Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
JACC Vol. 26, No. 3
September 1995:815-25
815
Mechanical and Metabolic Functions in Pig Hearts After 4 Days of
Chronic Coronary Stenosis
A. J A M E S L I E D T K E , MD, FACC, B R I T T A R E N S T R O M , PnD, S T E P H E N H. NELLIS, PHD,
J E N N I F E R L. HALL, MS, W I L L I A M C. STANLEY, PHD
Madison, Wisconsin
Objectives. This study sought to evaluate the functional and metabolic consequences of imposing a chronic external coronary
stenosis around the left anterior descending coronary artery for 4
days in an intact pig model.
Background. A clinical condition termed hibernating myocardium has been described wherein as a result of chronic sustained
or intermittent coronary hypoperfusion, heart muscle minimizes
energy demands by decreasing mechanical function and thus
avoids cell death. The use of chronic animal models to simulate
this disorder may assist in establishing causative associations
among determinants to explain this phenomenon.
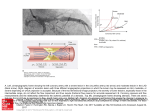
Methods. A hydraulic cuff oceluder was placed around the left
anterior descending coronary artery in eight pigs. Coronary flow
velocity was reduced by a mean (-+SE) of 49 -+ 5% of prestenotic
values, as estimated by a Doppler velocity probe. After 4 days the pigs
were prepared with extracorporeal coronary circulation and evaluated at flow conditions dictated by the cuff' occluder. Substrate
utilizations were described using equilibrium labeling with
[u-t4C]paimitate and [5-3H]glucose. Results were compared with a
combined group of 21 acute and chronic (4 day) sham animals.
Results. Four days of partial coronary stenosis significantly
decreased regional systolic shortening by 54%. Myocardial oxygen
consumption was maintained at aerobic levels, and rest coronary
flows were normal. Fatty acid oxidation was decreased by 43%
below composite sham values, and exogenous glucose utilization
was increased severalfold. Alterations in myocardial metabolism
were accompanied by a decline in tissue content of adenosine
triphosphate.
Conclusions. These data suggest that chronic coronary stenosis
in the absence of macroscarring imparts an impairment in
mechanical function, whereas coronary flow and myocardial oxygen consumption are preserved at rest. The increases in glycolytic
flux of exogenous glucose are similar to observations on glucose
uptake assessed by fluorine-18 2-deoxy-2-fluoro-D-glucose in patients with advanced coronary artery disease. We speculate that
intermittent episodes of ischemia and reperfusion are the cause of
this phenomenon.
(J Am CoU Cardiol 1995;26:815-25)
Previous evidence from cardiac catheterization data (1,2) indicated that in some patients with coronary artery disease, left
ventricular dysfunctionwas not the result of myocardial infarction
but of impaired contraction in otherwise viable tissue whose
function could in part be revived by appropriate stimuli. Rahimtoola (3) expanded on these observations when in 1984 he
described in a series of patients with coronary artery disease,
Imaging studies conducted at about the same time and later,
presumably in comparable groups of patients, documented a
peculiar metabolic abnormality characterized by a marked
increase in exogenous glucose utilization when normalized by
perfusion (i.e., the "flow-metabolic mismatch" [4-8]) while at
the same time retaining the capacity of oxidative metabolism
(9). The presence of increased glucose metabolism has served
as a reliable clinical marker to successfully predict contractile
recovery after revascularization (10-12).
The coronary flow stimulus responsible for chronic downregulation of mechanical performance in otherwise noninfarcted
myocardium is unknown. The original hypothesis of sustained,
chronic hypoperfusion is under debate and has now been broadened to include other combinations of intermittent or sustained
hypoperfusion sufficient to blunt coronary reactive hyperemia
(13). One line of evidence developed in recent animal studies (14)
indicated that a progressive decline in mechanical function occurred at normal rest coronary blood flows, suggesting a cumulative effect of myocardial stunning secondary to repetitive bouts
of unwitnessed ischemia followed by aerobic reperfusion. Metabolic data were not acquired in these studies.
At issue remains the relative absence of established chronic
a state of persistentlyimpaired myocardialand left ventricular
function at rest due to reduced coronaryblood flowthat can be
partially or completely restored to normal if the myocardial
oxygen supply/'demandrelationship is favorablyaltered, either
by improvingblood flow and/or by reduced demand.
From the Cardiolo~ Section, Universit_,,of Wisconsin Hospital and Clinics,
Madison, Wisconsin. This work was supported in part by PHS Grant HL-32350,
National Heart, Lung, and Blood Institute. National Institutes of Health, Bethesda,
Maryland; and by grants from the Rennebohm Foundation of Wisconsin, the Oscar
Mayer Cardiovascular Research Fund and American Heart Association Grants-inAid 91-GA-11/92-GS-26 of the Wisconsin Affiliate (the Dave McClain Research
Grant), Madison, Wisconsin and 92-729 of the National Center, Dallas, Texas.
Manuscript received November 28. 1094', revised manuscript received April
7, 1995, accepted April 20, 1995,
Address for correspondence: Dr. A. James Liedtke, Cardiolog~ Section.
H6/349, University. of Wisconsin Hospital and Clinics, 600 Highland Avenue.
Madison, Wisconsin 53792-3248.
@1995 by the Americm ('~llcgc ~fl ( aTdi,fl,~,,
0735-1097/95/$9.50
0735-1097(95)00223-Q
816
LIEDTKE ET AL.
CORONARY STENOSIS IN PIG HEARTS
animal models of compromised coronary reserve sufficient to
impair contractile performance yet preserve myocardial viability. These models are necessary' to develop causative associations among myocardial mechanics, metabolic function and
coronary flow to understand the clinical data better. We
previously developed a 7-day model of chronic coronary stenosis in intact swine that reduced coronaU flow velocity by
~50% and effected a 64% decline in regional shortening by
I week (15). Histologic examination revealed preserved viability. The purpose of the present report was to use a modified
4-day version of this model and to characterize and correlate
several estimates of myocardial metabolism with regional
shortening and coronary, perfusion. These measurements were
acquired on the fourth day of imposed coronary stenosis using
established metabolic techniques while coronau circulation
was maintained by extracorporeal perfusion (16).
Methods
First operation. Eight pigs weighing a mean (_+SE) 45.1 _+
1.7 kg were anesthetized with acepromazine maleate (0.11 to
0.22 mg/kg body weight intramuscularly), atropine sulfatc
(0.05 mg/kg intramuscularly) and ketamine hydrochloride
(20 mg/kg intramuscularly) followed by intubation and administration of a mixture of 0.8% to 2.0% isoflurane and nitrous
oxide/oxygen (50:50). In addition, 2% lidocaine hydrochloride
(3 ml intravenously) and pancuronium bromide (3 ml intravenously) were given initially, with additional dosages given
throughout the study if needed. Before operation, cefazolin
sodium (1 g intravenously) was also administered. A left
thoracotomy was performed as previously described (15).
Continuous monitoring of select leads of the electrocardiogram was performed to observe heart rate. After the pericardium was incised, a fluid-filled catheter was placed in an
internal mammary artery and retrogradely positioned in the
descending thoracic aorta for recording pressures. A second
catheter was inserted into the left atrium. This catheter had
both an access port for infusing adenosine (0.14 to 0.28 mg/kg
per rain) when needed to prevent possible coronary spasm
after surgical manipulation of the left anterior descending
coronary artery' and another port for infusing microspheres
(either tin-ll3, scandium-46, cerium-141 or ruthenium-103).
The mammary artery cannula was also used for sampling blood
containing microspheres (at 9.8c~ ml/min for 2 rain) during
coronary blood flow measurements. Microspheres were injected before and after imposing the partial coronary stenosis
around the left anterior descending coronary, artery'. Regional
mechanical performance was obtained using ultrasound crystals placed in the midmyocardium of the perfusion bed supplied by the left anterior descending coronary artery. Flow
veloci~ in this artery was measured from a Doppler velocity
probe (2.5 to 4.0 mm) placed at a site in the proximal third of
its distribution. Just distal to the Doppler probe we also placed
a hydraulic occluder cuff that was partially inflated to produce
an external coronary stenosis such that peak phasic flow
velocity was reduced by 509;. The hydraulic occluder cuff was
JACC Vol. 26, No. 3
September 1995:815-25
maintained partially inflated over the 4-day interval between
first and second operation to simulate a chronic stenosis.
During this interval, no attempt was made to remanipulate the
cuff inflation. Competency of cuff inflation was reassessed at
the time of second operation. In addition, an estimate of
coronary, reserve measured as peak reactive hyperemia after a
15-s occlusion was obtained before and after induction of
partial stenosis at the time of the first operation and before
corona U cannulation at second operation.
After operation and instrumentation, wires from the velocity probe and ultrasound crystals, together with an aortic
pressure line, were directed through a subcutaneous tunnel to
an exit site in the posterior neck region. An internal mammary
vein was cannulated, and its cannula was also externalized
through the neck and kept open with heparin to serve as a port
for injecting medications, if needed. During closure of the
chest, intrathoracic air was evacuated by multiple aspirations,
and cefazolin sodium (1 g) was given at the site of the thoracic
incision to prevent infection. After operation, buprenorphine
(0.3 mg intramuscularly), flunixin meglumine (0.5 ml intramuscularly) and Combiotic (penicillin and dihydrostreptomycin,
3 ml intramuscularly) were administered. The pigs were
brought to the recovery area and monitored daily and given
food containing flunixin meglumine (50 rag) and aspirin
(650 rag) and water. All procedures performed in this study
were approved by the University of Wisconsin Clinical Health
Science Animal Care and Use Committee, which adheres to
the National Institutes of Health guide for the care and use of
laboratory animals.
Second operation. Studies were conducted 4 days after the
first operation. Pigs now weighing 47.3 + 1.5 kg were again
sedated with ketamine (20 mg/kg intramuscularly) and given
atropine sulfate (0.05 mg/kg intramuscularly). The pigs were
reintubated with controlled positive ventilation using oxygensupplemented room air and anesthetized with alpha-chloralose
(l g intravenously initially, followed by 0.5 g intravenously
every hour thereafter), morphine (45 mg intravenously every
hour) and pentothal (10 ml intravenously, initially). A left
thoracotomy was performed in all animals. The detailed description of the extracorporeally perfused procedure, preparation and instrumentation has been reported elsewhere (16,17).
In the present study, the perfusion system was modified such
that only the left anterior descending coronary artery was
cannulated. This artery was perfused by an arterioarterial
shunt connected extracorporeally. Blood was withdrawn from a
cannulated femoral artery and returned by a low flow perfusion
pump. The extracorporeal circuit included a mixing chamber
for introducing and mixing radioactive substrates and indocyanine green. The dye was used for determining a dilution factor
(k) as an estimate of venous cross-contamination of blood
draining from adjacent myocardial beds into the anterior
distribution of the great cardiac vein.
Left ventricular and aortic pressures were measured using a
high fidelity double-tipped pressure device (Millar) placed in
the left ventricular chamber. Systemic pressures were maintained at -100 mm Hg and replenished with 6% dextran in
JACC Vol. 26, No. 3
September 1995:815 25
saline solution if needed. Electrocardiographic monitoring was
again performed throughout the operation and perfusion
trials. Heparin (20,000 U) was given initially, followed by
10,000 U every hour thereafter. Blood sugar levels were held at
-100 mg/dl, and additional dextrose was given if needed.
Regional systolic shortening in anterior myocardium was acquired with the implanted ultrasound crystals. Additional
microsphere measures were obtained before and 10 rain after
cannulation of the left anterior descending coronary artery.
Pump flows for the extracorporeal coronary circuit were set
according to the oxygen saturation of venous effluent sampled
from the anterior distribution of the great cardiac vein. The left
anterior descending coronary artery was then cannulated, and
the pump flows of the extracorporeal perfusion circuit were
adjusted to match the venous oxygen saturation. For technical
reasons, the Doppler velocity probe was removed to provide
adequate surgical space for the arterial cannulation.
After extracorporeal perfusion, steady-state infusion of
labeled [U-HC]palmitate (43/~Ci, 1.58 × 106 disintegrations
per minute (dpm)/min) and [5-3H]glucose (75 ~Ci, 2.74 x 106
dpm/min) into the extracorporeal circuit was started and
continued throughout the study. Samples for metabolic and
mechanical measurements were collected every 10 min over a
60-rain perfusion trial. Indocyanine green indicator was administered for 5 min every 20 min starting at time 0. The dilution
factor (k) was used in the calculation of carbon dioxide
production from labeled palmitate and glucose utilization from
tritiated glucose, as reported for glucose in earlier studies (17).
Serum fatty acid levels (p,mol.ml ~) were determined according to the method of Ho (18), and blood glucose levels
(/.~mol.ml-~) were obtained using a Glucometer lI. Myocardial
oxygen consumption (/~mol.h ~.g dry wt -~) was calculated
from hemoglobin oxygen saturation data according to a previously reported formula (16).
At the end of the study, fresh tissue samples were taken
from anterior and lateral myocardium perfused by the left
anterior descending and circumflex coronary, arteries, respectively, for isolating mitochondria. Other tissue samples from
the two beds were quickly freeze-clamped in liquid nitrogen
and stored at -70°C for later analysis. Hearts were then
dissected free and weighed. The weight of the anterior myocardial bed was calculated as 33.8% of the total heart weight on
the basis of data obtained from 40 previously studied animals
(33.8 _+ 0.7%). Hearts were sliced and stained in a solution of
1.5% triphenyltetrazolium chloride and in 20 mmol/liter potassium phosphate buffer (pH 7.4) for 1 h at 38°C to identi~
any areas of infarction. Thereafter, epicardial and endocardial
tissue samples from both beds were collected, weighed and
counted for radioactivity, and coronary flow was determined
on the basis of calculations of infused microspheres.
Analysis of blood, plasma and tissue samples. Arterial and
venous blood samples, 1 ml of blood in triplicate, were used to
measure carbon dioxide production from labeled palmitate,
and the rest of the collected blood was centrifuged at 1,500 g
for 10 min to obtain plasma. Plasma samples from artery and
vein were analyzed for tritiated water released from labeled
LIEDTKE ET AL.
CORONARY STENOSIS IN PIG HEARTS
817
glucose according to the procedures of Rovetto et al. (19)
using a Dowex-1 borate column. The tritiated water was eluted
with water and counted for radioactivity, and the rate of
glucose utilization was calculated (17). Tritium leakage by
nonmetabolizable dissociation from glucose was -0.2%. Another portion of the plasma was used for the determination of
lactate extraction. The lactate concentration was measured
enzymatically (20) and calculated as previously described (17).
Lactate concentration was also determined from frozen tissue
extracted in 6% perchloric acid (20).
Adenine nucleotides and creatine phosphate. Frozen tissue
from both perfusion beds were extracted with 6% perchloric
acid, neutralized and then analyzed by high performance liquid
chromatography using a Waters ~Bondapak C~8 column. The
compounds were eluted with a gradient consisting of solvent A
(50 retool/liter potassium dehydrogen phosphate and 2 retool/
liter tetrabutyl ammonium phosphate, pH 5.8) and solvent B
(50 retool/liter potassium dihydrogen phosphate, pH 5.8 and
acetonitrile, 2:1). The adenine nucleotides were detected at
260 nm, and creatine phosphate was detected at 210 nm on a
multichannel ultraviolet detector.
Glucose transporter protein. Additional glycolytic information was also gathered for the insulin-responsive glucose
transporter protein, hexokinase and phosphofructokinase activities. Glucose transporter protein concentration was quantified as described by James et al. (21) in aliquots of frozen
tissue homogenized in buffer containing 20 mmol/liter HEPES
(N-2-hydroxyethypiperazine-N'-2-ethanesulfonic acid), 1 retool/
liter ethylenediaminetetraacetic acid (EDTA) and 250 mmol/liter
sucrose and diluted with Laemmli sample buffer. Triplicate
aliquots of this mixture containing 30 /~g of protein in each
sample were subjected to sodium dodecyl sulfate-polyacrylic gel
electrophoresis using a 10% resolving gel. Proteins were electrophoretically transferred to 0.45-p~m Immobilon-P membranes
(Millipore). Membranes were blocked overnight at 4°C with a
solution containing 50 mmol/liter Tris buffer, 200 retool/liter
sodium chloride, 0.025% Tween 20 and 0.02% sodium azide, (pH
7.5) in 5% Carnation nonfat dry milk. Immobilon sheets were
then incubated for 60 rain at 37°C in an identical solution
contained in 1% milk and a 250-fold dilution of R820 anti-glucose
transporter protein polyclonal antisera (East Acres Biologicals).
Membranes were subsequently rinsed twice at room temperature
with the 1% milk solution, followed by incubation at room
temperature for 60 rain in the 1% milk solution and 3 gCi
iodine-125 goat anti-rabbit IgG (ICN). After incubation, the
membranes were washed three times for 15 min in the 1% milk
solution, air-dried and exposed to Kodak XAR-5 film at -70°C.
The visualized bands were traced, excised and counted in a
gamma counter. The results were corrected for background,
which was determined from unlabeled areas. Values were expressed relative to an internal control (15 ~g of myocardial
protein from Yucatan minipigs), which was run in triplicate on
each gel. For this particular measurement, glucose transporter
protein in hearts with external stenoses was compared with that in
tissue from a recently reported (22) historical control group of
nondiabetic aerobic pig hearts.
818
LIEDTKE ET AI,.
CORONARY STENOS1S IN PIG I IEARTS
JACC Vol. 26, No. 3
September 1995:815-25
Table 1. ExperimentalVariables of Aerobic Performance in Acute and Chronic Sham Hearts
Perfusate FAs 0xmol.ml i)
Perfusate glucose (gmoi.ml k)
LAD pump flows (ml.min t.g dry wt t)
LVP (ram Hg)
HR (beats.rain L)
SS (% initial values)
M£o 2 (mmol.h ~.g dry' wt t)
FA oxidation (#mol.h ~.g dry wt ~)
Glucose utilization (gmol.h ~.g dr3., wt 1)
Acute Sham Hearts
(developed concurrently
with present study)*
(n
7)
Chronic Sham Hearts
(Liedtkc et al. [31])f
[n = 7)
Chronic Sham Hearts
(Liedtke et al. [32])~
(n - 7)
Mean Sham Values
Statistics{}
11,40 = 11.113
6.4 + 0.4
6.4 _+ (1.5
99 ÷ 3
~ + 9
84.1 ~ 6.4
1.27 + 0.12
27.0 _+ 2.6
36.4 = 7.0
1).43 ÷ 0.04
7.1 * 0.6
6.2 ± 0.4
96 ± 3
137 _+ 4
11)1).4 ÷ 25.5
1,24 _+ 0.05
34.0 ± 4.7
36.4 + 13,1
0.39 _+ 0.05
6.4 = 0.6
6.0 + 0.5
91 +_ 5
182 -+ 3]1
77.0 _+ 62
1.12 = 0,10
19.6 +_ 3,0
30.2 + 3.3
0.41 _+ 0.02
6.6 _+ 0.3
6.2 +_ 0.3
95 +_ 2
138 +_ 8
87.2 + 8.8
1.21 _+ 0.05
26.9 +_ 2.4
34.3 _+ 4.9
NS
NS
NS
NS
F = 0.001
NS
NS
F = 0.034
NS
*Anesthesia: alpha-chloralose, morphine and pentothal, identical to intervention hearts with chronic coronary stenoses in present study. ~Anestbesia, first
operation: 0.4e~'~ to (/.8% halothane and 5(1~:,) nitrous oxide-50% o~'gen mixture; anesthesia, second operation, same. Intraoperatively during the 4 days between
operations, pigs received flunixin, meglumine and aspirin, as approved by the University of Wisconsin-Madison Research Animal Resource Center, :~Anesthesia
for first and second operations and interoperative analgesia same as in other chronic sham group. §Analysis of variance with Tukey's honestly significant
difference test. ]Hearts were atrially paced. Data presented are mean value + SE obtained during extracorporeal perfusion runs. FA = fatty acid; HR = heart
rate; LAD
left anterior descending coronary artery: LVP
left ventricular peak pressure; M~'o z = myocardial oxygen consumption; SS = regional systolic
shortening.
Hexoldnase. Frozen tissue was homogenized, and the
hexokinase activity of the homogenized tissue was estimated
by following the rate of nicotinamide adenine dinucleotide
phosphate (NADPH) production measured over 20 min at
340 nm and 30°C according to the methods of Sheer et al.
(23).
Phosphofructokinase. The tissue was homogenized in
150 mmol/liter potassium chloride, 50 mmol/liter potassium
bicarbonate and 6 mmol/liter EDTA, as described by Shonk
and Boxer (24). The enzyme activity in the extract was
measured as the rate of oxidation of nicotinamide adenine
dinucleotide (NADH) determined at 340 nm and 26°C, as
reported by Kemp (25).
Mitochondriai respiration. Mitochondria were isolated
from flesh tissue from both the left anterior descending and
circumflex-perfused myocardium according to a modified
method by Murphy et al. (26). Briefly, tissues were homogenized in 20 mmol/liter Tris buffer (pH 7.5) containing
0.25 mol/liter sucrose using a Kinematica polytron PT 10/35
spun once at a fifth of its maximal speed for 20 s, then once
at a sixth of its maximal speed for another 2(1 s. The
homogenate was centrifuged at 400 g for 20 min, followed by
centrifugation of the isolated supernatant at 1,500 g for
15 rain. The mitochondrial pellet was "washed" twice and
finally suspended in the homogenate medium. Mitochondrial protein (0.5 mg) was measured according to the
methods of Bradford (27) and used for the determination of
state 3 and state 4 respiration as well as the adenosine
diphosphate (ADP)/oxygen ratio and the respiratory control
ratio using a Clark oxygen-sensitive electrode (26,28). All
procedures were carried out at 4°C. The respiration medium
consisted of 20 mmol/liter Tris buffer (pH 7.4), 100 mmol/
liter sucrose, 100 mmol/liter potassium chloride and 2
mmol/liter inorganic phosphate. Mitochondrial protein
(0.5 mg) was added to the respiration medium, followed by
the addition of 10 mmol/liter malate and pyruvate as
substrate; ADP (1,040 nmol) was added to initiate state 3
respiration. Oxygen consumption was calibrated with the
standard solubility data of oxygen (29). Respiratory rates
and the respiratory control ratio were obtained along the
linear portion of the standard protein curves.
Statistics. Intragroup statistical comparisons in hearts
with external stenoses (intervention hearts, present study)
were made using paired Student t tests. When multiple
comparisons of regional systolic shortening and microsphere
flow data were made against baseline (initial values at first
operation), Bonferroni adjustments were included. Statistical significance was defined for probability values -<5%.
Data from intervention hearts were also contrasted with 1)
historical data from acute mild to moderate ischemia experiments using the extracorporeally perfused intact heart
model (16,17,30); and 2) three groups of sham hearts (Table
1). These sham hearts included two historical groups (n = 7
each) of chronic aerobically perfused hearts also studied
over 4 days (31,32) (chronic sham hearts) and one group
(n = 7) of acute sham hearts developed concurrently with the
intervention hearts of the present study. The three sham
groups were compared (Table 1) using analyses of variance
with Tukey's honestly significant difference test. The acute
sham group, weighing 42.8 ± 0.9 kg (mean ± SE), also
received the same preanesthetic medications and anesthesia
as hearts with external stenoses. Sham hearts included a
range of heart rates, as noted in Table 1, in part because of
the pacing used in one group of chronic sham hearts and a
somewhat wide variance in fatty acid oxidation. Measurements of glycolytic proteins, mitrochondrial respiration and
bioenergetics (Table 3) were compared in part between
intervention hearts and either acute sham or historical
control hearts using nonpaired Student t tests.
JACC Vol. 2t~. No. 3
September 19t~5:S15-25
LIEDTKE ET AL.
CORONARY STENOSIS IN PIG HEARTS
819
Table 2. Rest Coronary Flow Rates Measured by Microspheres in Intervention Hearts With Chronic
CoronaU Stenosis Imean ± SE)
Flow Rate (ml/min per 111{)wet wt)
tAD
First operation
Bcfi)rc partial cuff inflation
After partial cuff" inflation
p value
Second operation
Bct\~rc LAD cannulation
and cxtracorporcal pcrfusion
After LAD cannulation
and cxtracorporcal pcrfusion
p value
LCx
EPI
ENDO
EPI
ENDO
82 : 1~
6tJ - S
NS*
108 + 15
77 + O
NS*
69 - 10
6fl 7
NS*
11)8 _+ 16
87 + l0
NS*
S5 - 5
105 ~ 7
86 + 4
99 + 3
82 ~ 6
93 + 5
NS*t
N S*'l"
88 - 7
NS:~+
~)1 + 111
NS~+
-
*lntragroup comparisons at first and scctmd operations by, pairvd Student t test, including Bonferruni correction.
tlntragroup comparisons between first and scctmd opcralitms (after partial cuff inflation vs. before left anterior descending
corona U arte W [LAD] cannulation and cxtracorporcal pcrfusion) by' paired Student t test, including Bonferroni correctkm.
END() (EPI) cndocardial (~'picardial) flow distribulion: l.Cx :: left circumflex corona O' artery' peffusion system.
Results
Precannulation data from first and second operations.
Consequent to partial cuff inflation in intervention hearts, peak
phasic velocity was reduced by a mcan (-SE) of 49 + 5~J; of
prestenotic values at first operation. As a result, whereas rest
flow in stenosed vessels was only slightly reduced in the
endocardial perfusion zone (Table 2) (p - NS), peak reactive
hyperemia (ratio of peak hyperemic to baseline ttow velocity)
after a 15-s arterial occlusion was diminished by 38% (2.1 _+0.2
to 1.3 + 0.1, p < 0.004).
At second operation, peak phasic velocity with the cuff
occluder still inflated was 79 _+ 10~¢~of prestcnotic values
(62 + 11% of prestenotic values if the responses of one pig
were deleted), and reactive hypcrcmia had partially recovered (1.9 _+ {I.2). Rest flows in stcnosed vessels before
cannulation were comparable to post-cuff inflation flows
(Table 2) at first operation. Flows in the uncannulated
circumflex bed were also comparable to those of first
operation (Table 2). Before coronary cannulation, venous
oxygen saturation in anterior venous cfflux was 21.4 + 3.2C,~.
As described in Methods section, cxtracorporeal pump flows
were set to match these venous oxygen values after cannulation and resulted in flows of 4.7 = 0.3 ml.min i.g dry wt
This matching was effective, as reflected by the microsphere
data, which showed no regional pcrfusion differences before
and after cannulation.
Measurements during perfusion trials at second operation.
Myocardial pressure development during cxtracorporeal coronary perfusion included peak left ventricular pressures of 95 ~+
4 mm Hg and end-diastolic pressures of 9 + 1 mm Hg in
intervention hearts. Heart rate was 12~, +_ 8 beats/min. Perfusate levels of free fatty acids and glucose were (/.33 +_ 0.()4 and
6.0 + 0.3 /,,mol.ml ~. respectively. These mechanical and
biochemical data were comparable to those for the three sets
of sham hearts presented in Table 1.
Regional systolic shortening in intervention hearts is
shown over the 4-day study interval in Figure 1, and a more
detailed description of shortening during the extracorporeal
perfusion trial at second operation is illustrated in Figure 2.
Partial cuff inflation at first operation caused no abrupt
changes (100CJ~ to 97 + 4% of initial values) but by the
fourth day had effected an appreciable deterioration in
performance (62 _+ 7% of initial values, p < 0.003).
Extracorporcal perfusion itself effected an additional 16%
decline in regional shortening after cannulation (p < 0.003),
for a total decrease of 54% (46 _+ 7% of initial values). This
compared with mean sham values of 87.2 _+ 8.8% (Table 1,
Fig. 2) also acquired during extracorporeal perfusion.
Metabolic status was estimated from rates of oxygen consumption and substrate utilization, mitochondrial performance
and bioenergetics. The decline in regional systolic shortening
in intervention hearts was not matched by oxygen consumption
(1.01 _+ 0.09 mmol.h-l.g dry wt ~) (Fig. 3, panel A), which
only decreased by 17% compared with composite sham heart
values (Table 1; Fig. 3) and was greater than values previously
published for mild to moderate acute ischemia using the same
perfusion system (16). The capacity for retained aerobic performance was reflected in the estimates of mitochondrial
respiration, which were no different than acute aerobic values
(Table 3). Fatty acid oxidation, estimated by carbon dioxide
production from U-carbon-14 palmitate in pig hearts, is noted
to vau widely at aerobic conditions (Table 1, Fig. 4, panel B)
and also during mild to moderate acute ischemia (-18 to
-27% change) based in part on fatty acid availability in
perfusate (16). In the present intervention hearts, fatty acid
oxidation (15.4 _+ 2.7/xmol.hr Jg dry, wt -l) (Fig. 4, panel A)
was appreciably decreased both below aerobic values (-37%
820
LIEDTKE ET AL.
CORONARY STENOS1S IN PIG HEARTS
JACC Vol. 26, No. 3
September 1995:815-25
Table 3. Measurements of Glycolytic Proteins, Mitochondrial Respiration and Bioenergetics
Acute Sham or Historical
Control Hearts (LAD)*~"
GLUT 4 (¢~ of control)
Mean + SE
p value
Hexokinase (U/g ,*ct wt)
Mean ± SE
p value
PFK (U/g wet wt)
Mean ~ SE
p value
Respiration cnmrol ratio
Mean ± SE
p value
State 3 respiratinn
Mean -+ SE
p wdue
State 4 respiration
Mean + SE
p v~due
ADP/()
Mean ~ SE
p value
Creatine phosphate (#.mol/g dry wt)
Mean + SE
p value
Adenosine triphosphate (rtmolg dry,'wt)
Mean ± SE
p value
Adenosine diphosphate (>mol/g dry' wt)
Mean - SE
p value
Adenosine monophosphate (/,moL'g dry wt)
Mean ± SE
p value
Tissue lactate (#mol/g dr5., wt)
Mean + SE
p ~alue
Intervention Hearts:I
LAD
991) + 5.6
< 11.11'44
77.3 _'_ 7.5
0.39 + (I.02
NS
(/.39 + 0.01
12.3 + (I.6
<0.012
10.2 -+ 0.4
4.9 - 1.2
NS
3.2 + 0.2
240 + 42
NS
222 +- 20
61i ± 15
NS
70 + 3
3.3 ± {).3
NS
3.0 + 0.1
35-3
NS
23*-6
25+ 1
0.001
19 + 1
LOx
81.5 = 9.9
NS
0,45 +_ 0.02
<0.017
11.1 _+ 0.5
NS
3.7 -+ 0.4
NS
283 -- 23
0.038
77 -+ 3
NS
3.1 +- 0.1
NS
14-+3
NS
23+-I
<0.019
5.5 + 0.2
NS
5.2 +- 0.4
0.4 - 0.1
NS
0.4 + 0.1
6.3 -+ 0.4
<0.013
0.4 -+ 0.1
NS
35.1 -- 7.4
39.9 _+ 7.9
NS
* Data ti'om Stanley ct aL (22). fp values are intergroup comparisons of left anterior descending coronary, artery. (LAD)
data between acute sham or historical control hearts versus intervention hearts. ~p values are intragroup comparisons, left
anterior descending versus left circumflex coronary, artery (LCx) pcrfused myocardium. ADP/O
measure of oxidative
phosphurylation: GLUT 4 glucose transporter protcin for cardiac muscle; PFK = phosphofructokinase.
120
A
tll
a
100
Figure 1. Regional systolic shortening (SS) expressed as
percent of initial values over time for intervention hearts.
Ultrasound crystals were placed at midmyocardial depth in
left anterior descending coronary artery (LAD) perfused
myocardium. Regional function showed a progressive deterioration over 4 days of exposure to partial coronary stenosis.
Extracorporeal perfusion itself effected an additional 16%
decline in motion during the perfusion trial. BC (AC) =
before (after) cannulation; BI (AI) = before (after) cuff
inflation. Data shown are mean value (columns) _+ SE
(vertical bars).
80
GO
40
20
0
BI LAD
AI LAD
FIRST SURGERY
BC LAD
SECOND
A C LAD
SURGERY
J A C C V o l . 26, N o . 3
September 1995:815-25
CORONARY
140
e
Figure 2. Regional mechanical performance for
anterior myocardium during extracorporeal perfusion trials in intervention hearts (A) and three
sham heart groups (B). Initial value refers to
performance at the beginning of first operation for
both intervention and chronic sham hearts or precannulation values in the case of acute sham hearts.
Systolic shortening was decreased by 54% in intervention hearts. Extracorporeal peffusion itself also
effeeted a net decline (-8.3%) in motion (i.e.,
-16% in acute sham hearts, +0.4% in chronic
sham 1 hearts [31] and -9.4% in chronic sham 2
hearts [32]).
STENOSIS
A
Clwo,V¢ Coronaq St,n~ds
140
= 120
It,
-= 1t0
I
)
100
; leo
-~
" "
o
©
-
00
r
l
I
0....o--4O
[
7°
v
J
L
.
'
T
I
---o~
T
.
m
"F'"~'"~
B
80
1![ J lr
I
V
t
'
'
' -~...fl,_
1JO
tie
0
Z
I
I
I
I
I
I
I
(i
10
|0
34
¢0
50
60
Figure 3. Regional myocardial oxygen consump-
tion from anterior myocardium for intervention (A)
and sham hearts (B). Intervention hearts appeared
to retain aerobic behavior over the course of the
perfusion trials.
O
$
~
I
Chronic Sham 1
, Chronic Sham 2
20
P
"10
O
1;0
40
50
|0
Discussion
Experimental
considerations.
hibernation:
metabolic
and c o r o n a r y flow
The present report describes an intact pig
heart model with long-term coronary stenosis sufficient to
compromise peak phasic flow velocity and in part reactive
hyperemia but not long-term rest coronary flows. These ad-
A
1.80
B
Cl¢oei¢ Coroury $tenodt
1.60
"
1,20
1,20
!
l
T
o---.o----~,
i
i
J
r
T
1
V
A
1
1
"~
0.80
'0
0
¢
.
J
0.40
¢
S
£
£
O.lO
-10
l0
Estimates of bioenergetics were obtained by biopsy at the
conclusion of the perfusion trials in intervention hearts and are
presented in Table 3. In absolute terms, adenosine triphosphate (ATP) was decreased compared with that in acute sham
hearts or adjacent aerobic myocardium, and creatine phosphate values appeared reduced compared with historical control values (33). This may reflect inadequate energy production
in left anterior descending coronary perfused tissue or increased energy demand in presumably hyperkinetic adjacent
circumflex coronary perfused tissue.
Tissue processed with triphenyltetrazolium staining showed
no evidence of myocardial infarction. This agreed with previous data (15,32) in which tissue was histologically evaluated
and was without microscopic evidence of necrosis.
t
0.00
10
PEIFUSlON ;'IllS (mini
1.40
1.10
;
+ Acute S~mm
4O
@
i
:~
r
,...-.,---I--'-F"T--r--I
1
1
mIFUSlO, TIE (mill)
~"
|
E
change) in pigs with similar serum fatty acid levels (16) and
below composite values for sham hearts (-43% change).
Conversely, in intervention hearts, exogenous glucose utilization, estimated from release of tritiated water from 5-hydrogen-3
glucose, was many times higher (Fig. 5, panel A) than aerobic
values reported historically (17) or in sham hearts (Table 1; Fig.
4, panel B) but was less than the flux rates achieved in acute mild
to moderate ischemia (30). These shifts in glucose utilization
agree with trends reported clinically (4-12). Increases in glucose
flux were not explained by increased activity of selective glycolytic
enzymes or glucose transporter protein. Compared with data in
adjacent, aerobically peffused myocardium of intervention hearts
or in the same left anterior descending coronary perfusion bed of
acute sham hearts (Table 3) or in historical controls (22), there
was either no difference or a decrease in enzyme activities or
glucose transport protein function in intervention hearts (Table
3). Mean lactate extraction data for the perfusion trial were 16 _+
19 p~mot.h 1.g dry wt-I, which probably reflected lactate extraction and some lactate release through the multifold increase in
glycolysis. Tissue lactate concentrations in intervention hearts
were comparable in both anterior descending and circumflex
peffused myocardium.
i
60
4
N
=
I
T
20
0
-10
821
LlEDTKE ET AL.
1N P I G H E A R T S
,
m
' ""--.-.~._L..--,'--~
1,00
0.80
O.6O
* Acute Shim
0.40
A ¢hri: Slum 1
e Chronic Sham 2
0,21
m
I
I
n
I
I
I
O
10
20
30
40
60
40
PERFUSION TiE {rain)
0.00
-10
10
20
m
m
m
|
30
40
80
60
I~FUSm T E (m)
822
I , I E I ) T K E Vf[
('ORONARY
STENOSIS
IN IJl(; l l L / \ R I S
A
SO
i
B
5O
Chronic Coronary Stenom
'~
J A C C V o l . 26, N o . 3
S e p t e m b e r 19 9 5 : 8 1 5 25
1 ,'%k.
A
+ Acute Sham
i
• Chrmc Share 1
4o
'°""F:4 i::'!
s0
O
tG.~
.,'i
.+
t
~
L
l
l
1
/ /• ¢" " ~J- - !
1
, l/!
I
I
]A
IlFI 124
i0
T
1
"+
T
l
~ - .0,.. _ _ .G._.
i
"
Figure 4. Rates of myocardial fatty acid oxidation
estimated by carbon dioxide production for anterior
myocardium in intervention (A) and sham (B) hearts
during extracorporeal perfusion. Data for 0- and
10-min perfusion were not included in the average
values reported in the text because of disequilibrium
of exogenous labeling in myocardium. Fatty acid
oxidation in intervention hearts was reduced by 43%
below mean values in sham hearts, but these latter
groups evinced wide variation, presumably due to
variation in heart rates (HR [beats/minD.
I!
20
'
_. O
I
i
E
-i
HI 182
r'-i
E
-1
I
-10
0
I0
10
iO
40
50
0
-10
60
0
10
TW(R)
Pi~m~
I0
iO0
A
~oo
^
1110 Chromic Coronary Stenosis
t
,,,
160
140
>!-q
_
[
^
Ct 100
$
B
+ Acute Slim
,+ Chrwc Sham 1
, Chronic Sham 2
80
$u
I: 40
60,
L
E 40
10
0
-10
levels in myocardium pcrfused by the left anterior descending
coronary artery. In the present report, there was no evidence
by tissue staining of macroinfarction. This finding corresponded with other studies (15,32) using this preparation in
either a 4- or 7-day protocol, in which no histologic evidence of
myocardial necrosis was observed. Microscopically, a few
minor loci of abnormal cells were observed with loss of nuclei
and cross striations. Thus, the pig model presented here bears
similarity to the mechanical or metabolic accommodations
previously reported (34,35) clinically in patients with coronary
artery disease and reversibly depressed myocardial function.
Hibernating myocardium was initially regarded as a consequence of low flow ischemia (3), but this concept is now being
questioned because in clinical studies it is observed (36) that a
majority of reversibly dysfunctional myocardium is perfused at
normal rest blood flows. Indeed, the flow perturbation responsible for affecting down-regulation of mechanical function in
hibernating hearts is still under active review, with proponents
advocating either sustained hypoperfusion or intermittent ischemia with cumulative stunning (14). Sustained hypoperfusion
as a mechanistic determinant may not be compatible with
140
p 100
40
p
$0
160
120
$
m
IO
180
'0 1t0
I10
I
40
3
),
I
I
30
PERFUSION Tile Imin)
justments in flow velocity resulted in inipaired contractilc
performance and altered metabolism. Aerobic behavior was
maintained at the end of 4 days undcr such conditions, but
fatty acid oxidation was depressed and glycolysis was increased
multifold. It is inferred from the lactate extraction/production
data in corona U venous effluent that glucose oxidation was
preserved or enhanced in intervention hearts. This preservation is argued because, in the setting of increased glycolysis,
any mitochondrial impairment in thc oxidation of glucose
would have led to a pronounced release of lactate. This
preservation is also supported by the absence of accumulation
of lactate in tissue perfused by the left anterior descending
coronary perfusion circuit. As noted from the protein dala
(Table 3), the increase in glycolysis occurred at normal t)r
slightly decreased levels of glucose protein transporter and
enzyme activities regulating glucose uptake. The relation between fatty acid oxidation and exogenous glucose utilization
was reciprocal and may reflect the traditional allosteric and
product inhibitions that govern competitive substrate utilizations. The multifold increase in exogenous glucose utilization
was not completely sullicicnt to maintain ATP levels at aerobic
II
v
I
I
),
l
"
i
HR 137
l
t
1
SO
I~0
•
I0
I
i
i
i
i
m
l
0
II
tO
30
40
SO
$0
~SION
T W (Bin)
~
i
|
-10
0
10
a
l0
RERF~
i0
I
40
Title(mm)
Figure 5. Myocardial exogenous glucose utilization measured during perfusion trial for intervention (A) and sham hearts (B). There was a
multifold increase in exogenous glucose utilization in intervention hearts compared with that in
aerobic sham hearts.
JACC V'ol. 2~. No. 3
September 1905:815 25
continued tissue viability because the limited oxygen storagc
capacity of obligately aerobic myocardium places such hearts
at continued risk for acute ischemia or infarction. An alternate
hypothesis is intermittent ischemia with periodic aerobic relief
from chronic anaerobiosis but with collective stunning. Folts et
al. (37) showed, in a corona D, stenosis model in dogs, a pattern
of cyclic flow variation with formation and washout of platelet
microthrombi in response to a critical narrowing of a corona U
artery. This same phenomenon has been argued to occur
clinically (38). Such a mechanism could explain several facets
of hibernating myocardium in that the intermittent ischemia
and reperfusion may contain certain cardioprotective properties of preconditioning, allow' some preservation of aerobic
bioenergetics with higher ATP production from fatty acid
oxidation and simplify the interpretation of mechanical downregulation as the cumulative effect of coronary reperfusion
with myocardial stunning. Uncoupling of the flow-functional
relatkm was in fact observed early in the development of
corona D' occlusion by amaroid constriction in canine experiments reported by Canty and Klockc (39), suggesting myocardial stunning as an early, and perhaps requisite, prodromc to
hibernation. Shen et al. (14) recently suggested that the motkm
abnormalities previously ascribed to myocardial hibernation
might be better explained bv viewing them as a result of
"chronic myocardial stunning" and argued for abandoning the
term hibernation. The present data observed in intervention
hearts with stenoses are in keeping with the concept of
intermittent (in our case, unwitnessed) bouts of ischcmia
followed by reperfusion because our microspherc data at
second operation were comparable to normal rest flows, and
metabolism was aerobic.
One may speculate that repetitive stunning is perhaps
responsible in part for dictating the observed changes in
substrate utilization reported in the present study. We have
extensively characterized (16,17,30,40) intermediary, metabolism in acutely stunned myocardium during postischemic
reperfusion in the cxtracorporeally perfused pig model. Rcsuits in these acute hearts showed 1) near-complete recover',' in
aerobic oxygen consumption despite a persistent impairment
in mechanical function; 2) a significant increase in glycolysis
and glucose oxidation; and 3) complete recovery and on
occasion an overshoot above preischemic values of fatty acid
oxidation. With the exception of the latter, these changes are
directionally compatible with the long-term trends reported
here. The discordant results in fatty acid metabolism between
acute and chronic hearts might bc furthcr explained by threshold effects triggering regulatory inhibitions between compcting
substrates. In acutely stunned hearts, exogenous glucose utilization increased on average to 48 +_ 1il/zmoFh I.g dry, wt
during reperfusion (17,30), whereas in the present study it was
three times higher and more likely to influence allosteric and
product inhibition. By protocol design, the duratkm of rcperfusion in our short-term studies was only 40 to 6(i rain.
However, Matsuzaki et al. (41) rcported in a model of shortterm hibernation (but with some infarctkm) that a 5-h exposure of partial corona U stcnosis caused regional mechanical
LIEDTKE ET AL.
CORONARY STENOSIS IN PIG HEARTS
823
dysfunction during reperfusion for at least 3 days. If the
duration of the effects of intermittent ischemia with reperfusion on metabolism is similar to that observed on mechanics in
the Matsuzaki model, and if the effects are cumulative, their
collective influence may well explain the magnitude of shifts in
substrate utilization reported here. It should be emphasized,
however, that the hypothesis of demand and intermittent
ischemia postulated here will be proved only with direct
observations, such as the telemonitoring of systolic shortening
and venous oxygen saturation in conscious animals during the
intervals between operations.
Experimental hibernation: methodologic considerations.
The present model was developed to describe the metabolic
effects of long-term partial coronary, stenosis. Because of the
relative deficit of preformed collateral vessels in pig hearts and
their inability to undergo complete angiogenesis secondary to
stress (42), our objective was to readjust coronary reserve only
modestly and thus avoid acute ischemia. This approach was
successful, as evinced by the preserved lactate consumption
profile, lack of increase in tissue lactate concentrations, negative triphenyltetrazolium staining in intervention hearts and
absence of necrosis by histologic review in previous studies
(31) of reperfusion and mechanical recovery with this model.
Several additional comments, technical points and possible
limitations are appropriate in the context of this new animal
preparation:
1. Anesthesia and analgesia regimens were reviewed and
approved by the University of Wisconsin-Madison Research
Animal Resources Center. The increase in body weight in
intervention animals between operations may be viewed as a
reflection of their clinical stability.
2. The protocol for intervention animals was shortened
from the original period of 7 days (15) to that of 4 days. This
was done to prevent any late-occurring infections (there were
none), lessen the labor-intensive animal handling and resultant
expenses of a complex, long-term animal preparation and
diminish the risk of pericarditis from the first operation, which
might independently compromise regional systolic shortening.
3. Extracorporeal perfusion had a detrimental effect on
mechanical performance both in intervention and sham hearts.
From precannulation values, regional systolic shortening in
intervention hearts further declined by 16% and in sham hearts
by 8.3%. This change may reflect some alteration of vascular
turgor as a result of the nonphasic perfusion characteristics
of the extracorporeal perfusion system, which in turn might
secondarily influence myocardial elastance and diastolic stiffheSS.
4. Dilution contamination of venous effluent in the anterior
distribution of the great cardiac vein by venous drainage in
adjacent beds was insignificant in the present study on the basis
of the k values estimated by indocyanine green indicator (see
Methods). Values were 0.95 _+ 0.01 in intervention hearts,
which indicated that the measurements of myocardial oxygen
consumption and net lactate extraction, which were derived
using nonradioactively labeled methods, were not appreciably
distorted by contaminated venous blood.
824
LIEDTKE ET AL.
CORONARY STENOSIS IN PIG HEARTS
5. Because of the partial recover, of reactive hyperemia in
intervention hearts, which may reflect capacitance changes in
the cuff occluder over time, we plan on developing a fixed, rigid
collar as the extraluminal stenosis device to effect greater
dysfunction of contractile behavior in future studies. Use of
this new device will allow us also to compare the presumed
intermittent flow perturbations reported here with a more
sustained intervention of hypoperfusion.
6. Heart rate increased selectively in intervention hearts by
22% before and after coronav cannulation and was 19%
higher than at first operation. One possible explanation of this
trend is altered tissue compliance and increased myocardial
stiffness secondary to exposure to chronic coronary stenosis.
This stiffness might conceivably be exacerbated by the perfusion dynamics of a constant-flow perfusion pump during
extracorporeal perfusion, which in turn would trigger sympathetic nerve stimulation and an increased heart rate. Sinus
tachycardia was also observed during recovery experiments in
reperfused hearts after relief of chronic corona~ stenosis (32).
However, the increase in heart rate was not excessive in the
present studies and frequently has been noted in past acute
ischemia studies using pentobarbital. We do not believe that
the metabolic data reported here reflect a condition of "demand ischemia" as a result of excessive tachycardia. The recent
data of Massie et al. (43) indicated that in pig hearts this type
of ischemia occurred only at suhendocardial/subepicardial flow
ratios <-0.87 _+ 0.04. Our lowest ratio in intervention hearts at
second operation was 1.13 _+ 0.15. Tissue lactate concentrations also argue against this hypothesis.
JACC Vol. 26, No. 3
September 1995:815-25
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
We thank Larry F. Whitesell. BS, Catherine R. Kidd, BS, Gregory R. Thomas.
BS, Daniel K. Paulson, MS, Emanual Scarbrough, MS, and Alice M. Eggleston.
MS, for technical assistance.
22.
23.
References
1. Helfant RH, Pine R, Meister SG, Fcldman MS, Trout RG, Banka VS.
Nitroglycerin to unmask reversible asynergy: correlation with post corona~
bypass ventriculography. Circulation 1974;50:108-13.
2. Cohn PF, Gorlin R, Herman MV, et al. Relation between contractile reserve
and prognosis in patients with coronary artery disease and a depressed
ejection fraction. Circulation 1975:51:414 20.
3. Rahimtoola SH. A perspective on the three large multicenter randomized
clinical trials of coronary bypass surgery for chronic stable angina. Circulation 1985:72: 8uppl V:V-123-25.
4. Brunken R, Tillisch JH, Schwaiger M. et al. Regional perfusion, glucose
metabolism, and wall motion in patients with chronic electrocardiographic Q
wave infarctions: evidence for persistence of viable tissue in some infarct
regions by positron emission tomography. Circulation 1986:73:951-63.
5. Hashimoto T, Kambara H, Fudo T, ct al. Non-Q wave versus Q wave
myocardial infarction: regional myocardial metabolism and blood flow
assessed by positron emission tomography. J Am Coil Cardiol 1988;12:8893.
6. Marshall RC, Tillisch JH, Phelps ME. et al. Identification and differentiation
of resting myocardial ischemia and infarction in man with positron computed
tomography, lSF-labeled fluorodeoxyglucose and N-13 ammonia. Circulation
1983;67:766-78.
7. Vanoverschelde J-LJ, Melin JA, Bol A, et al. Regional oxidative metabolism in
patients after recovery from reperfused anterior myocardial infarction: relations
to regional blood flow and glucose uptake. Circulation 1992;85:9-12.
8. Schwaiger M, grunken R, Grover-McKay M, et ah Regional myocardial
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
metabolism in patients with acute myocardial infarction assessed by positron
emission tomography. J Am Coil Cardiol 1986;8:800-8.
Gropler RJ, Geltman EM, Sampathkumaran K, et al. Functional recove~
after coronary revascularization from chronic coronary, artery disease is
dependent on maintenance of oxidative metabolism. J Am Coll Cardiol
1992;20:569-77.
Eitzman D, AI-Aouar Z, Kanter HL, et al. Clinical outcome of patients with
advanced coronary, artery disease after viability studies with positron emission tomography. J Am Coll Cardiol 1992;20:559-65.
Ma~ick TH, Maclntyre WJ, Lafont A, Nemec J J, 8alcedo EE. Metabolic
responses of hibernating and infarcted myocardium to revascularization: a
follow-up study of regional perfusion, function and metabolism. Circulation
1992:85:1347-53.
Tillisch J, Brunken R, Marshall R, et al. Reversibility of cardiac wall-motion
abnormalities predicted by positron tomography. N Engl J Med 1986;314:
884-8.
Bolli R. Myocardial "stunning" in man. Circulation 1992;86:1671-91.
Shen Y-T, Hasebe N, Zhang H, Vatner SF. Impaired regional myocardial
function during amaroid-induced chronic coronary" artery stenosis in conscious pigs: hibernation or stunning? [abstract]. Circulation 1993;88 Suppl
1:I-188.
Bolukoglu H, Liedtke AJ, Nellis SH, Eggleston AM, Subramanian R,
Renstrom B. An animal model of chronic coronary stenosis resulting in
hibernating myocardium. Am J Physiol 1992;263:H20-9.
Liedtke AJ, Nellis SH, Neely JR. Effects of excess free fatty acids on
mechanical and metabolic function in normal and ischemic myocardium in
swine. Circ Res 1978;43:652-61.
Liedtke AJ, Renstrom B, Nellis SH. Correlation between [5-3H]glucose and
[U-L~C] deoxyglucose as markers of glycolysis in reperfused myocardium.
Circ Res 1992;7l:689-700.
Ho RJ. Radiochemical assay of long chain fatty acids using 63Ni as tracers.
Anal Biochem 1970;36:104-13.
Rovetto MJ, Lamberton WF, Neely JR. Mechanisms of glycolytic inhibition
in ischemic rat hearts. Circ Res 1975;37:742-51.
Fleischer WR. Enzymatic methods for lactate and pyruvic acid. In: MacDonald RP, editor Standard Methods in Clinical Chemistry, Vol. 6. New
York: Academic Press, 1970:245-59.
James DE, Strube M, Mueckler M. Molecular cloning and characterization
of an insulin-regulatable glucose transporter. Nature 1989;338:883-7.
Stanley WC, Hall JL, Smith KR, Cartee GD, Hacker TA, Wisneski JA.
Myocardial glucose transporters and glycolytic metabolism during ischemia
in hyperglycemic diabetic swine. Metabolism 1994;43:61-9.
Sheer WD, Lehmann HP, Beeler MF. An improved assay for hexokinase
activity in human tissue homogenates. Anal Biochem 1978;91:451-63.
Shonk CE, Boxer GE. En~'me patterns in human tissue I. Methods for
determinations of glycolytic enzymes. Cancer Res 1964;24:709-21.
Kemp RG. Phosphofructokinase from rabbit skeletal muscle. Methods
En~mol 1975;42C:71-7.
Murphy ME, Peng CF, Kane J J, Straub KD. Ventricular performance and
biochemical alteration of regional ischemic myocardium after reperfusion in
the pig. Am J Cardiol 1982;50:821-8.
Bradford MM. A rapid and sensitive method for the quantitation of protein
utilizing the principle of protein-dye binding. Anal Biochem 1976;72:248-54.
Higihara B. Techniques for the application of polarography to mitochondrial
respiratkm. Biochem Biophys Acta 1961;46:134-42.
Estabrook RW. Mitochondrial respiratory control and the polygraphic
measurements of ADP:O ratios. Methods Enzymol 1967;10:41-7.
Liedtke AJ, Renstrom B, Hacker TA, Nellis SH, The effects of moderate
repetitive ischemia on myocardial substrate utilization. Am J Physiol. In
press.
Liedtke AJ, Renstrom B, Nellis SH, Subramanian R, Woldegiorgia G.
Myocardial metabolism in chronic reperfusion following nontransmural
infarction in pig hearts. Am J Physiol 265:1993;H1614-22.
Liedtke A/, Renstrom B, Nellis SH, Subramanian R. Myocardial function
and metabolism in pig hearts following relief from chronic partial coronary
stenosis. Am J Physiol 1994;267:H1312-9.
Liedtke AJ, Nellis SH, Neely JR. Effects of excess free fatty acids on
mechanical and metabolic function in normal and ischemic myocardium in
swine. Circ Res 1978;43:652-61.
Vanoverschelde J-IA, Melin JA, Bol A, et al. Regional oxidative metabolism
in patients after recovery from reperfused anterior myocardial infarction:
JACC Vol. 26, No. 3
September 1995:815 25
35.
36.
37.
38.
relations to regional blood flov, and glucose uptake. Circulation 1992:85:9 12.
Vanoverschelde J-LJ, Wijns W, Depre C, et al. Mechanisms of chronic
regional postischemic dysfunction in humans: new insights from the study of
uoninfarcted collateral-dependent myocardium. Circulation 1993;87:1513-3.
Udclson, JE. Can technetium 99m-labeled sestamibi track myocardial viability? J Nucl Cardiol 1994;h571-5.
Folts JD, Gallagher KP, Rowe GG. Blood flow reductions in stenosed canine
coronary arteries: vasospasm or platelet aggregation? Circulation 1982;65:
248-55.
Willerson JT. Campbell WB, Winniford MD. et al. (1995) Conversion from
chronic to acute coronary artery"disease: speculation regarding mechanisms.
Am J Cardiol 1984;54:1349-54.
LIEDTKE ET AL.
CORONARY STENOSIS IN PIG HEARTS
825
39. Canty JM, Klocke FJ. Reductions in regional myocardial function at rest in
conscious dogs with chronically reduced regional coronary artery pressure.
Circ Res 1987;61: Suppl II:II-107-16.
40. Renstrom, B, Nellis SH, Liedtke AJ. Metabolic oxidation of glucose during
early myocardial reperfusion. Circ Res 1989;65:1094-101.
41. Matsuzaki M, Gallagher KP, Kemper WJ, White F, Ross J. Sustained
regional dysfunction produced by prolonged coronary stenosis: gradual
recovery, after reperfusion. Circulation 1983;68:170-82
42. White FC, Carroll SM, Magnet A, Bloor CM. Coronary collateral development in swine after coronary artery occlusion. Circ Res 1992;71:1490-500.
43. Massie BM, Schwartz GG, Garcia J, Wisneski JA, Weiner MW, Owens T.
Myocardial metabolism during increased work states in the porcine left
ventricle in vivo. Circ Res 1994;74:64-73.