Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
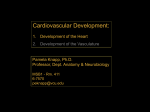
Update in Radiology Anatomical variations of septum pellucidum P. Sartori*, V. Anaya, Y. Montenegro, M. Cayo and G. Barba Computed Tomography and Magnetic Resonance Imaging Department, EDES, Hospital Español, Ciudad Autónoma de Buenos Aires, Argentina Abstract Septum Pellucidum is a thin medial septum of triangular shape that consists of two nervous laminae that are attached and located between the corpus callosum and the fornix. Anatomical variations of septum pellucidum appear during fetal life in the ventro-dorsal position. These variations are: cavum septi pellucidi, cavum vergae and cavum veli interpositi. The presence or absence of these cavities can be related to the presence of nervous system or neuropsychiatric dysfunction, therefore they should be well known to avoid wrong diagnoses © 2014 Sociedad Argentina de Radiología. Published by Elsevier Spain, S.L.U. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). Keywords: Septum pellucidum; Cavum septum pellucidum; Cavum vergae; Cavum vellum interpositum Introduction During intrauterine life, there are normal midline cavities which usually persist in adulthood and should not be confused with pathological entities. It is important to know them, as they may may be related to concomitant neurological or neuropsychological diseases. In this article, we review the septum pellucidum (SP) and its anatomical variations. In Latin, the word septum (saepire) means fence or partition wall, while pellucidum or perlucidum means translucent. Thus, SP (or lucidum) is a thin medial septum of triangular shape that consists of two nervous laminae that are attached and located between the corpus callosum and the fornix (fig. 1)1-5. In 1966, Andy and Stephen called it “telencephalic septum” (septum telencephali) 6. Boundaries are described in table 11,4-6. The SP serves as a relay station, containing fibers that connect with hippocampus and the hypothalamus2. Complete absence of the SP occurs in 2 to 3 individuals per 100 000 people, being a predictor of brain abnormalities, such as: septooptic dysplasia, corpus callosum abnormalities, holoprosencephaly, lissencephaly or Chiari malformation6,7. During intrauterine life, there are three potential cavities in the midline between the lateral ventricles. These cavities regress between the seventh month of fetal life and the second year of postnatal life, but some may persist in adulthood8,9. These cavities, first described in the year 1600, include: cavum septum pellucidum (CSP), cavum vergae (CV) and cavum veli 80 Rev. Argent. Radiol. 2015;79(2): 80-85 interpositi (CVI). They occur with a prevalence of 0.14%8-10. It is important to highlight that these cavities are in direct contact with the subarachnoid space, but they do not communicate with or are considered part of the ventricular system. As these cavities are not lined with ependyma or choroid plexus cells, they do not produce cerebrospinal fluid (CSF)3,9-11. 1) Cavum septum pellucidum: it is also known as cavum septi pellucidi, the ventricle of the septum or fifth ventricle (fig. 2)3,8,10,12. It can be found in all fetuses at 36 weeks’ gestation and persists in 36% of full-term infants, only 6% of them persist after the six month of live3,4,11-13. It is significantly more common in women3. CSP is part of normal development. As from 12 weeks of gestational age, the corpus callosum starts to develop from the lamina terminalis as a fiber bundle that connects the two hemispheres, also originating the SP. The space between the two laminae that are not fused, located between the frontal horns of the lateral ventricles and anterior to the foramen of Monro is called CSP (fig. 3)10,11,14. A number of theories have been proposed for the origin of CSP, but it is thought that during embryo-fetal development, the mass of cells occupying the space of the SP is involved in the development of the commissural plate. Selective elimination of this group of cells would lead (by necrosis) to the molecular concentration of large amounts of amino acids, which would attract fluids to achieve a balance in the oncotic pressure of the plate. Fluid pressure would be responsible for P. Sartori et al. the formation of CSP12. However, it has also been hypothesized that this entity may originate during infancy, as a result of repeated shaking, when rocking infants vigorously in an attempt to soothe them12. CSP is a triangular space between the two laminae of the septum pellucidum (its boundaries are detailed in table 2)3,4,8,10,12,13,15,16. CSP may occur in isolation or in association with cavum vergae, communicating with the latter through the aqueductus caudae septi or aqueductus ventriculii vergae7,8. CSP is an important marker for the evaluation of normal development of the fetal neural axis. Absence of the CSP is rarely an isolated finding, as nonvisualization of the CSP on ultrasound (US) or magnetic resonance imaging (MRI) scans in fetal life is associated with brain malformations, such as holoprosencephaly, septo-optic dysplasia, agenesis of the corpus callosum, Alexander disease, tuberous sclerosis, phakomatosis, pinealoma, trisomy 21 and schizencephaly3,10,12,14,16. Considering embryonic development, CSP may not occur without the development of the corpus callosum; therefore agenesis of the corpus callosum is always associated with agenesis of the SP3,4. There are US studies in which CSP has been identified in 100% of fetuses between 18 and 37 weeks’ gestation, and in 79% of fetuses between 30 and 41 weeks’ gestation; in newborns, complete posterior closure has been seen in 97%, so the CSP is present when the cavum vergae is absent16. Hence, visualization of the CSP between 18 and 20 weeks’ gestation implies normal development of the brain16. In patients with schizophrenia or in aggressive, alcoholic individuals or people with neurological development disorders, there is a higher prevalence of enlarged CSP3-5,11,14,15,17,18. It was De Greef who first reported an association between CSP and schizophrenia11. Some authors report an association between boxing and the presence of CSP due to repeated brain trauma. An association between CSP and posttraumatic stress disorders has also been reported, in the military population currently participating in war conflicts or in veterans of wars2,3,5,12,13,15,17. There are various classifications for CSP. Based on whether the CSP communicates with the lateral ventricles through fenestrations, it may be classified as communicating or noncommunicating (more common)2,13. However, another classification focuses on asymptomatic (communicating or non- Table 1: Boundaries of the septum pellucidum. BoundaryStructure SUPERIOR Inferior surface of the body of corpus callosum ANTEROINFERIOR Superior surface of the genu of corpus callosum POSTEROINFERIOR Corpus and columns of the fornix Figure 1 Axial T2-weighted magnetic resonance imaging of the brain demonstrating normal appearance of the septum pellucidum (lucidum) (arrow). LATERAL Medial wall of frontal horns of lateral ventricles MEDIAL Virtual space with contralateral septum Figure 2 Sketch of axial and sagittal views of the cavum septum pellucidum. Rev. Argent. Radiol. 2015;79(2): 80-85 81 Anatomical variations of septum pellucidum communicating CSP) and symptomatic (non-communicating CSP) characteristics; the latter may be simple, not complicated or complicated by brain injuries12. 2) Cavum vergae: Andrea Verga, an italian anatomist described it in 1851. Iit is also known as cavum fornicis, cavum psalterii, Verga´s ventricle, the ventricle of Strambio, ventriculus triangularis or sixth ventricle10,12,13. Cavum vergae is the posterior extension of CSP, extending as far as the posterior columns of the fornix and the foramen of Monro (fig. 4)9,10,13. It is triangular in shape (its boundaries are listed in table 3)4,5,10,13. Cavum vergae begins to develop by the 5th month of gestation and disappears by two months of age 10. CV is present in 30% of normal newborns, subsequently regressing and disappearing13. The incidence of CV was 2.3% in 1032 brains studied, and it is important to highlight that it is almost always found in association with CSP7,9,10,13 When the CSP is dilated, the CV is also dilated, as they join through a defect of the fornix, which is not in contact with the corpus callosum10 (fig. 5). Some authors report a higher prevalence of enlarged CSP or CV in patients with schizophrenia10. 3) Cavum velum interpositum (CVI) was first described by Kruse and Schaetz in 19309,10. It is also known as cisterna interventricularis, ventriculi tertii, transverse fissure or subtrigonal fissure9. The incidence of CVI ranges, according to various authors, between 21 and 34%, and persistence in postnatal life is rare, being 30% in 1-10 year-old children, with no significant differences between genders9. CVI is a subarachnoid cistern arising as an extension of the cisterna magna and which originates from the roof plate of the diencephalo, protruding into the primitive neural tube approximately during the third fetal month. CVI is a normal Table 2: Boundaries of the cavum septum pellucidum. BoundaryStructure ANTERIOR Genu of corpus callosum POSTERIOR Corpus and columns of the fornix SUPERIOR Inferior border of the body of corpus callosum INFERIOR Rostrum of the corpus callosum and anterior white commissure LATERAL Laminae of septum pellucidum Table 3: Boundaries of the cavum vergae.. BoundaryStructure ANTERIOR Crus of the fornix POSTERIOR Body of the corpus callosum SUPERIOR Splenium of the corpus callosum INFERIOR Hippocampal commissure and psalterium (lyra davidis) Figure 3 Axial T1-weighted magnetic resonance of the brain demonstrating the presence of a triangular cavity between the frontal horns of the lateral ventricles, known as cavum septum pellucidum (arrowhead). 82 Rev. Argent. Radiol. 2015;79(2): 80-85 Figure 4 Sketch of axial and sagittal views of the cavum septum pellucidum associated with the cavum vergae. P. Sartori et al. Figure 5 Axial T2-weighted magnetic resonance of the brain demonstrating a cavity filled with cerebrospinal fluid and interposed between the lateral ventricles (asterisk). The finding is consistent with cavum septum pellucidum associated with cavum vergae. Figure 7 FLAIR axial magnetic resonance imaging of the brain showing a triangular cavity cephalic to the fornix, between the lateral ventricles, called cavum velum interpositum (arrowhead). Table 4: Boundaries of the cavum velum interpositum. BoundaryStructure SUPERIOR Figure 6 Sketch of axial and sagittal view of the cavum velum interpositum. cavity in the development of the brain9,10 (fig. 6) and its presence has not been associated with neuropsychiatric disorders or dysfunction of the limbic system19. CVI is a triangular cavity of dorsal base located in the choroidal fissure (fig. 7). The boundaries of CVI are detailed in table4 4,9,10,13,19,20. It is important do distinguish CVI from CV. One of the main features is the fact that CV always coexists with CSP, but these entities can also be differentiated by the location of the internal cerebral veins, as CV lies above these veins, whereas CVI encloses them. Corpus callosum (lower border) and hipoccampal commissure INFERIOR Tela choroidea of the third ventricle and thalamus LATERAL Crus of the fornix ANTERIOR Foramen of Monro POSTERIOR Pineal region INFEROLATERAL Internal cerebral veins CVI should also be differentiated from an arachnoid cyst of the quadrigeminal cistern or from a pineal cyst. The latter lies inferiorly to the internal cerebral arteries9,19. Rev. Argent. Radiol. 2015;79(2): 80-85 83 Anatomical variations of septum pellucidum Conclusion It is important to recognize anatomical variations of the septum pellucidum so that they may not be wrongly diagnosed as interhemispheric cystic lesions, whether before or after birth. Recognition of such variations during fetal life serves as a predictor for the detection of brain malformations or behavior disorders. Conflicts of interest The authors declare no conflicts of interest. Figure 8 Coronal fetal ultrasound showing the cavum septum pellucidum (asterisk). Imaging diagnosis of SP and variants Prenatal diagnosis is made by transabdominal ultrasound and, in the case of cephalic presentation, transvaginal ultrasound allows better visualization of its variants (fig. 8)10. The columns of the fornix should be differentiated from a CSP to avoid making mistakes, and the same applies to enlarged CSP in the presence of CV, when the latter laterally displaces the CSP leaflets mimicking an absent CSP14,17. Differential diagnosis for an enlarged CSP include vein of Galen aneurysm (which is diagnosed by color Doppler technology with knowledge of the anatomy of the region), arachnoid cyst and dilated third ventricle (distinguished by its location between the thalami)14. In the fetus, CSP and CV can be seen by US and MRI, although the latter may replace US in cases of maternal obesity and olighohydramnios3,5,14,21. MRI has the advantage of delineating the pineal gland with respect to the quadrigeminal cistern or pineal cysts, differentiating such cysts from CVI21. The anterior extension of the CVI is best displayed on axial T2-weighted MR images, while the posterior extension of the CVI can be seen as an anechoic inverted helmet-like structure on US scans (the convex side of this helmet is formed by the internal cerebral veins). Differential diagnosis is made on the basis of the position of the internal cerebral veins, as arachnoid cysts compress the tectum towards the brain and displace the internal cerebral veins upward against the splenium of the corpus callosum (which differentiates them from the CVI)21. 84 Rev. Argent. Radiol. 2015;79(2): 80-85 References 1. Lo Vuolo M. Doppler color venoso: miembros inferiores y pelvis. Buenos Aires: Journal; 2008. 2. Eklof B, Perrin M, Delis KT, Rutherford RB, Gloviczki P, et al., American Venous Forum. Updated terminology of chronic venous disorders: The VEIN-TERM transatlantic interdisciplinary consensus document. J Vasc Surg. 2009;49: 498---501. 3. Marinello Ponentes J, Calvo J, Vila R, Lapiedra O. Insuficiencia venosa crónica. Conceptos actuales. Anales de Cirugía Cardíaca y Vascular. 2004;10:96---143. 4. Eklöf B, Rutherford RB, Bergan JJ, Carpentier PH, Gloviczki P, Kistner RL, et al. Revision of the CEAP classification for chronic venous disorders: Consensus statement. J Vasc Surg. 2004;40:1248---52. 5. Bauer G. The aetiology of leg ulcers and their treatment by resection of the popliteal veins. J Int Chir. 1948;8:937---67. 6. Browse NL, Burnand KG, Wilson N, Irvine A. Diseases of the veins. London: Edward Arnold; 1998. 7. Paolinelli P. Ultrasonido Doppler de extremidades inferiores para el estudio de la insuficiencia venosa. Rev Chil Radiol. 2009;15:181---9. 8. Nigro JA, Méndez Flores A, Nigro MB. Correlación: sintomatología - signología clínica con eco-Doppler. Vascular - clasificados según Ceap. Flebología y Linfología. Lecturas vasculares. 2012;7:1048---58. 9. Polak JF. Doppler: cuello y extremidades. Madrid: Marbán; 2007. 10. Caggiati A, Bergan JJ, Gloviczki P, Eklof B, Allegra C, Partsch H, et al. Nomenclature of the veins of the lower limb: extensions, refinements, and clinical application. J Vasc Surg. 2005;41:719---24. 11. Segura JA. Interpretación de la hemodinamia venosa con eco-Doppler. Flebología y Linfología Lecturas Vasculares. 2006;1:58---67. 12. Segura JA. Iinterpretación de la hemodinamia venosa con eco-Doppler. Flebología y Linfología Lecturas Vasculares. 2007;2:206---20. 13. Schadeck M. Duplex and Phlebology. Napoli: Gnocchi; 1994. 14. Juan Samsó J, Fontcuberta García J, Senín Fernández ME, Vila Coll R. Guía básica para el diagnóstico no invasivo de la insuficiencia venosa. Capítulo de Diagnóstico Vascular No Invasivo de la Sociedad Espa˜nola de Angiología y Cirugía Vascular. Angiología. 2002;54:44---56. 15. Selfa S, Diago T, Ricart M, Chuliá R, Martín F. Insuficiencia venosa crónica primaria de los miembros inferiores. Valoración prequirúrgica con ecografía Doppler duplex color. Radiología. 2000;42:343---8. 16. Coleridge-Smith P, Labropoulos N, Partsch H, Myers K, Nicolaides A, Cavezzi A. Duplex Ultrasound investigation of the veins in chronic venous disease of the lower limbs –UIP consensus document. Part I. Basic principles. Eur J Vasc Endovasc Surg. 2006;31:83---92. P. Sartori et al. 17. Gómez C, Jiménez H, Ulloa JH. Nomenclatura de las venas de los miembros inferiores y términos en flebología: los consensos internacionales. Rev Colomb Cir. 2012;27:139---45. 18. Anonymous. Diagnosis and treatment of venous ulceration. Lancet. 1982;2:247---8. 19. Kistner RL. Primary venous valve incompetence of the leg. Am J Surg. 1980;140:218---24. 20. Eriksson I, Almgren B. Surgical reconstruction of incompetent deep vein valves. Ups J Med Sci. 1988;93:139---43. 21. Gloor B, Largiader J. Surgical treatment of deep venous reflux. Eur J Vasc Endovasc Surg. 1997;13:98---100. Rev. Argent. Radiol. 2015;79(2): 80-85 85