. q. SQ: What is the primary way to get to the oribit? The natural way is the superior orbital fissure and an unnaturally way is to drill out the floor. r. The PCF, some of the major foramina, the internal auditory meatus (for ex. the 7th and 8th CN travel in this canal). Another large defect is the jugular foramen. The jugular veins in the neck are named after this and three of the last four CNs travel through this foramen- 9, 10, and 11. IV. [S5] a. This shows the bones that make up the floor of the cranial fossae b. Sphenoid bone, lesser wings, greater wings, sphenoid bone in different locations in the body. The sphenoid bone is wedged here posteriorly by the occipital bone, laterally the temporal bone, the ethmoid, etc V. [S6] a. b. c. d. e. These are the same bones as the previous slide, but put back into anatomical position. Blue is the frontal bone that contributes to the forehead and the roof of the orbit or the floor of the ACF. Gray is the Ethmoid bone Yellow is the sphenoid bone with lesser and greater wing A lot of the formina of the MCF travel through the greater wing. For ex. foramen rotundum and ovale. Gross Anatomy: 1:00 - 2:00 Scribe: Teresa Kilborn Monday, January 12, 2009 Proof: Ashley Holladay Dr. Tubbs Cranial Cavity Page 2 of 7 f. The foramen spinosum, small foramen just posterior/lateral to the foramen ovale, transmits an important artery that will be talked about later. g. A psuedoforamen is a foramen that is formed with several bones come together leaving a tiny area for things to pass through as opposed to a normal foramen that goes through a single bone. An example is the foramen lacerin that is filled with cartilage in adulthood. What travels just above this is very important- the ICA. h. Petrus ridge i. Red is the temporal bone. j. Inside petrus bone are the small middle ear bones. (Ex. ear ossicles) k. Posteriorly, the blue is the occipital bone with the large foramen magnum which is the largest opening in the skull where the brain stem travels and becomes the spinal cord in essence. l. A divot or depression in the body of the sphenoid is the sella turcica that houses the pituitary gland m. An anterior clinoid process, a posterior clinoid process-they are some of the bones that make the cranial floor (skull base) n. ACF, MCF, and PCF VI. [S7] a. Rotate skull, looking from the feet up b. Occipital bone is gray with the foramen magnum and occipital condyles c. The sphenoid is the blue with two part pterygoid process- a medial and lateral plate d. 2 of the 4 muscles of mastication-muscles that move the jaw and allow you to chew, come off of the lateral plate. VII. [S8] a. Sagittal section through the midline b. Frontal bone contributing to ACF, as well as the Ethmoid bone with the crysta galli, you can see the lesser wing of the sphenoid. c. The temporal bone with the petrus ridge d. Occipital bone e. Foramen magnum is large defect in the occipital bone f. Hypoglossal canal- the 12th cranial nerve that makes the tongue move goes through this hypoglossal canal [near the foramen magnum] VIII. [S9] a. If you looked at the covering of the brain you would see the calvaria. Skull is designed to protect the brain and form the face. The calvaria is the covering of the brain b. Joints between bones in the skull are called sutures. They are fairly immotile. c. There are coronal, lambdoid, and sagittal sutures. IX. [S10] a. This is a fetal skull. b. Sutures have no fused yet so that the fetus’s head can squeeze out the birth canal by temporary deformation. c. By doing so, you are left with defects- anterior fontanel (diamond shaped) and posterior fontanel. These are often referred to as soft spots. When you feel these, you are actually feeling the pressure inside of the brain. X. [S11] a. Lateral surface of the fetal skull. b. Not all of the bones have fused yet. c. Some of the boney processes have not formed yet. One of which is the mastoid process that is behind the ear. The sternoclatomastoid muscle attaches to this. What happens is, sometimes, not being here it does not protect that part of the skull and there is a very important CN that exits the skull between the styloid process and what would be the mastoid process. As the OB is trying to pull a baby out of the birth canal, they use tongs that may puncture the facial nerve because the mastoid process is not there to protect it. If this happens, the baby could be born with facial palsy. XI. [S12] a. As the baby is starting to have molding of the cranium, he needs the bones of the calvaria to be mobile. b. Baby gets a cone-shaped head during delivery that comes back to a more natural shape afterwards. XII. [S13]- skip XIII. [S14] a. In lab, you’ll see that the floor is coated with a thick layer called the dura mater. There are 3 layers to the meninges: the outer dura, middle arachnoid, and the inner pia. The dura is the tougher of the three and coats the inside of the skull, thus it is not obvious where the foramina are. Also, there are structures that are traveling through and occluding the defects-the nerves, arteries, and veins- making them not visible. b. The floor of the ACF, if you were to chisel the bone away, is the orbit. Gross Anatomy: 1:00 - 2:00 Scribe: Teresa Kilborn Monday, January 12, 2009 Proof: Ashley Holladay Dr. Tubbs Cranial Cavity Page 3 of 7 c. There are several well defined venous structures that are closely related to the layers of the meninges called the dural venous sinuses. d. Anteriorly, not shown is the Cribriform plate which has 18-20 nerves coming from the nose. e. The optic nerves are filling the optic canal along with the ophthalmic artery which is a branch of the ICA. f. Posteriorly the pituitary gland sits in the sella turcica g. Further back is the superior orbital fissure. The 3rd, 4th, 6th, and the 1st part of the trigeminal nerve travel through the superior orbital fissure. h. The trigeminal nerve has 3 parts: i. 1st part- V1- ophthalmic nerve. Travels through the superior orbital fissure. ii. 2nd part-V2- maxillary nerve. Travels through the foramen rotundum. iii. 3rd part- V3- mandibular nerve. Travels through the foramen ovale. i. The trigeminal nerve proper is posterior to the ophthalmic division. j. Posterior/ laterally to the foramen ovale is the foramen spinosum, not seen very well. Blood vessels including the middle meningial artery come through this. The most common cause of a epidural hematoma is a laceration of the middle meningial artery that allows blood to accumulate outside of the dura mater. k. The internal auditory meatus with the 7th and 8th CN l. The jugular foramen- 9th , 10th , 11th and internal jugular vein come out the jugular foramen. m. Hypoglossal nerve through the hypoglossal canal. n. The base of the skull is a busy place- anyone who has had a basilar skull fracture where they sustained a large amount of force to the skull is likely to fracture on the base of the skull because fractures like to go through paths of least resistance so they like to travel through these areas that have foramen or holes already present. XIV. [S15] a. Olfactory nerves come through the cribriform plate. b. The optic nerves travel through the optic canal. c. 3,4,6, and V1 travel through the superior orbital fissure. d. V2 and V3 travel through the foramen rotundum and ovale respectively. e. 7 and 8 travel through the internal auditory meatus. f. 9, 10, 11 through the jugular foramen. g. Hypoglossal nerve through the hypoglossal canal. XV. [S16] a. The association of these cranial nerves b. Cross section through the ACF through the cribriform plate c. Small olfactory nerves d. One end of the olfactory nerves are sitting in the superior aspect of the nasal cavity waiting to smell something, then travel through the cribriform plate and synapse in the olfactory bulb and contract. e. Brain, frontal lobe and olfactory tract are just above the ACF floor. f. An injury that comes through the ACF floor in the region of the cribriform plate can disrupt smell by injuring the olfactory nerves and also if you puncture through the meninges then you have the possibility that the CSF that is coating the spinal cord and brain will leak through these little holes. Patients may come in after falling complaining that they can’t smell and clear fluid dripping out of their nose because their cribriform plate is incompetent. If you have CSF coming out, then you also have the possibility of bacteria going in. The possibility of getting meningitis is huge. XVI. [S17] a. The same three layers of meninges are located intercranially b. The exception is that the dura mater has 2 layers in the intercranium, unlike one layer in the spinal column c. Cross section: bone, Calveria, brain, the purple is the arachnoid, pia mater directly on the brain itself, above arachnoid is 2 layers of the dura mater one is snuggly on the inside of the bone of the skull-the periosteal layer or endosteal. d. The other layer that diverges away is the meningeal layer. e. Why have two layers? Because in various parts of the potential space is venous blood. When the venous blood is found between those two layers it is called a dura venous sinus, not to be confused with your periosteal air sinuses that have mucous in them. These are basically blood vessels that are specialized and on the inside is an endothelium just like any other blood vessel in the body. f. Rough estimation of how the dura venous sinuses are put together. They are pockets of venous blood. You have veins that are on the surface of the brain but the majority of blood from the inside of the skull will come back into the dura venous sinuses and leave the skull at its base. XVII. [S18] a. Schematic coronal section b. Outside of the skull layers with vessels, etc. Gross Anatomy: 1:00 - 2:00 Scribe: Teresa Kilborn Monday, January 12, 2009 Proof: Ashley Holladay Dr. Tubbs Cranial Cavity Page 4 of 7 c. Layer of veins that lie within 2 layers of the outer skull that we call the calveria. There is an outer table and an inner table, between the two is a type of marrow called the diploic space, communicating with veins just under your skin. d. Veins that come to and from the dura venous sinus. There is a connection between the dura venous sinus and the diploic space. Thus in turn, the intercranial dura venous sinuses can have access to the tissue just below the skin. These veins, called emissary veins, do not have vavles, thus, venuous blood flow will go either way. If the pressure is higher inside it goes out and if the pressure is higher outside then it goes in. If you get a skin lesion that gets infected (ex. pimple) that infection can gain access to the dura venous sinses and that can result in death. e. Blown up picture: dural venous sinus, emissary veins, diploic veins, the surface of the brain with the endosteal and meningeal layer of the dura. f. The specific dural venous sinus that is between the two layers of dura is called the superior venous sinus g. The inferior sagittal sinus runs between two leafs of the meningeal layer of dura mater. h. Arachnoid granulations – cauliflower like tuffs of arachnoid. They are the main way that you take CSF in the subarachnoid space back into the venous system for reuse. XVIII. [S19] XIX. Dura Mater [S20] a. Diploic veins b. In lab when you first look inside your skull, you’ll hopefully see part of the dura mater. c. Running on the top of the outer layer is the middle meningeal artery. XX. [S21] a. Shows grooves for vessels XXI. [S22] a. The middle meningeal artery is covered by a thin bone and if lacerated then it can result in an epidural hematoma- blood collection outside of the dura, but inside the skull. These are life threatening because the arteries continue to pump blood into the space causing the brain to shift away. Inside of the skull you can’t do a lot of shifting. XXII. [S23] a. Once you open the dura mater you’ll see the brain with surface vessels- arteries and veins. The larger veins will travel up and drain into the venous sinuses. Shown here is the superior sagittal sinus. These are called bridging veins. b. If you shock them violently then you would get venous rupture leading to a subdural hematoma- blood between the brain and the dura. More likely in elderly because their brain has atrophied allowing for more “rocking” room. These are chronic problems and are not associated as much with mortality XXIII. [S24]-skip XXIV. [S25] a. Sagittal section b. Some of the meningies form specialization, for example we’ve already talked about sinuses c. Septations can help divide d. One is the sickle shaped midline projection that runs from the crysta galli posteriorly called the falx cerebri (falx meaning sickle shaped). The left and right brain are divided partially by the falx cerebri e. Posteriorly, the cerebellum in the PCF will have a midline septum called the falx cerebelli, another specialization of dura mater. f. Tentorium cerebelli- horizontally oriented, covers the PCF, looks like tent under. Under which is the cerebellum and the brain stem that has been removed. XXV. [S26] a. Better view of the tentorium cerebelli b. The occipital lobe sits on the tentorium cerebelli and once you go below it you are in the PCF. c. The edge (sharp) of the tentorum cerebelli is called the incisura or the tentorial notch d. Sometimes you can have brain that is above the incisura that if it gets under high enough pressure then it can ooze down below that notch and compress nerves in the body ex. oculomotor nerve XXVI. [S27] a. Picture of the falx cerebri, PCF, Cerebellum, Brain stem XXVII. [S28] a. One very special intercranial dura sinus is the cavernous sinus. Between two layers of dura, the endosteal and meningeal layers. Just lateral to the body of the sphenoid. It’s unusual because it is the only venous structure in the body that you have an arterial vessel traveling through it- the ICA. There are also several CNs that travel through the cavernous sinus that are for the most part related to the orbit (3rd, 4th, 6th, V1 and V2). b. Pituitary (looks like an onion) sitting down in the sella turcica Gross Anatomy: 1:00 - 2:00 Scribe: Teresa Kilborn Monday, January 12, 2009 Proof: Ashley Holladay Dr. Tubbs Cranial Cavity Page 5 of 7 c. Dura specialization that forms a neck or collar around the pituitary gland is called the difermatic sella d. If you have a base or skull fracture where the ICA is lacerated then it will leak high pressure arterial blood into the cavernous sinus. Two of the big veins within the the orbit drain posteriorly into the sinus, but with a high pressure hose pumping arterial blood into the sinus the blood flow will be reversed and the two veins will receive arterial blood. One is above and one is below the eye ball. What you see in the patient is that their eyeball looks like it is coming in and out of the orbit with each heartbeat. This is called a carotid cavernous fistulaconnection between an artery and a vein in the venous sinus. What you see in the patient is called pulsatile exophthalmic that you can see more readily from the side of the patient. XXVIII. [S29] a. The brain in general does not have innervations b. If you can operate on someone and then get down to their brain and wake them up, they can’t feel that. c. What they do feel is the dura, it is very pain sensitive. There are a lot of nerves that serve the dura mater d. All of the dura of the anterior and medial fossa is innervated by the trigeminal nerve (all three parts) e. The PCF can be innervated by high cervical nerve branches as well as the 9th, 10th and even 7th CN. f. Meningitis is very painful because you irritate the dura XXIX. [S30]- skip XXX. [S31] a. Another example showing the profuse innervations of the dura XXXI. [S32] a. The dural venous sinuses have are gravity dependent, they have no valves. b. Their job is to get all of the intercranial blood back to the neck through the jugular veins. You’re collecting all of the venous blood through tributaries that are specialization of the dura and eventually to the jugular foramen that houses the internal jugular vein, or more specifically a dilation of that internal jugular vein called the superior jugular bulb. c. Increased flow through IJ’s when you have lying down. d. While standing, you have various other routes, ex. via spinal canal and its venous plexuses that bring blood back to the heart. XXXII. [S33] a. Name individually the dural venous sinuses: i. Cavernous venous sinus on either side of the sphenoid bone, it has profuse inter connections in between both sides of the pituitary b. One tributary into the cavernous venous sinus is the sphenopartital sinus that runs under the lesser wing of the sphenoid c. Superior ophthalmic vein- emissary vein that brings blood from the outside to the inside of the body, it is high pressure in the vein going to the eye that gives the pulsatile exophthalmus d. Veins that run on the top on bottom of the petrosal ridge- Superior and inferior petrosal e. The midline over the occipital and sphenoid bones is the basilar venous sinus f. Posteriorly, the attached edge of the tentorium cerebelli is a tranverse sinus on either side called the Superior sagittal sinus. It has a characteristic triangular shape (triangle at bottom) g. There is a straight sinus that runs between the falx cerebri and the tentorium cerebelli. h. A common output is a sigmoid sinus that has an s-shape. It drains into the jugular foramen where the internal jugular vein is. It is the last input to get that intercranial blood out. i. Tentorium cerebelli j. The confluence of sinuses is located where the transverse, superior sagittal, and occipital sinuses come together. k. Straight sinus, cavernous sinus, sphenoparietal, basilar venous sinus, superior petrosal, transverse, sigmoid XXXIII. [S34] a. Two sinuses not show on last slide: i. Occiptial venous sinus- runs on the midline on the internal aspect of the occipital bone and also contributes to the confluence ii. Marginal venous sinus- circular venous network that runs around the rim of the foramen magnum b. SQ: Does both the confluence and the superior sagittal sinus have a triangular shape? The superior sagittal sinus has a triangular shape, but the confluence does not. It is just where we see the transverse superior on one side, occipital, etc. coming together in an empty site. c. SQ: On the previous slide was that the superior sagittal sinus at the top? Yes, it runs from the crysta galli to the back of the head along the midlilne. d. SQ: Where are the petrosal veins in this picture? The inferior petrosal is just below the petrosal ridge and drains into the internal jugular vein and the superior petrosal is just above the petrosal ridge and it drains back into the transverse sinus. Gross Anatomy: 1:00 - 2:00 Scribe: Teresa Kilborn Monday, January 12, 2009 Proof: Ashley Holladay Dr. Tubbs Cranial Cavity Page 6 of 7 XXXIV. [S35] a. Sigmoid sinus has a characteristic s-shape b. Transverse sinus into superior petrosal, then sigmoid sinus and into the jugular vein. c. In neurosurgery, they will do a retrosigmoid craniotomy. The idea is that you make a hole into the skull and you stay way away from the cranial sinuses because if you make a cut into these sinuses then it bleeds profusely and it is very hard to stop. XXXV. [S36] a. Another view of the cranial venous sinuses. The superior sagittal sinus that runs back to the confluence. Inferior sagittal runs on the free margin of the falx cerebri. b. There is a big vein that drains structures from the lateral side of the brain stem, the mid brain and the deep surface of the brain called the great cerebral vein of galen which is one of the main tributaries into the straight sinus. c. Occipital sinus, Sigmoid sinus, Petrosal veins XXXVI. [S37] Covered everything in this image XXXVII. [S38] a. Two main tributaries into the great vein of galen which is itself a tributary to the straight sinus. XXXVIII. [S39] a. Cavernous sinus we went over already, remember the key things about this sinus is that it houses the ICA, which supply 2/3 of the blood supply to the brain b. Pituitary gland c. CN III travels through the cavernous sinus, CN IV, V1, and maybe V2, CN VI has the most medial projection and hugs the ICA as it travels through the venous sinus XXXIX. [S40] a. ICA makes a bend as it comes up into the skull b. Comes in through the carotid canal, starts vertically, takes horizontal turn, and then runs through the cavernous sinus shown in blue. c. The foramen lacerum, the ICA doesn’t run through it but as it takes its course, it is just above that area of fibrocartilage XL. [S41]- skipped XLI. [S42]- skipped XLII. [S43] a. Many of the blood vessels that are underneath the skin not only in the face but also back of the head have communications with other veins structures that then have communications with the venous sinuses b. For example, cavernous sinus is blue and if you have an infection in the subcutaneous tissue here it can spread through these pathways. One pathway called the pterygoid venous plexus. It can travel to the cavernous venous sinus and if you get an infection there, then the blood tends to clot which stops flow through that area, increasing intercranial pressure, and pinching the nerves and other structures in the area causing them not to work as well. c. Red arrows show the pathway that if you have an infection it can travel, for ex. the pterygoid venous plexus and into the cavernous sinus. XLIII. [S44] a. Read this, some of the direct communications. b. We said that the superior and inferior ophthalmic veins are basically emissary veins that run above and below the eyeball. They directly, and by the inferior ophthalmic, indirectly, drain into the cavernous sinus. c. The pterygoid venous plexus. XLIV. [S45] a. Area lateral to the nasal cavity, above the lip and below the eye called the danger zone or the triangle of danger. If you have an infection in this area then there is a very rich venous supply that can take it back into for example the valveless venous structures that lead to the pterygoid venous plexus and cavernous sinus. XLV. [S46] a. Venous sinuses, especially superior venouos sinus will allow the protrusion of arachnoid granulations. b. Allows CSF to percolate up into the arachonoid granulation and to be recycled back into the venous circulation XLVI. [S47] a. Found on the lateral surface of the venous sinus and tend to be more concentrated in lakes of blood called lateral lakes. XLVII. [S48] a. Circulation of CSF percolating into the depths of the brain, outside, and around the brain and spinal cord. Eventually it will come up to the granulations and make its way back to venous circulation. Gross Anatomy: 1:00 - 2:00 Scribe: Teresa Kilborn Monday, January 12, 2009 Proof: Ashley Holladay Dr. Tubbs Cranial Cavity Page 7 of 7 b. If you occlude the granulations with a blood clot from say trauma, they may not absorb as well and you develop too much fluid in the cavities of the brain- hydrocephalus. XLVIII. [S49] a. One treatment for hydrocephalus- bypass normal pathways of ventricular system, poke a hole in the floor of the brain and that allows CSF to come down through a new pathway. XLIX. [S50] a. The blood supply of the brain b. 1/3 comes from left and right vertebral arteries and 2/3 from left and right ICA c. They fuse at the base of the brain and form the circle of willis d. The circle of willis is a back up mechanism that allows for stenosis due to disease while still having retrograde flow because of the circular pattern. L. [S51] a. Look at on your own b. Vertebrals are the main posterior inferior supply. c. ICA with elaborate connection between them that sends blood to various parts of the brain. d. Unfortunately up to 20%-25% of the population doesn’t have good enough collateral connections to sustain the brain if you were to occlude either the right or left ICA thus they’d have a stroke on whatever side you occlude. LI. [S52] [End 49:27]