Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
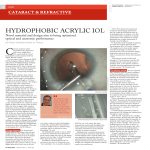
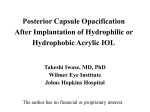
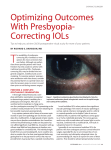
LABORATORY SCIENCE Double-C loop platform in combination with hydrophobic and hydrophilic acrylic intraocular lens materials Dimitriya Bozukova, PhD, Liliana Werner, MD, PhD, Nick Mamalis, MD, PhD, Laure Gobin, PhD, Christophe Pagnoulle, PhD, Anne Floyd, MD, PhD, Erica Liu, MD, PhD, Shannon Stallings, MD, PhD, Caleb Morris, MD, PhD PURPOSE: To analyze the behavior of a new double-C-loop quadripod symmetrical intraocular lens (IOL) platform combined with a hydrophilic lens material and a new hydrophobic glistening-free acrylic lens material, Ankoris and Podeye, respectively, in silico (computer simulation), in vitro (laboratory investigation), and in vivo (rabbit model). SETTING: John A. Moran Eye Center, University of Utah, Salt Lake City, Utah, USA, and Physiol S.A., Liege, Belgium. DESIGN: Experimental study. METHODS: An in silico simulation investigation was performed using finite elements software, an in vitro investigation according to the International Organization for Standardization (ISO119793:2012), and an in vivo implantation in a rabbit model with 4 weeks of follow-up. Postmortem data were collected by Miyake-Apple gross examination and histopathologic analyses. Biocompatibility and IOL centration were tested. RESULTS: Both IOLs demonstrated statistically insignificant variations in posterior and anterior capsule opacification and Soemmerring ring formation. They were well biotolerated with no signs of toxicity, inflammation, or neovascularization. Axial and centration stability were noted in vitro and in vivo as a result of significant contact between surrounding tissues and haptics and the posterior portion of the optic. CONCLUSION: The results suggest suitability of the double-C loop IOL platform for the manufacturing of premium (ie, multifocal, toric, and multifocal toric) IOLs. Financial Disclosure: Drs. Bozukova, Gobin, and Pagnoulle are employees of Physiol S.A., Liege, Belgium. Dr. Pagnoulle has a proprietary interest in the tested intraocular lenses. No other author has a financial or proprietary interest in any material or method mentioned. J Cataract Refract Surg 2015; 41:1490–1502 Q 2015 ASCRS and ESCRS Numerous investigations to evaluate the biomechanical stability of intraocular lenses (IOLs) have been done. Some evaluate the biocompatibility of the lens material.1–5 Others emphasize the influence of the design on the degree of posterior capsule opacification (PCO)6–11 and lens biomechanical stability.12,13 Early studies reported that hydrophobic acrylic materials are associated with lower PCO rates as a result of lens epithelial cell (LEC) regression after approximately 1 month of implantation regardless of the IOL design.2 Later studies demonstrated the 1490 Q 2015 ASCRS and ESCRS Published by Elsevier Inc. importance of a sharp posterior lens optic edge as a major factor limiting the PCO rate.8,9 Rabbit studies demonstrated that cell migration was prevented by intimate mechanical contact between the sharp optic edge and the capsular bag. A 5-year clinical study compared the neodymium: YAG (Nd:YAG) laser capsulotomy rates with 2 hydrophobic acrylic IOLs with a sharp optic edge and a round optic edge and a hydrophilic acrylic IOL with a sharp optic edge.14 The results suggested that the combination of a sharp optic edge and a hydrophobic http://dx.doi.org/10.1016/j.jcrs.2014.10.042 0886-3350 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS acrylic material was the most appropriate choice for preventing optically significant PCO. Contradictory results have been reported,6–11 probably due to differences in the geometries of the analyzed square edges. This further confuses the situation, and the surgeon’s choice becomes even more difficult, especially when premium IOLs are concerned because their optical performance can be highly affected by undesirable cell proliferation and/ or lens misalignment. Indeed, abundant cellular proliferation or axial shift of the optic may lead to loss of visual acuity, which can be particularly deleterious with multifocal IOLs.15 Recently, Hirnschall et al.6 reported a 3-year randomized trial of a plate-haptic IOL and a 3-piece open-loop haptic toric IOL made of the same material. The IOLs had comparable PCO rates and capsular bag stability. The latest studies assessed the effect of both lens material and lens optic design on the biocompatibility, optic centration, and rotational and axial stability of IOLs, particularly premium ones (eg, multifocal, toric, and multifocal toric).6,14,16 For instance, Chang16 compared a silicone plate-haptic IOL with a hydrophobic acrylic C-loop model and reported better rotational stability of the hydrophobic C-loop version. Other authors have reported the results of singlemodel clinical investigations of the biomechanical stability of toric IOLs.17–19 The results indicate that silicone plate-haptic IOLs are prone to rotate by 5.56 degrees G 8.49 (SD),19 whereas hydrophobic acrylic C-loop IOLs manifest rotation levels in the range of 3.2 G 2.8 degrees.17 However, it would be speculative to conclude that the design or the material is a determinant for this result. Intrinsically, a C-loop design might be prone to rotate more easily in the direction opposite the haptic orientation. However, contrary to plate haptics, they provide more contact with the surrounding tissues.20 Recently, a new double-C-loop IOL (Physiol S.A.), combining the advantages of C-loop haptics and a symmetrical platform, was investigated clinically in its hydrophilic acrylic version. Ninety-one patients 1491 (117 eyes) were included in the study, which reported an absolute rotation of 2.5 G 2.06 degrees 12 months after implantation. The present study evaluated this IOL platform in combination with a generic hydrophilic acrylic material or a proprietary hydrophobic acrylic glisteningfree material (Physiol S.A.21–23) using in silico (computer simulation), in vitro (laboratory investigation), and in vivo (rabbit model) conditions. To our knowledge, the results of these 3 investigational methods are being presented for the first time. Biomechanical parameters are discussed in parallel with data related to the capsular and uveal biocompatibility of the test IOLs. MATERIALS AND METHODS Intraocular Lenses Podeye is a monofocal aspheric IOL manufactured from a hydrophobic acrylic glistening-free material (GF, Physiol S.A.). Ankoris (technical name POD T, Physiol S.A.) is a monofocal toric aspheric IOL manufactured from a hydrophilic acrylic material with a water uptake of 26%. Both IOLs contain ultraviolet and blue-light filters (proprietary formula from Physiol S.A., WO2006074843 used for the hydrophilic acrylic material24) and are double-C-loop quadripodes (Figure 1). The IOLs have an overall diameter of 11.4 mm, an optic diameter of 6.0 mm, and anteroposterior angulation of 5 degrees. The power of the tested IOLs was C23.5 diopters (D), and the tested toric IOLs had a cylinder of 1.5 D. In Silico Evaluation Finite Elements Numerical Simulation Numerical simulation of the biomechanical behavior of the IOLs was performed by the finite element method using Samcef Samtech software (Siemens). The Young modulus and the geometry of the IOLs were introduced as key parameters. The IOL mechanics were evaluated for different compression diameters simulating different capsular bag sizes for 2 conditions: “backed-up,” approximating the situation with an intact capsule, and “free,” approximating the situation after Nd:YAG PCO treatment when the posterior capsule was no longer intact. Radial compression forces were measured at the horizontal plane; axial compression forces (Case 1) and axial shift (Case 2) were measured at the vertical plane (Figure 2). Gravity was not considered. In Vitro Evaluation Young Modulus The elasticity (Young) modulus of sample Submitted: March 6, 2014. Final revision submitted: October 9, 2014. Accepted: October 13, 2014. From Physiol S.A. (Bozukova, Gobin, Pagnoulle), Liege, Belgium; the John A. Moran Eye Center (Werner, Mamalis, Floyd, Liu, Stallings, Morris), University of Utah, Salt Lake City, Utah, USA. Corresponding author: Dimitriya Bozukova, PhD, Physiol S.A., Allee des Noisetiers 4, 4031 Liege, Belgium. E-mail: d.bozukova@ physiol.be. disks of 3.0 mm thickness and 6.0 mm in diameter from the test and reference materials were tested with Instron 5566 and a static load cell of 500 N. The reference materials were tested in their equilibrated state (conditioned in a physiologic medium similar to the aqueous humor) after processing, packaging, and sterilization similar to the IOLs. Compression at a constant rate of advancement of the load cell of 0.5 mm/min was applied. The data were interpreted with Bluehill 2 software (Instron). The measurement was performed in triplicate, and the mean values were used for interpretation. J CATARACT REFRACT SURG - VOL 41, JULY 2015 1492 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS Figure 1. Design of the hydrophobic and hydrophilic IOLs. Scanning Electron Microscopy The optic edges of the dry IOLs were analyzed by scanning electron microscopy (SEM) (JSM 840A, Jeol Ltd). Confocal Microscopy The topography of the IOL optic periphery was analyzed using a 3-dimensional optical profiler confocal microscope (Sensofar PLU Neox, objective 20). Haptic Compression ForceLRadial Compression Force (FR) The force applied by the haptics to the capsular bag is important for IOL rotational and refractive stability and may have some effect on its resistance to PCO. The force was determined with a compression force tester (MFC1385-IOL, O&O mdc Ltd.); the possible value variation was less than 0.2% (method validation). Before the measurement, the equipment was calibrated according to the standard manufacturer’s procedure. Intraocular lenses in their original packaging state (1 per IOL model) were placed between the 2 jaws, and the compression force, in milligrams force, was measured for well diameters of 10.0 mm and 9.5 mm corresponding to various capsular bag sizes. In all cases, measurements were taken 30 seconds after haptic compression to give the haptic material time to relax. Ten samples per IOL model were tested. Median standard deviations (SDs) were calculated. The test was performed in accordance with the procedure recommended by the International Organization for Standardization (ISO) 11979-3.25 Axial Shift in Compression (Z) On compression, the haptics of the IOLs may deform differently and, therefore, the IOL optic may or may not remain at the initial position, moving forward or backward along the optical axis. Determining the axial shift experimentally aims at estimating the capability of the IOL haptics to compensate for capsular bag size variations and enable a stable anteroposterior IOL position, referred to as the effective lens position (ELP). This displacement was measured in air at 20 C G 2 C for all tested IOL models (1 per IOL model) in their original packaging state (hydrated or dried). The IOLs were placed in wells of 10.0 mm and 9.5 mm. Ten samples per IOL model were tested. The axial shift was determined using an optical comparator Figure 2. Representation of the 2 cases used for the finite elements numerical simulation. Line with dashes represents the posterior capsular bag (FR Z axial compression force; FR Z radial compression force; Z Z axial shift). with a precision of G 0.001 mm according to the procedure described by ISO 11979-3.25 Angle of Haptic Contact or Degree of Haptic Contact The angle of haptic contact is a measured approximation of the total haptic contact with the supporting ocular tissue. A high angle of haptic contact is associated with high interface between the IOL and tissue, with a higher friction force impeding IOL rotation. The angle of haptic contact was measured in vitro according to the procedure recommended by ISO 11979-3.25 Briefly, the IOL in its equilibrated state was positioned in test wells with an overall diameter of 10.0 mm and 9.5 mm. An image per condition was collected by optical microscopy (XLI Cap software, Optica), and the angle of haptic contact was then determined as the angle between the points where the clearance between the loop and well wall was 0.25 mm. A measuring device with an accuracy of 0.5 degrees was used. Ten samples per IOL model were tested. The result per IOL is presented as the sum of the angle of haptic contact measured for the 4 haptics. Optic Decentration (DX) Decentration of the IOL optic with respect to the optical axis may be deleterious for visual acuity because the IOL will no longer be in the optimum position. Decentration was measured in vitro according to the procedure recommended by ISO 11979-3.25 The setup from the angle of haptic contact test was used, and the optic decentration was measured as the distance between the optic center and the center of the traced circle corresponding to the test well diameter. Ten samples per IOL model were tested. In Vivo Evaluation Five New Zealand white rabbits of the same sex and weighing between 2.4 kg and 3.2 kg were acquired from approved vendors in accordance with the requirements of the Animal Welfare Act for use in this study. An extra rabbit was also ordered in case 1 of the study animals died. The animals were numbered consecutively from 1 to 6. They were housed and cared for at the animal facility of the John A. Moran Eye Center, University of Utah, Salt Lake City, J CATARACT REFRACT SURG - VOL 41, JULY 2015 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS Utah, USA. All rabbits were treated in accordance with the guidelines of the Association for Research in Vision and Ophthalmology, the Animal Welfare Act, and the Institute for Laboratory Animal Research. The animals were quarantined for at least 7 days prior to the beginning of the study. Their eyes were grossly checked for the presence of anomalies before the surgical procedures. The examination (performed by the same surgeon) was unremarkable in all eyes. The hydrophobic IOL was implanted in the right eye of the rabbits and the hydrophilic IOL in the left eye. The surgical procedures were performed by the same surgeon (N.M.) using the Universal S3 OPMI 6-CFC, XY surgical microscope (Carl Zeiss Meditec AG). Surgical Technique Each animal was prepared for surgery by pupil dilation with cyclopentolate hydrochloride 1.0% and phenylephrine 2.5% drops, applied topically approximately every 5 minutes for 15 minutes. A drop of gatifloxacin (Zymaxid) was also applied topically approximately every 5 minutes for 15 minutes. Anesthesia was achieved with an intramuscular injection of ketamine hydrochloride (50 mg/kg) and xylazine (7 mg/kg) in a mixture of 7:1. One drop of topical proparacaine hydrochloride was also placed in each eye before surgery. Eye movement and animal respiration were monitored intraoperatively to ensure that adequate levels of anesthesia were maintained. Supplemental anesthetics were given intramuscularly as needed during the surgery. The area around the eye was draped in an aseptic manner. A lid speculum was placed to retract the lids. One drop of povidone–iodine 5.0% (Betadine) as well as 1 drop of gatifloxacin were placed on the surface of the eye just before the surgery began. Using an aseptic technique and a surgical microscope, a fornix-based conjunctival flap was fashioned. A corneoscleral incision was then made using a crescent blade, and the anterior chamber was entered with a 3.0 mm keratome. A capsulorhexis forceps was used to create a well-centered continuous curvilinear capsulotomy (CCC) with a diameter of approximately 5.0 mm; this was followed by hydrodissection. One milliliter of epinephrine 1:1000 and 0.5 mL of heparin (10 000 USP units/mL) were added to each 500 mL of irrigation solution to facilitate pupil dilation and control inflammation. The endocapsular technique was used with the phacoemulsification performed entirely within the capsular bag. The residual cortex was then removed with the irrigation/aspiration (I/A) handpiece. An ophthalmic viscosurgical device (OVD) (sodium hyaluronate 1.6% [Amvisc Plus]) was used to expand the capsular bag, and the IOLs were inserted into the capsular bag using the recommended injection system (Medicel Accuject 2.2). The IOLs were loaded into the injector using an OVD (Physiovisc Integral, Physiol S.A.). After the IOLs were injected, their position inside the capsular bag was noted in clock hours according to the position of the toric marks (the site where the loops connect to the optic in the case of the nontoric design). The OVD was removed using the phaco handpiece primarily and then using the I/A handpiece. The wound was closed with a 10-0 monofilament nylon suture. Combination antibiotics and steroid ointment (neomycin polymyxin B sulfates dexamethasone) was applied to the eyes following surgery. The same ointment was placed in the eyes 4 times daily for the first postoperative week. It was discontinued after 1 week. In the second postoperative week, each animal received topical prednisolone acetate eyedrops 4 times daily. It was discontinued after the second week. 1493 Slitlamp Examination The eyes were evaluated grossly at day 1. Slitlamp examination with scoring for ocular inflammatory response was performed 1, 2, 3, and 4 weeks postoperatively (G 2 days), and photographs were taken as deemed necessary. At each examination, the rabbit eyes were dilated using a combination of cyclopentolate hydrochloride and phenylephrine hydrochloride solutions. A standard scoring method in 11 specific categories was used at each examination, including assessment of corneal edema as well as the presence of cell and flare in the anterior chamber. The slitlamp scoring system used was a modification of McDonald-Shadduck26 scoring. Retroillumination images with the pupil fully dilated were obtained for photographic documentation of CCC size, anterior capsule opacification (ACO), PCO, and any observed capsule fibrosis.27,28 The position of the IOL optic–haptic junction was followed with respect to the suture and noted in clock hours at each examination to roughtly evaluate the IOL rotation. Gross Examination After the clinical examination at 4 weeks, the animals were anesthetized using a 1 to 2 cc intramuscular injection of a 7:1 mixture of ketamine hydrochloride and xylazine and then humanely killed with a 1 mL intravenous injection of pentobarbital sodium/phenytoin sodium. The globes were enucleated and placed in 10% neutral buffered formalin for at least 24 hours. They were then bisected coronally just anterior to the equator. Gross examination and photographs from the posterior aspect (Miyake-Apple view) were performed to assess the ACO and PCO development as well as the IOL fixation. The extent and severity of ACO and PCO were scored on a scale from 0 (none) to 4 (severe).9,28 Gross photographs were taken using a camera (model D40 with an AF Micro Nikkor 55 mm 1:2.8 lens, Nikon Corp.) mounted on an MP4 Land camera (Polaroid). They were analyzed with the BX40 microscope (Olympus Optical Co., Ltd.). Photomicrographs were taken with a microscope digital camera (model P20) mounted with a U-TV0.5C-3 C-mount video port (Olympus Optical Co., Ltd.) attached to the light microscope for photodocumentation. Histology After gross examination and photographs, all globes were sectioned and the anterior segments including the capsular bags were processed for standard light microscopy and stained with hematoxylin–eosin. Features such as cell type, extent, and route of growth were documented by serial photomicrographs. Capsular Bag Size, Optic Decentration, Angle of Haptic– Tissue Contact The methods for in vitro evaluation were applied; however, the gross examination images were used. The IOL optic diameter was used for scaling. To enhance comprehension, results of a similar nature but obtained by different test methods are presented and discussed together and treated as laboratory data. Statistical Analysis Descriptive statistics were used for all objective measurements with the mean and SD. For qualitative grading with ordinal scales, the median is presented with the confidence interval (CI). For paired tests, both parametric and nonparametric statistical analyses were performed. The conventional way to perform analyses on paired data comprises the J CATARACT REFRACT SURG - VOL 41, JULY 2015 1494 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS following 2 steps: (1) Determine whether the paired differences are normally distributed via the KolmogorovSmirnov test. (2) If the Kolmogorov-Smirnov test is significant, indicating that the distribution of the differences is not normal, a Wilcoxon (nonparametric test) paired test is performed. If the Kolmogorov-Smirnov test is not significant, indicating that the distribution of the differences is normal, a paired t test is performed. Because there are fewer than 12 observations (as a general rule), the results of the paired Wilcoxon nonparametric tests of the collected data are presented. The variability of the experimental laboratory results is related to the method variability. All comparisons of laboratory measurement with simulated outcomes are purely empirical, and statistical analyses were not performed. The in silico results were obtained by finite element simulation, based on the mean value obtained for the elasticity (Young) modulus for both IOL materials. Because no randomization is required for finite element simulations, the outcomes are the same with any given run. Therefore, statistical comparison is impossible. The discrepancy between measured outcomes and simulated outcomes was evaluated for the sake of comparison only. RESULTS Microscopic Observation In Vitro Both IOLs were analyzed by confocal, optical, and SEM, and the profiles were compared with the theoretical profiles. They both had sharp-edged optics posteriorly and anteriorly (Figure 3). Because they are manufactured by a lathing/milling process, traces of the manufacturing tool are seen peripherally (Figure 3, A-II). The profiles observed by SEM (Figure 3, BI-II) are identical to the theoretical profiles (Figure 3, CI-II). A supplementary edge is designed at the optic–haptic junction to further impede cellular proliferation. Elasticity Modulus In Vitro The measured elasticity modulus of the 26% hydrophilic acrylic material (3.911 G 0.045 MPa) was lower than that of the hydrophobic acrylic counterpart (5.829 G 0.036 MPa). A similar trend was seen for the constraints applied by the materials at 10% and 20% of deformation, 0.342 G 0.005 MPa and 0.697 G 0.008 MPas for the hydrophilic material and 0.522 G 0.006 MPas and 1.164 G 0.010 MPas for the hydrophobic material, respectively. Radial Compression Force In Silico and In Vitro Lower in silico or in vitro simulated capsular bag diameters induced higher radial compression forces (Table 1). The radial compression forces simulated numerically for the hydrophilic IOL were slightly lower than those simulated for the hydrophobic IOL. This is a direct consequence of the introduced Young modulus values. For the hydrophilic IOL, the radial compression forces estimated in silico for a hypothetic capsular bag diameter of 10.0 mm were comparable to those obtained in vitro for both backed-up and free conditions. With the lower test diameter of 9.5 mm, the values obtained in vitro were slightly lower than those obtained in silico. For the hydrophobic IOL, the experimental results were systematically lower than the Figure 3. Comparison of confocal (A) and SEM (B) results for the theoretical designs (C) of the hydrophilic IOL (series I) and hydrophobic IOL (series II). J CATARACT REFRACT SURG - VOL 41, JULY 2015 1495 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS Table 1. Axial shift and radial compression forces measured at in silico and in vitro conditions. Radial Compression Force (mg) Test Condition In silico Ø 10.0 mm backed up Ø 10.0 mm free Ø 9.5 mm backed up Ø 9.5 mm free In vitro Ø 10.0 mm average Ø 10.0 mm SD Ø 9.5 mm average Ø 9.5 mm SD Axial Shift (mm) Hydrophobic Hydrophilic Hydrophobic Hydrophilic 157 165 252 249 105 111 169 171 d 0.073 d 0.122 d 0.073 d 0.122 72 7 117 9 88 46 100 21 0.029 0.016 0.061 0.013 0.089 0.013 0.110 0.014 Ø Z diameter computer-generated results, with higher discrepancies observed between the in vitro data and in silico data (Table 1). Vertical Compression Forces and Axial Shift In Silico and In Vitro Two parameters were measured on the axis vertical to the IOL optic plane: the vertical compression force applied by the optic and the optic axial shift. The first parameter was determined in silico, and the second was determined in silico and in vitro. As with the radial compression forces, the hydrophobic acrylic IOL in silico presented slightly higher vertical compression than the hydrophilic acrylic IOL related to the higher Young modulus introduced (Table 1). Meanwhile, the numerically estimated axial shift was the same for both IOLs. Experimentally, the hydrophobic IOL shifted less than the hydrophilic IOL. This difference was statistically significant (P value Z 0.0124 and .0004 at 10.0 mm and 9.5 mm simulated capsular bag size, respectively; 2-tailed paired t test). The vaulting angulation and the posterior capsular bag in vivo may be limiting factors in terms of axial shift. In in silico and in vitro conditions, a lower simulated capsular bag size generally induced higher axial shift no matter which IOL material was used. For a 10.0 mm simulated capsular bag diameter, vertical compression forces of 26.8 mg and 18.0 mg were calculated in silico for the hydrophobic IOL and the hydrophilic IOL, respectively. Reducing the capsular bag size to 9.5 mm resulted in a hypothetically increased force of 38.5 mg and 25.9 mg, respectively. Implantation Procedure in Rabbits The injection of all IOLs was well controlled. In some eyes, the IOL was fully injected in the capsular bag; in other eyes, 1 of the trailing loops was injected out of the bag but was easily placed in the bag with a hook. In rabbit 2, left eye (hydrophilic IOL), 1 trailing loop was caught in the injector and torn. Because of this, it was decided to include the extra rabbit, implanting the hydrophobic IOL in the right eye and the hydrophilic IOL in the left eye. Rabbit 2 was kept throughout the followup period to study the effect of the broken loop on IOL stability. The surgeon reported that a harder push was generally necessary to implant the hydrophobic IOL because of the higher Young modulus of the IOL material. At the end of the surgical procedure, the capsulorhexis was found to cover the optic periphery of the IOLs for 360 degrees in all cases. The surgical incision was located at 12 o’clock in all eyes, and all IOLs were oriented with the major axis along the 6 o’clock to 12 o’clock meridian. Slitlamp Examination At 1 day, corneal edema limited to the incision site was generally found in all eyes, which were otherwise unremarkable. Signs of a postoperative inflammatory reaction were very mild in all eyes; a few eyes in both groups had fibrin formation noted at the 1-week examination, but it had almost disappeared by the 2-week examination. Blood was noted in the anterior segment in eye 6, right eye, at the 1-week examination (likely from the incision site), and a small amount was present in front of the IOL at the end of the clinical follow-up. Starting at the 2-week examination, many eyes in both groups exhibited proliferative cortex material/pearls originating from the Soemmerring ring protruding anteriorly to the IOL; this began at the optic–haptic junctions and caused synechiae in some cases. Soemmerring ring formation breached the capsular bend, and LECs migrated behind the IOL. J CATARACT REFRACT SURG - VOL 41, JULY 2015 1496 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS Figure 4. Slitlamp examination images at 4 weeks in rabbit 1. A: Right eye (hydrophobic IOL). B: Left eye (hydrophilic IOL). Central PCO was absent at this point, but a mild degree of PCO was observed at the 3-week examination, increasing in intensity by the 4-week examination (generally beginning at the optic–haptic junctions in both IOL groups) (Figure 4). No statistically significant difference was observed between the groups, and the PCO scores at 4 weeks were as follows: hydrophobic IOL, 96.9% CI, 0.5-3.0; hydrophilic IOL, 96.9% CI, 0.5-2.0 (P Z 1.000, Wilcoxon paired test). A mild degree of ACO was observed in some eyes in both IOL groups but was not statistically significantly different between the 2 groups (P Z .072, Wilcoxon paired test). Both IOLs were well biotolerated with no statistically significant difference between groups in inflammatory deposits (P Z 1.000, Wilcoxon paired test), limbal vascularization (P Z 1.000, Wilcoxon paired test), iris vascularization (P Z .346, Wilcoxon paired test), or posterior synechiae (P Z .850, Wilcoxon paired test) (Figure 5). Zero levels of conjunctival injection, conjunctival discharge, corneal opacity, aqueous flare, and IOL decentration were observed at the same time point. The results for both IOLs showed no statistically significant difference for the investigated parameters (Table 2). Flare was practically undetectable because signs of postoperative inflammatory reaction were mild in all eyes, with fibrin formation noted in a few eyes at the 1-week examination and in none of the eyes at the 2-week examination. Rough assessment of rotational stability throughout the study showed no severe IOL rotation in either group. The optic–haptic junctions remained at the same positions relative to the sutures (expressed in clock hours). Figure 5. Slitlamp examination scores. The rectangles represent the 25th and 75th percentiles. The thick lines represent the median values. The whiskers represent the maximum and minimum values excluding outliers. The open circles represent the outliers. Scale is from 0 (no) to 4 (severe). Total score refers to the sum (limbal vascularization C iris vascularization C posterior synechiae C inflammatory deposits C PCO C ACO) for each animal (ACO Z anterior capsule opacification; PCO Z posterior capsule opacification). J CATARACT REFRACT SURG - VOL 41, JULY 2015 1497 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS Table 2. Calculated rabbit capsular bag size and in vitro and in vivo optic decentration. In Vivo Calculated Rabbit Eye ID Hydrophobic IOL 1 OD 2 OD 3 OD 4 OD 5 OD 6 OD Mean SD Hydrophilic IOL 1 OD 2 OD 3 OD 4 OD 5 OD 6 OD Mean SD In Vitro Optic Decentration at ø 10.0 mm In Vitro Optic Decentration at ø 9.5 mm Decentration (%) ø mm Rabbit Capsule Mean SD Mean SD 2.33 3.83 3.50 2.67 1.83 1.33 2.58 0.96 9.57 9.35 10.03 9.83 9.59 9.68 9.68 0.23 1.38 d d d d d d d 1.09 d d d d d d d 1.02 d d d d d d d 1.16 d d d d d d d 2.33 5.33 4.33 4.67 3.67 2.67 3.83 1.17 9.6 9.61 9.86 9.78 9.44 9.07 9.55 0.31 1.31 d d d d d d d 0.77 d d d d d d d 1.44 d d d d d d d 0.67 d d d d d d d ø Z diameter; IOL Z intraocular lens Gross Examination The scores for central PCO (P Z .93, Wilcoxon paired test), peripheral PCO (P Z .93, Wilcoxon paired test), and Soemmerring ring formation intensity (P Z 1.0, Wilcoxon paired test) multiplied by the Soemmerring ring area (P Z .34, Wilcoxon paired test) are shown in Figure 6. Some PCO was observed centrally and peripherally starting at the optic–haptic junctions in 75% of cases, but the between-group difference was not statistically significant (Figure 7). Mild degrees of ACO (hydrophobic IOL: median Z 1 and 96.9% CI, 0.5-1.0; hydrophilic IOL: median Z 0.5 and 96.9% CI, 0-1) were also detected in both groups. No IOL tilt and no IOL decentration were observed (including rabbit 2, left eye, which had a broken loop). All IOLs were fixated inside the capsular bag. Soemmerring rings were observed mainly anteriorly or at the level of the haptics, suggesting posterior lens/capsular bend formation as a result of the 5-degree angulation. The variation in capsulorhexis coverage of the optic periphery was not statistically significant given the standard variation rate (P Z .93, Wilcoxon paired test) (hydrophobic IOL: 96.9% CI, 60-280; hydrophilic IOL: 96.9% CI, 100-280). All cross-correlation coefficients were lower than 0.05, indicating no relationship or a poor relationship between capsulorhexis coverage and other parameters (Figures 6 and 7). Histopathologic Analysis Representative microscopic images of the histopathologic investigation are shown in Figure 8. The histopathologic findings were similar in both IOLs, with no significant difference between the right eyes and left eyes. All rabbit eyes showed a moderate amount of proliferative cortical material in the fornix forming a Soemmerring ring. The material proliferating on the anterior surface of the IOL varied from trace to a large amount of material. In several rabbits, the anterior cortical material extended onto the pupillary space, but there was no statistically significant difference between the groups. Similarly, based on a qualitative estimation, the posterior capsule proliferation of cortical material ranged from trace to a moderate amount with no statistically significant betweengroup difference. There was no sign of untoward inflammation or toxicity in any rabbit eye (Figure 8). Calculated Rabbit Capsular Bag Table 2 shows the results for these parameters. A rabbit capsular bag diameter of 9.07 to 10.03 mm was calculated based on the gross examination images obtained by the MiyakeApple technique. Based on the same images, the mean optic decentration relative to the optic diameter was calculated; it was 2.58% G 0.96% for the hydrophobic In Vitro and In Vivo Optic Decentration (DX) J CATARACT REFRACT SURG - VOL 41, JULY 2015 1498 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS Figure 6. Gross examination scores. The rectangles represent the 25th and 75th percentiles. The thick lines represent the median values. The whiskers represent the maximum and minimum values excluding outliers. The open circles represent the outliers. Scale is from 0 (no) to 4 (severe). Total score refers to the sum (central PCO C peripheral PCO C SRI C Soemmerring ring area C ACO) for each animal. The capsulorhexis is expressed as value 102 (ACO Z anterior capsule opacification; CR Z capsulorhexis; IOL Z intraocular lens; PCO Z posterior capsule opacification; SRA Z Soemmerring ring area; SRI Z Soemmerring ring intensity). IOL and 3.83% G 1.17% for the hydrophilic IOL (P Z .003, 2-tailed paired t test). These values are slightly higher than those obtained with an in vitro model (P ! .001 at both 9.5 mm and 10.0 mm well diameters; 2-tailed paired t test). Given the SDs for the 2 conditions, this variation is not considered significant. Moreover, it is close to the precision of the measurement technique. All these values are largely lower than the tolerance limits acceptable by the current ISO standard. A degree of zero decentration was estimated by the ophthalmologic examiner (L.W.) during clinical examination, suggesting unnoticeable decentration levels. The IOL that had 1 damaged trailing haptic (rabbit 2, left eye) presented with slightly higher calculated optic decentration in vivo, but this remained clinically unnoticeable (Table 2). In Vitro and In Vivo Angle of Haptics Contact To obtain comparable results, in vitro test well diameters of 9.5 mm and 10.0 mm were compared with the measured in vivo rabbit capsular bag sizes 9.07 to 10.03 mm (Table 2). The tendency was for the angle of haptic contact to increase as the test well size or rabbit capsular bag size decreased (Figure 9). The measured angle of haptic contact was the same Figure 7. Gross postmortem examination images in rabbit 1. (A) Right eye (hydrophobic IOL). (B) Left eye (hydrophilic IOL). J CATARACT REFRACT SURG - VOL 41, JULY 2015 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS 1499 Figure 8. Images from histopathologic examinations (PCO Z posterior capsule opacification; Philic Z hydrophilic; Phobic Z hydrophobic). for other similar conditions regardless of the IOL materials. The in vivo results were quite similar to the measured in vitro results with the 9.5 mm test well diameter, which is in line with the measured mean rabbit capsular bag size, 9.68 mm for the right eyes and 9.55 mm for the left eyes. The variations were relatively small for all conditions, 104 to 134 degrees of capsule contact for the hydrophilic IOL and 104 to 129 degrees for the hydrophobic IOL (Figure 9). DISCUSSION The tested double-C-loop platform provides a symmetrical quadripod design with 2 by 2 oppositely Figure 9. Angle of haptic contact measured under in vitro and in vivo conditions (Ø Z diameter). oriented haptics. This haptic orientation provides 4 contact points for fixation of the IOL in the capsular bag. The IOL optic has a sharp edge, which limits cellular migration at the posterior lens–capsule interface and prevents PCO formation.10 Hence, the obtained microscopic images of the edge corresponded to the edge in the theoretical model. The magnitude of the measured Young modulus is considerably low and argues for good foldability of both IOL materials during injection and good recovery of shape and optical properties after injection.23 Very strong radial or vertical haptic compression forces may induce capsule ovaling, stretch, or even damage, while low radial compression forces may result in poor IOL stability.23 These parameters depend on the IOL material and design, capsular bag size, and elasticity. Small capsule diameters, more elastic materials, and nonflexible haptics may provoke stronger compression forces in both directions. The measured Young modulus is slightly higher for the hydrophobic acrylic material. The Young modulus was used as a basic parameter for the numerical simulation and, therefore, slightly higher compression forces were estimated in silico for the hydrophobic IOL than for the hydrophilic IOL. The computer-simulated radial compression forces were generally higher than those measured in vitro, probably due to the absence of gravity as a parameter in the in silico investigation. Another reason may be the constant Young modulus considered in silico and J CATARACT REFRACT SURG - VOL 41, JULY 2015 1500 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS the limit of elasticity. Meanwhile, partial drying of the IOL during the period of the in vitro measurement may change the elasticity. Moreover, finite element simulation does not consider the relaxation processes that occur in the IOL material on compression and is based on purely elastic deformation. This explains the difference between in silico and in vitro results for the hydrophobic IOL, which is known to have significant plasticity.23 In contrast, the hydrophilic material is elastic and results, therefore, in similar in vitro and in silico results. Considering the large SD measured in vitro for the radial compression force applied by the hydrophilic IOL, the trend observed for the hydrophobic IOL can be considered similar to that observed for the hydrophilic IOL. The same conclusion stands for the experimental axial shift results. Although the difference between the axial shifts of the 2 IOLs experimentally was statistically significant, it is orders of magnitude lower than that measured for the Envista MX60 (Bausch & Lomb), Acri.Tec 366D (Carl Zeiss Meditec), and Sensar AR40E (Abbott Medical Optics) IOLs.23 This suggests that anteroposterior stability of the IOL may be expected clinically, ensuring the refractive stability of both IOLs in this study (Podeye and Ankoris). Higher radial than vertical compression forces obtained in silico for both IOLs suggest that capsular bag size compensation at the plane parallel to the IOL optic is better than compensation at the perpendicular plane. It can be explained by the ergonomic design of the haptics, which provides relaxation within the optic plane of the IOL. This improves the ELP of the IOL for better refractive predictability. Rabbit histopathologic investigation demonstrated contact between the posterior optic surface and the capsule. In the case of the hydrophobic acrylic IOL, this may support the formation of the IOL–capsule junction through physical or biological adhesion. With the hydrophilic acrylic IOL, the posterior material–capsule contact is expected to impede cell migration and PCO formation. The calculated rabbit capsular bag size postmortem was slightly lower than that reported in the scientific literature for this animal model.29 This may be due to different factors such as the rabbit age, weight, or the measuring technique used. Also, the eyes had been fixated in formalin, and tissue shrinkage likely occurred. This parameter was not a subject of investigation in the present study and was used only for comparative purposes. However, the calculated value is comparable to typical human capsular bag diameters29 and the results obtained by this animal model are therefore an indication of clinical behavior. Low decentration levels were calculated in vitro and in vivo. Moreover, they remained undetectable to the ophthalmologic examiner (L.W.) and were rated as zero decentration. This demonstrates the radial stability of the tested IOL design regardless of the material and is in accord with the results from the radial and vertical compression force measurements. Both IOLs were well biotolerated, and no toxicity, inflammation, or neovascularization was observed. Given the reactivity of the rabbit model, it is difficult to interpret the IOL material behavior in terms of PCO, ACO, and Soemmerring ring formation.30 These parameters are in direct relationship with protein secretion and epithelial cell proliferation.31 Indeed, some PCO was detected during the slitlamp examination and later on postmortem gross examination by the Miyake-Apple technique. The PCO scores are comparable to those reported for other hydrophobic acrylic IOLs.8,9 Because the tested hydrophobic acrylic IOL is made of bioadhesive material,22 it is expected that clinically, firm contact between the IOL and the posterior capsule will occur. Indeed, a clinical investigation performed recently with this IOL confirmed this expectation, and the results will be published soon. The degree of haptic contact in vivo and in vitro (at 9.5 mm test well diameter) was similar relative to the reproducibility and reliability of the results. More than a 100-degree angle of contact was measured systematically, which suggests sufficient haptic–tissue interface and friction. Indeed, a higher degree of haptic contact is associated with stronger material/tissue friction and would be beneficial in preventing the IOL from rotating and misaligning. According to the comparison of rabbit and human ocular parameters presented in the literature,29 the human eye has a slightly lower capsular bag diameter than the rabbit eye. Therefore, it is suggested that in clinical cases, the angle of haptic contact will be similar to or higher than the values measured in the present study. Although 1 haptic of 1 of the tested hydrophilic IOLs (rabbit 2, left eye) was broken accidentally during implantation, the IOL remained centered in the eye. It is assumed that even if a haptic were damaged accidentally, the remaining functional haptics would enable the IOL to position as a conventional asymmetric open-C-loop IOL. This intended micromechanical effect further enhances the IOL design safety, and the present case is an indication for that. In conclusion, this study is the first demonstration of the reproducibility of data obtained in silico, in vitro, and in vivo for a new double-C-loop symmetric platform manufactured in hydrophilic and hydrophobic acrylic materials. Both IOLs were well biotolerated and safe for patients, with no sign of toxicity or inflammation. Given the reactivity of the selected animal J CATARACT REFRACT SURG - VOL 41, JULY 2015 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS model, it is understandable that some PCO, ACO, and Soemmerring rings were observed. Both IOLs also demonstrated resilience to decentration as a result of sufficient contact and friction between the surrounding tissues and the IOL material. Results suggest that the double-C-loop platform is a suitable carrier of premium optics (multifocal and toric) regardless of the IOL material. WHAT WAS KNOWN The material and design are known to be factors in the postoperative behavior of an IOL. When inappropriately selected, they might cause complications related to their biomechanical stability and biocompatibility. Premium (multifocal and toric) IOLs are sensitive to rotation, decentration, axial displacement, and PCO. WHAT THIS PAPER ADDS The double-C-loop symmetric quadripod platform naturally provided the IOL with axial and centration stability regardless of the IOL material. In combination with appropriately selected IOL material, it is a suitable candidate for special optic IOLs. REFERENCES 1. Heatley CJ, Spalton DJ, Kumar A, Jose R, Boyce J, Bender LE. Comparison of posterior capsule opacification rates between hydrophilic and hydrophobic single-piece acrylic intraocular lenses. J Cataract Refract Surg 2005; 31:718–724 2. Hollick EJ, Spalton DJ, Ursell PG, Pande MV. Lens epithelial cell regression on the posterior capsule with different intraocular lens materials. Br J Ophthalmol 1998; 82:1182–1188. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1722372/pdf/ v082p01182.pdf. Accessed March 27, 2015 3. Hayashi K, Hayashi H. Posterior capsule opacification after implantation of a hydrogel intraocular lens. Br J Ophthalmol 2004; 88:182–185. Available at: http://www.ncbi.nlm.nih.gov/pmc/ articles/PMC1771981/pdf/bjo08800182.pdf. Accessed March 27, 2015 4. Werner L. Biocompatibility of intraocular lens materials. Curr Opin Ophthalmol 2008; 19:41–49 €m C. Posterior 5. Kugelberg M, Wejde G, Jayaram H, Zetterstro capsule opacification after implantation of a hydrophilic or a hydrophobic acrylic intraocular lens; one-year follow-up. J Cataract Refract Surg 2006; 32:1627–1631 6. Hirnschall N, Nishi Y, Crnej A, Koshy J, Gangwani V, Maurino V, Findl O. Capsular bag stability and posterior capsule opacification of a plate-haptic design microincision cataract surgery intraocular lens: 3-years results of a randomized trial. Br J Ophthalmol 2013; 97:1565–1568 7. Prinz A, Vecsei-Marlovits PV, Sonderhof D, Irsigler P, Findl O, Weingessel B. Comparison of posterior capsule opacification between a 1-piece and a 3-piece microincision intraocular lens. Br J Ophthalmol 2013; 97:18–22 1501 8. Werner L, Mamalis N, Pandey SK, Izak AM, Nilson CD, Davis BL, Weight C, Apple DJ. Posterior capsule opacification in rabbit eyes implanted with hydrophilic acrylic intraocular lenses with enhanced square edge. J Cataract Refract Surg 2004; 30:2403–2409 9. Werner L, Mamalis N, Izak AM, Pandey SK, Davis BL, Nilson CD, Weight C, Apple DJ. Posterior capsule opacification in rabbit eyes implanted with 1-piece and 3-piece hydrophobic acrylic intraocular lenses. J Cataract Refract Surg 2005; 31:805–811 10. Morgan-Warren PJ, Smith JMA. Intraocular lens edge-design and material factors contributing to posterior-capsulotomy rates: comparing Hoya FY60AD, PY60AD, and Acrysof SN60WF. Clin Ophthalmol 2013; 7:1661–1667. Available at: http://www.ncbi. nlm.nih.gov/pmc/articles/PMC3755701/pdf/opth-7-1661.pdf. Accessed March 27, 2015 11. Schauersberger J, Amon M, Kruger A, Abela C, Schild G, Kolodjaschna J. Lens epithelial cell outgrowth on 3 types of intraocular lenses. J Cataract Refract Surg 2001; 27:850–854 12. Visser N, Bauer NJC, Nuijts RMMA. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg 2013; 39:624–637 13. Chassain C, Pagnoulle C, Gobin L, Rozema J. Evaluation d’une nouvelle plateforme d’implant intraoculaire: centrage et stabilite rotatoire [Evaluation of a new intraocular lens platform: centration and rotational stability]. J Fr Ophtalmol 2013; 36:336–342 14. Johansson B. Clinical consequences of acrylic intraocular lens material and design: Nd:YAG-laser capsulotomy rates in 3 x 300 eyes 5 years after phacoemulsification. Br J Ophthalmol 2010; 94:450–455. Available at: http://www.ncbi.nlm.nih. gov/pmc/articles/PMC2976308/pdf/bjo166181.pdf. Accessed March 27, 2015 15. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg 2009; 35:992–997 16. Chang DF. Comparative rotational stability of single-piece openloop acrylic and plate-haptic silicone toric intraocular lenses. J Cataract Refract Surg 2008; 34:1842–1847 17. Visser N, Ruız-Mesa R, Pastor F, Bauer NJC, Nuijts RMMA, s-Mico R. Cataract surgery with toric intraocular lens imMonte plantation in patients with high corneal astigmatism. J Cataract Refract Surg 2011; 37:1403–1410 18. De Silva DJ, Ramkissoon YD, Bloom PA. Evaluation of a toric intraocular lens with a Z-haptic. J Cataract Refract Surg 2006; 32:1492–1498 19. Chang DF. Early rotational stability of the longer Staar toric intraocular lens; fifty consecutive cases. J Cataract Refract Surg 2003; 29:935–940 20. Buckhurst PJ, Wolffsohn JS, Davies LN, Naroo SA. Surgical correction of astigmatism during cataract surgery. Clin Exp Optom 2010; 93:409–418 21. Pagnoulle C, Nolet De Brauwere Van Steeland M, inventors, PhysIOL, assignee. Polymer composition for an intraocular lens Patent WO2006/063994, December 13, 2005; Available at: http://www.wipo.int/patentscope/search/en/WO2006063994. http://www.google.bj/patents/WO2006063994A1?clZen. Accessed March 27, 2015 22. Pagnoulle C, Bozukova D, Gobin L, Bertrand V, Gillet-De Pauw M-C. Assessment of new-generation glistening-free hydrophobic acrylic intraocular lens material. J Cataract Refract Surg 2012; 38:1271–1277 ro ^me C. Biomechanical and optical 23. Bozukova D, Pagnoulle C, Je properties of 2 new hydrophobic platforms for intraocular lenses. J Cataract Refract Surg 2013; 39:1404–1414 J CATARACT REFRACT SURG - VOL 41, JULY 2015 1502 LABORATORY SCIENCE: DOUBLE-C-LOOP COMBINED WITH HYDROPHOBIC AND HYDROPHILIC ACRYLIC IOLS 24. Pagnoulle C, Nolet De Brauwere Van Steeland M, inventors, PhysIOL, assignee. Yellow chromophore agent composition for intraocular lenses and thus obtainable lenses Patent WO2006074843, December 6, 2005; Available at: http://www. google.com.na/patents/WO2006074843A1?clZen. Accessed March 27, 2015 25. International Organization for Standardization. Ophthalmic Implants – Intraocular Lenses – Part 3: Mechanical Properties and Test Methods. Geneva, Switzerland, ISO, 2012; (ISO 11979–3:2012) 26. McDonald TO, Shadduck JA. Eye irritation. In: Marzulli FN, Maibach HI, eds, Dermatotoxicology and Pharmacology (Advances in Modern Toxicology, volume 4). Washington, DC, Hemisphere Publishing, 1977; 139–191 27. Nishi O, Nishi K. Preventing posterior capsule opacification by creating a discontinuous sharp bend in the capsule. J Cataract Refract Surg 1999; 25:521–526 28. Werner L, Pandey SK, Apple DJ, Escobar-Gomez M, McLendon L, Macky TA. Anterior capsule opacification; correlation of pathologic findings with clinical sequelae. Ophthalmology 2001; 108:1675–1681 29. Gwon A. The rabbit in cataract/IOL surgery. In: Tsonis PA, ed, Animal Models in Eye Research. San Diego, CA, Elsevier/Academic Press, 2008; 184–204 30. Wormstone IM, Wang L, Liu CSC. Posterior capsule opacification. Exp Eye Res 2009; 88:257–269 31. Hyon JY, Yeo HE. Rotational stability of a single-piece hydrophobic acrylic intraocular lens during removal of ophthalmic viscosurgical devices. Am J Ophthalmol 2010; 149: 253–257 J CATARACT REFRACT SURG - VOL 41, JULY 2015 First author: Dimitriya Bozukova, PhD Physiol S.A., Liege, Belgium