Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Asperger syndrome wikipedia , lookup
Alcohol withdrawal syndrome wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Recovery International wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Parkinson's disease wikipedia , lookup
History of psychiatry wikipedia , lookup
Abnormal psychology wikipedia , lookup
Mental health professional wikipedia , lookup
Conversion disorder wikipedia , lookup
Posttraumatic stress disorder wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
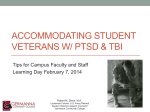
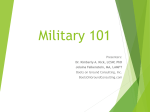
Rehabilitation Psychology 2009, Vol. 54, No. 3, 239 –246 In the public domain DOI: 10.1037/a0016908 Assessment and Diagnosis of Mild Traumatic Brain Injury, Posttraumatic Stress Disorder, and Other Polytrauma Conditions: Burden of Adversity Hypothesis Lisa A. Brenner Rodney D. Vanderploeg VA VISN 19 Mental Illness Research, Education, and Clinical Center (MIRECC); University of Colorado Denver, School of Medicine James A. Haley VA Medical Center; University of South Florida; Defense and Veterans Brain Injury Center Heidi Terrio Evans Army Community Hospital; Defense and Veterans Brain Injury Center Objective/Method: Military personnel returning from Iraq and Afghanistan have been exposed to physical and emotional trauma. Challenges related to assessment and intervention for those with posttraumatic stress disorder (PTSD) and/or history of mild traumatic brain injury (TBI) with sequelae are discussed, with an emphasis on complicating factors if conditions are co-occurring. Existing literature regarding cumulative disadvantage is offered as a means of increasing understanding regarding the complex symptom patterns reported by those with a history of mild TBI with enduring symptoms and PTSD. Implications: The importance of early screening for both conditions is highlighted. In addition, the authors suggest that current best practices include treating symptoms regardless of etiology to decrease military personnel and veteran burden of adversity. Keywords: Operation Enduring Freedom, Operation Iraqi Freedom, traumatic brain injury, posttraumatic stress disorder, war, polytrauma has been introduced to describe these more complex blast-related injuries. The RAND Corporation recently conducted a large representative sample survey (n ⫽ 1,965) of those who had been deployed as part of OEF/OIF. A random sampling methodology was used to assess exposure to various psychological and physical traumas, and injuries, and evaluate current symptoms (Tanielian & Jaycox, 2008). Trauma exposure was common. Fifty percent reported that they had a friend who was seriously wounded or killed, 45% indicated that they saw dead or seriously injured noncombatants, and over 10% reported that they were injured and required hospitalization. Frequency of trauma events was found to be even more common in a New England Journal of Medicine study (Hoge et al., 2004), in which over 90% of service members surveyed upon returning from Iraq reported being shot at or seeing dead bodies or human remains, and over 80% reported knowing someone who was seriously injured or killed. The RAND survey found that approximately 19% of returning service members met criteria for either posttraumatic stress disorder (PTSD) or depression (Tanielian & Jaycox, 2008); these numbers are similar to those reported by Hoge and colleagues (Hoge, Auchterlonie, & Milliken, 2006). As might be expected, there was a strong relationship between combat trauma experiences and PTSD. The development of PTSD was also significantly associated with having been wounded or injured (Hoge et al., 2004). Both the RAND survey (Tanielian & Jaycox, 2008) and Hoge and colleagues (2008) found relatively high rates of probable mild traumatic brain injury (TBI) or concussions, 19.5% and 15.2%, respectively. Concussion and psychological comorbidities were also common in both studies. RAND survey results suggest that Since October 2001, approximately 1.64 million U.S. troops have been deployed to Operation Enduring Freedom and Operation Iraqi Freedom (OEF/OIF) in Afghanistan and Iraq. A significant number have had multiple deployments. Service members in these environments experience not only traditional combat firefights with insurgents, but also the chronic threat of roadside bombs and improvised explosive devices (IEDs). In OEF/OIF, research suggests that 75% of combat injuries result from such explosive munitions (Owens et al., 2008). As a result of this increasingly common mechanism of injury, as well as improvements in body armor and surgical stabilization on the front-line of combat, more war-wounded are returning with multiple complex injuries in unpredictable patterns (Gawande, 2004). Common conditions in multiple combinations include open wounds; traumatic brain; spinal cord, eye, ear, and musculoskeletal injuries; traumatic amputations; and mental health problems. The term polytrauma Lisa A. Brenner, VA VISN 19 Mental Illness Research, Education, and Clinical Center (MIRECC); Departments of Psychiatry, Neurology, and Physical Medicine and Rehabilitation, University of Colorado Denver, School of Medicine, Denver, CO; Rodney D. Vanderploeg, James A. Haley VA Medical Center; Departments of Psychology and Psychiatry and Behavioral Medicine, University of South Florida; Defense and Veterans Brain Injury Center, Tampa, FL; Heidi Terrio, Department of Deployment Health and Headquarters, Evans Army Community Hospital; Defense and Veterans Brain Injury Center, Fort Carson, CO. Correspondence concerning this article should be addressed to Lisa A. Brenner, VA VISN 19 MIRECC, 1055 Clermont Street, MIRECC, Denver, CO 80220. E-mail: [email protected] 239 240 BRENNER, VANDERPLOEG, AND TERRIO over a third of those who experienced a probable TBI had cooccurring depression (Tanielian & Jaycox, 2008). Hoge et al. (2008) found that of those with a probable concussion (combining the LOC and the alteration of consciousness groups), 32.6% also had PTSD. When this military cohort presents to the Veterans Health Administration (VHA), these comorbidities continue. One study found that 42% of OEF/OIF veterans with a mild TBI history also had PTSD symptoms (Lew et al., 2008). Department of Defense (DoD) and Department of Veterans Affairs (VA) System of Care Developments for the OEF/OIF Cohort To enhance early identification and treatment of physical and mental health concerns both the DoD and VA have implemented screening procedures. The DoD instituted Post-Deployment Health Assessment (PDHA) and Reassessment (PDHRA) programs. The PDHA is scheduled with trained health care providers within 30 days after returning to home or to a military processing station. The purpose is to review each service member’s current health, mental health, or psychosocial issues commonly associated with deployments, possible deployment-related occupational and environmental exposures (including TBI, which was added in 2008), and to discuss deployment-related health concerns. Positive responses require supplemental assessment and/or referrals for medical consultation. Similarly, the PDHRA is designed to identify and address health concerns, with specific emphasis on mental health, that have emerged over time since deployment. The PDHRA should be completed within the 3- to 6-month time period after return from deployment, ideally at the 3- to 4-month mark because many transitions occur between 90 and 120 days. An influx of young OEF/OIF combat veterans has been presenting to VA medical centers with overlapping physical injuries and mental health and substance use conditions. Headaches and various musculoskeletal pain (including low back pain) are also common. In an effort to assure appropriate, effective, and timely care the VHA developed a comprehensive and integrated system of care to treat polytrauma patients. As one entry point, in December 2005, the VHA established a series of national clinical reminders in the Computerized Patient Record System (CPRS) for screening veterans who seek care within the VHA upon their return from OEF/OIF. These reminders target problems in the areas of PTSD, depression, alcohol abuse, infectious diseases, and chronic symptoms. In April 2007, an additional mandatory clinical reminder for TBI was added to this CPRS-based postdeployment screening process. Nationally mandated clinical reminders help clinicians identify populations at risk and to standardize care. The implementation of care that includes system-wide screening, standardized assessment and treatment planning, computerized templates, and practice guidelines has been shown to improve outcomes (e.g., California Acute Stroke Pilot Registry Investigators, 2005; Lesho, Myers, Ott, Winslow, & Brown, 2005); however, there are still a number of challenges to overcome. This article describes obstacles related to accurate assessment and diagnosis of multiple comorbid conditions, with a particular focus on mild TBI history with enduring symptoms and PTSD, and offers a conceptual model with assessment and treatment planning implications. Military Mind-set and Resultant Biases Despite the high rates of psychological symptoms and diagnoses in OEF/OIF troops, there are unique factors in the military that contribute to resistance to seeking help. One concern is possible underreporting of symptoms and problems immediately following deployment. For example, Milliken and colleagues (Milliken, Auchterlonie, & Hoge, 2007) found the rates of reported depression and PTSD approximately doubled between the immediate Iraqi PDHA and the subsequent PDHRA. Hypotheses used to explain this phenomenon include the possibility that soldiers believe that if they report problems during postdeployment assessment they will be kept on base longer, rather than being allowed to return home to their families; therefore, they deny symptoms and behavior changes even if they are aware of them. A second hypothesis is that immediately following deployment military personnel are in a type of honeymoon period during which they believe that any current symptoms are minor and will disappear once they are back in their home environments. When that does not happen and new family and relationship readjustment problems emerge, soldiers admit to problems initially minimized or denied. Family members may also encourage help seeking behavior. In addition, military personnel may not recognize symptoms until they are back in their home environments. This may be related to the less structured nature of their civilian lives (e.g., increased options regarding daily activities). Other research has demonstrated fear of stigmatization as a barrier to seeking mental health services. Military personnel are concerned about how they will be perceived by their peers and leadership. These concerns are substantially more prevalent than negative beliefs about effectiveness of treatment (Hoge et al., 2004). The finding that these fears about being stigmatized are more than twice as high in individuals who have mental health conditions (50%– 65%) than in those who do not (20%–33%) is troubling. As a result, it is not surprising that within the OEF/OIF active duty cohort with psychological disorders only 23% to 40% reported having received professional help in the past year. Consistent with these findings are anecdotal reports that when OEF/ OIF veterans are evaluated at VA medical centers they are accepting of diagnoses of physical injuries and TBI, yet are resistant to diagnoses of PTSD or depression. Anecdotal reports also indicate that veterans may be more likely to follow through on referrals for TBI-related intervention (e.g., neuropsychological consultation and various rehabilitation therapies—speech, occupational, cognitive remediation, or cognitive aids and devices) than they are for mental health-related services. Factors Complicating Accurate Assessment and Diagnosis There are many factors that complicate accurate assessment and diagnoses of OEF/OIF veterans presenting to health care professionals. These include the following: (a) patient and health care provider misinformation regarding TBI; (b) delayed clinical presentation of the patient which may in part be related to in-theater assessment barriers; (c) exposure to numerous potentially injurious events; (d) multiple symptoms common across various diagnoses or simply associated with deployment-related stress; and (e) mental health comorbidities in addition to a history of mild TBI. MILD TBI, PTSD, AND POLYTRAUMA COMORBIDITY Health Care Misinformation Blast exposure. There appears to be a common misconception among soldiers/veterans, the news media, and some health care providers that exposure to a blast event means that a person sustained a TBI. This is incorrect. Exposure can mean multiple things. One soldier may see a Humvee three vehicles in front of his going over an exploding roadside bomb, but not experience any direct or indirect physical effect of the explosion. Another soldier could be in the first Humvee under which the bomb exploded and sustain a broken leg and ruptured tympanic membrane from the force of the blast, and be knocked unconscious for several minutes. While the first soldier did not experience a TBI, the second did. Diagnosis of TBI. The tendency to conceptualize TBI screening and diagnosis as synonymous contributes to current misconceptions regarding the exact definition of a TBI. Schwab et al. (2007) discuss TBI screening as a means of triage to facilitate evaluation, diagnosis, treatment, and/or education. Therefore, screening usually consists of one or more questions aimed at identifying individuals at risk for having a condition, not diagnosing a condition, per se. Diagnostically, to have sustained a TBI an individual must have experienced an external physical force that resulted in a traumatically induced structural injury to the brain, or a physiological disruption of brain function indicated by medical findings such as positive neuroimaging, or an acute alteration in consciousness. Such findings may range from immediate confusion and disorientation to unconsciousness (see Table1). Whereas hospital records and/or neuroimaging findings may assist with the historical diagnosis of more severe and/or acute injury, the “gold standard” for determining prior TBI is patient self-report, facilitated by structured or in-depth clinical interview (Corrigan & Bogner, 2007, p. 316). Thus, a TBI is an injurious historical event. Current symptoms months later are irrelevant to correctly making the diagnosis. Not having current symptoms does not mean that the person did not experience a TBI. At the same time, having current Table 1 Departments of Defense and Veterans Affairs Consensus Definition of Traumatic Brain Injury (Department of Veterans Affairs and Department of Defense, 2009) A traumatically induced structural injury and/or physiological disruption of brain function as a result of an external forcea that is indicated by new onset or worsening of at least one of the following clinical signs, immediately following the event: 1. Any period of loss of or a decreased level of consciousness; 2. Any loss of memory for events immediately before or after the injury (posttraumatic amnesia); 3. Any alteration in mental state at the time of the injury (confusion, disorientation, slowed thinking, etc.) (alteration of consciousness/ mental state); 4. Neurological deficits (weakness, balance disturbance, praxis, paresis/plegia, sensory loss, aphasia, etc.) that may or may not be transient; 5. Intracranial lesion. Note. a External forces may include the following: the head being struck by an object, the head striking an object, the brain undergoing an acceleration/deceleration movement without direct external trauma to the head, a foreign body penetrating the brain, forces generated from events such as a blast or explosion, or other forces yet to be defined. 241 symptoms such as headaches, dizziness, memory problems, and irritability does not mean a person had a TBI. Such symptoms may be related to the TBI, but may also be associated with other factors and conditions. For example, Schneiderman, Braver, and Kang (2008) presented findings which suggest that mild TBI and PTSD are independently significantly associated with soldier endorsement of three or more postconcussive symptoms. Adjusted prevalence ratios for such symptoms in those with mild TBI or PTSD were 1.50 and 3.71, respectively. In OEF/OIF military personnel, the majority of those with a deployment-acquired TBI sustained a mild injury. That is, neuroimaging was negative, there were no neurological deficits, and the alteration of consciousness was typically brief, with a period of being dazed and confused lasting minutes to several hours. At worst, loss of consciousness was generally less than 30 min (see Table 2). Confusing the clarity of the definition/diagnosis of TBI is the criterion of “an alteration of consciousness,” which in this context is defined as a disruption of brain functioning from a physical trauma. A TBI alteration of consciousness (i.e., confusion, disorientation, incoherency at the scene of the event) is different from a psychological alteration of consciousness, although they may be difficult to distinguish, particularly if information is being obtained months later. Most individuals who are close to an unexpected explosion in which they may feel the ground move or environmental debris such as sand hit their skin will have an adrenalin rush and experience an alteration of consciousness—fear, anxiety, alteration of attention, and/or change in environmental awareness. This is a typical psychological response. However, this type of alteration of consciousness does not reflect a physiological disruption of brain functioning and would not mean that the person sustained a TBI. Careful clinical interviewing is necessary to tease apart these two types of altered consciousness. Asking a soldier to compare a blast-related consciousness-altering event to other combat events in which there clearly was not a physical force to the body may be useful (e.g., comparing subjective experiences between a combat firefight and a blast event). In addition, emerging research regarding associations between readily identifiable physical injuries and history of mild TBI may inform assessment practices. For example, Xydakis and colleagues (2007) found a significant association between barotraumatic tympanic membrane perforation and concussive brain injury. They suggested that medical providers “treating blast survivors with tympanic-membrane perforation need to have a high index of suspicion for concomitant neurologic injury” (p. 831). Postconcussive symptoms and postconcussive syndrome (PCS). A TBI is a historical injurious event; however, postconcussive symptoms or PCS reflect a set of physical/somatic, cognitive, and emotional symptoms which began or worsened immediately after the TBI event. These symptoms include the following: headaches, dizziness, fatigue, disordered sleep, concentration problems, memory problems, slowed thinking, depression, anxiety, and irritability. The immediate onset and presence of these symptoms in the minutes and days after the TBI event increases the likelihood that a TBI occurred. However, their presence does not mean that a TBI occurred if the immediate event did not result in either a structural lesion to the brain or an immediate physiological disruption of brain functioning (e.g., unconsciousness, memory gaps, or being dazed, confused, and/or disoriented). For example, injuries to the shoulders and neck may result in subsequent headaches, and as- BRENNER, VANDERPLOEG, AND TERRIO 242 Table 2 Departments of Defense and Veterans Affairs Consensus-Based Classification of Closed Traumatic Brain Injury Severity (Department of Veterans Affairs and Department of Defense, 2009) Criteria Structural imaging Loss of consciousness Alteration of consciousness/mental stateⴱ Posttraumatic amnesia Glasgow Coma Scale (best available score in first 24 hr) Mild Moderate Severe Normal 0–30 min Normal or abnormal ⬎30 min and ⬍24 hr Normal or abnormal ⬎24 hr A moment up to 24 hr 0–1 days ⬎24 hr; severity based on other criteria ⬎1 day and ⬍7 days ⬎7 days 13-15 9-12 ⬍9 ⴱ Alteration of mental status must be immediately related to the trauma to the head. Typical symptoms would be looking and feeling dazed and uncertain of what is happening, confusion, difficulty thinking clearly or responding appropriately to mental status questions, and being unable to describe events immediately before or after the trauma event. sociated psychological trauma may result in anxiety, insomnia, fatigue, and problems with concentration and memory (i.e., common stress adjustment or PTSD symptoms). In fact, one study (Hoge, Terhakopian, Castro, Messer, & Engel, 2007) found that somatic symptoms, including some often associated with mild TBI (e.g., headache, dizziness), were more frequently endorsed by military personnel who screened positive for PTSD than by those who did not. No postconcussive symptom is unique to or diagnostic of a TBI. In the majority of patients with mild TBI, these postconcussive symptoms last less than a day or gradually decrease and disappear over the course of several weeks. Neuropsychological recovery is typically complete by 1 month after injury (Belanger, Curtiss, Demery, Lebowitz, & Vanderploeg, 2005; Belanger & Vanderploeg, 2005; Schretlen & Shapiro, 2003). The etiology for persistent postconcussive symptoms (months and years postinjury) remains to be determined. However, research has shown that symptom persistence is more related to psychological, social, and motivational factors than to acute injury characteristics (McCrea et al., 2008). Numerous studies have reported that postconcussive symptoms are quite common among individuals with various medical or psychological disorders (Fox, Lees-Haley, Earnest, & Dolezal-Wood, 1995; Iverson & McCracken, 1997). In addition, pre-existing or comorbid psychiatric difficulties have been shown to be important moderators of persistent postconcussive symptoms (Greiffenstein & Baker, 2001; King, 1996; Luis, Vanderploeg, & Curtiss, 2003). Findings that mild TBI increases the risk for developing subsequent psychiatric conditions (Fann et al., 2004; Vanderploeg, Curtiss, Luis, & Salazar, 2007), and that pain syndromes and sleep problems are significantly associated with postconcussive syndrome (Nicholson, 2000; Perlis, Artiola, & Giles, 1997) further complicate clinical presentation and treatment considerations. Delayed Presentation for Health Care and Exposure to Multiple Potentially Injurious Events Military personnel going through a PDHA or VHA patients who screen positive on any OEF/OIF health care clinical reminders are typically presenting from several months to a year or more following deployment. If TBI screening is positive, the TBI event typically occurred many months earlier. Obtaining a careful history regarding details of the potentially injurious event, any eventrelated loss or alteration of consciousness, and immediate and emerging symptoms over the subsequent hours and days is extremely difficult. Patients’ memories have faded and merged with many other deployment-related experiences. Veterans often describe multiple historical events in which a TBI may have occurred. Most of these events are also psychologically traumatizing, may be associated with recurrent intrusive thoughts or nightmares, or discussion of them may be associated with increased anxiety and physiological arousal (i.e., PTSD symptomology). Furthermore, many veterans describe chronic sleep disturbances and fatigue throughout their deployment, as well as headaches and back pain from physical activities and carrying heavy equipment. Most view these symptoms as part and parcel of their deployment, and consider them a shared experience with their peers. Asking them to attempt to ascribe onset or worsening of symptoms to particular events in time is problematic. Clinicians report that when discussing one blast event with a veteran during which there may have been a brief alteration of consciousness or some minor memory gaps, veterans will say, “but that was not the worst event.” When then asked to describe the worst event, veterans will describe a clearly psychologically traumatizing event in which there were numerous injuries or deaths among others (civilians and military troops), but during which the veteran in question was clearly not physically injured. Thus, within the veteran’s mind, physically traumatic/injurious and psychologically traumatic/injurious are often merged and overlapping constructs. Multiple Symptoms and Patterns of Overlap Across Various Comorbidities The classic use of symptoms to make accurate diagnoses is to carefully track the onset and course of symptoms, including factors that exacerbated or diminished their severity. In the OEF/OIF cohort with delayed clinical presentation and multiple events that may have resulted in a mild TBI or posttraumatic stress, it is difficult to tease apart historical details and symptom onset and course to determine whether a TBI actually occurred. In contrast, even with delayed clinical presentation, using current symptoms to MILD TBI, PTSD, AND POLYTRAUMA COMORBIDITY determine whether a veteran meets criteria for various mental health conditions (e.g., PTSD, depression, substance use disorder, etc.) may be less problematic. Yet, because of potential comorbidities and/or the late onset of symptoms, clinical presentations may be atypical. Moreover, parsing out the percent of current symptoms due to various comorbid conditions is not possible. Findings from Terrio and colleagues (Terrio et al., 2009) help illustrate this point. They presented data on self-reported symptom onset and course in soldiers identified as having had a mild TBI during OIF deployment. Figure 1, adapted from their data, demonstrates the initial postconcussive symptoms and the pattern of improvement between event and postdeployment assessment months later. Postconcussive complaints of headache and dizziness were common acutely, but showed resolution in a large majority of soldiers. In contrast, irritability and memory problems were reported less frequently acutely and appear to show minimal resolution. However, other findings from Terrio and colleagues indicate that at least half of current postdeployment irritability and memory problems may not be related to soldiers’ history of mild TBI and may reflect other deployment-related factors (see Figure 2). Surprisingly, even 38% of current postdeployment complaints of balance difficulties were unrelated to any history of prior mild TBI, although its exact etiology is unclear from these data. Patterns of symptom overlap could potentially help differentiate etiologies across comorbid conditions. However, this does not appear to be the case. Using the Vietnam Experience Study data set, Vanderploeg and colleagues (Vanderploeg, Belanger, & Curtiss, 2009) compared participants who had experienced a history of mild TBI years earlier (n ⫽ 278) with those meeting criteria for a current diagnosis of PTSD (n ⫽ 249). Current frequencies of nine common postconcussive symptoms were examined: sleep problems, fatigue, irritability, headaches, dizziness, memory problems, concentration problems, sadness/depressed mood, and anxiety. Low back pain also was included given its common complaint in the OEF/OIF cohort. In both the mild TBI and the PTSD groups the two most frequently endorsed symptoms were sleep problems and irritability: mild TBI – sleep ⫽ 45%, irritability ⫽ 40%; PTSD – sleep ⫽ 66%, irritability ⫽ 64%. In the mild TBI group, the next three most frequent symptoms were fatigue ⫽ 39%, low back pain ⫽ 36%, and memory problems ⫽ 29%; while in the PTSD group they were low back pain ⫽ 48%, concentration ⫽ 45%, and fatigue ⫽ 41%. All symptoms were more frequent in the PTSD 90% 80% Acute (right after mTBI) 70% Post-Deployment 60% 50% 40% 30% 20% 10% 0% Headache Dizziness Balance Problems Irritability Memory Problems Figure 1. Fort Carson: Postdeployment data (n ⫽ 907). mTBI ⫽ mild traumatic brain injury. 243 90% 80% Post-deployment Onset (New Sx) 70% Persistent Sx since TBI 60% 50% 40% 30% 20% 10% 0% Headache Dizziness Balance Problems Irritability Memory Problems Figure 2. Currently symptomatic: Onset of symptoms (n ⫽ 844). TBI ⫽ traumatic brain injury; Sx ⫽ symptoms. group than the mild TBI group, and more frequent in both these groups than in the healthy control subjects. Patterns of symptom overlap were examined in both clinical groups. Sleep problems had the highest degree of overlap with other symptoms, suggesting that sleep problems may drive or sustain the other symptoms. If this is the case, treating sleep problems first may result in substantial improvement in all reported symptoms. Postdeployment Clinical Presentation: An Accumulative Condition of Adversity Burden Of significant concern is how to best help war veterans maintain or return to previous levels of functioning. Based upon the information presented above, clinicians are being asked to facilitate this process in the context of multiple diagnostic and treatment-related questions. It has even been hypothesized that current processes (i.e., TBI screening) could contribute to poor outcomes by creating potential iatrogenic consequences (Hoge et al., 2008). However, existing literature regarding the cumulative impact of adversities (O’Rand, 1996; Price, Risk, Haden, Lewis, & Spitznagel, 2004; Séguin et al., 2007) both supports the importance of identifying deployment-related conditions and symptoms and suggests that an alternate clinical approach may be indicated. The idea of cumulative disadvantage was introduced by Merton (1968) who identified disparities between career trajectories of scientists who received early advantages versus those who did not. Merton later noted that “differences in individual capabilities aside . . . processes of accumulative advantage and disadvantage accentuate inequalities in science and learning: inequalities in peer recognition, inequalities of access to resources, and inequalities of scientific productivity” (Merton, 1988, p. 616). Analyzing life course trajectories of older adults, O’Rand (1996) suggested that “patterns of inequality” transpired over time secondary to the interaction between institutional mechanisms and individual difference. She suggested this interplay resulted in increasing heterogeneity and inequality between aging cohorts. The theory has also been used to explain how an accumulation of disadvantaged genetic and/or environmental factors (Preston, Hill, & Drevenstedt, 1998) can result in a cascade of physical and psychiatric risk (Ferraro & Kelley-Moore, 2003; Morgan et al., 2008; O’Rand, 1996; Séguin et al., 2007). 244 BRENNER, VANDERPLOEG, AND TERRIO In a recent article, Séguin and colleagues (2007) explored the cumulative impact of psychosocial factors across the life trajectory to “delineate pathways” of those who died by suicide. The researchers identified two distinct life trajectories among those who engaged in lethal suicidal behavior: (1) individuals who experienced significant childhood adversities and were more likely to present with personality disorders; and (2) those with lives marked by fewer adversities but who contended with major “difficulties” later in life. In exploring means of suicide prevention for those in the first trajectory, the authors noted the importance of “reducing childhood adversities and promoting resiliency.” They suggested that this in part could be accomplished via early intervention. Moreover, in exploring the role of PTSD and drug dependence in nonfatal suicide, Price and colleagues (2004) suggested that the impact of psychiatric comorbidities can be cumulative. Findings documented potential causal roles involving PTSD, drug dependence, and suicidality over the course of a lifetime. The authors concluded that interventions aimed to reduce suicidality should include treatment of substance abuse and depression. Increasing coping strategies was also suggested as being potentially useful, thereby supporting the idea that addressing specific symptoms or problems early may decrease longterm negative outcomes. Cumulative Disadvantage and OEF/OIF Veterans Ruff et al. (Ruff, Camenzuli, & Mueller, 1996) discuss a similar “cumulative model” regarding postconcussive disorder in which difficulties with physical, emotional, cognitive, psychosocial, vocational, financial, and recreational functioning are viewed as stressors that exacerbate premorbid factors and result in increased disability (Evered, Ruff, Baldo, & Isomura, 2003). Likewise, King (2008) suggests that if mild TBI and PTSD conditions are present, they can be “mutually exacerbating.” In terms of OEF/OIF veterans, such cumulative models may provide a theoretical basis from which to conceptualize the current difficulties reported by returning soldiers with co-occurring mild TBI and PTSD. This theory would also suggest that individuals with both conditions may be at increased risk for poor long-term physical and health-related outcomes. Consistent with this, Vanderploeg et al. (2009) found that in those with PTSD, subsequently sustaining a mild TBI significantly decreased the rate of PTSD recovery. Over a 16-year window of time, approximately 69% of those without a subsequent mild TBI recovered from their PTSD, while only 48% of those who subsequently sustained a mild TBI recovered from PTSD. Early assessment and treatment is indicated in order to alter negative life course trajectories. With this theory in mind, evaluation of deployment-related TBI and associated sequelae has utility both in terms of identifying symptoms that require immediate attention and documenting life events which may contribute to an individual’s overall burden of adversity. The advantage of symptom identification and symptom-based treatment altering a negative life course trajectory outweighs potential short- and long-term problems of misdiagnosis or missed diagnosis. Short-term symptoms related to a history of mild TBI and PTSD (e.g., headaches, dizziness, irritability) would be expected to impact psychosocial functioning. Based upon the cumulative disadvantage model, long term symptoms could be mutually exacerbating and ultimately precipitate engagement in detrimental behaviors (e.g., substance abuse), the onset of additional conditions (physical and/psychological), and negative psychi- atric outcomes (e.g., suicide). Formal application of this model to returning military personnel is indicated and may provide evidence that could be used to guide best practices. In terms of the DoD screening, current processes in place at Fort Carson have been cited as a model (Bradshaw, 2007). Evaluation at this facility includes use of standard TBI screening questions (the Warrior Administered Retrospective Casualty Assessment Tool [WARCAT]) followed by clinical interview (Schwab et al., 2007; Terrio et al., 2009). The WARCAT gathers soldier selfreport data (e.g., injury history, protective gear, the nature of the explosive mechanisms involved) and provides a template for the structured clinical interview. This timely and comprehensive process eliminates the redundancy of multiple screening efforts and allows for information obtained to be placed in soldier medical records. Inherent to the process at Fort Carson is differentiating between TBI history and associated symptoms, and providing soldiers with education and the expectation for recovery. Similarly, TBI screening within the VA is focused only on symptomatic individuals; follow-up services address existing veteran concerns regardless of etiology and support the expectation for recovery. The importance of educating individuals regarding the positive expectation for recovery after TBI was highlighted by a recent study that found that patient perceptions about the severity and future duration of their postconcussion symptoms early after injury was associated with positive outcomes (Whittaker, Kemp, & House, 2007). Moreover, Ponsford and colleagues (2002) found that civilians who received early intervention (increased monitoring and education) following a mild TBI reported fewer symptoms than those who did not receive such augmented care. Conducting early screenings and providing education for war veterans about TBI symptoms and the expectation for recovery should decrease poor outcomes. However, to date the effectiveness of education with soldiers and/or veteran whose injuries were sustained months to years earlier is untested. Further research in this area is indicated. TBI screening processes can also be used to identify comorbidities and provide an opportunity for intervention which military personnel and veterans may be more willing to accept because of lower levels of associated stigma. However, at present there is a dearth of evidence-based treatments for co-occurring TBI and PTSD (Soo & Tate, 2007). To address overlapping mild TBI and PTSD symptoms, regardless of etiology, an alternate clinical approach is indicated. Terrio and colleagues (2009) discuss the concept of identifying and addressing symptoms in a stepwise fashion. As is suggested in Figure 3 (Terrio, 2009), treatment at COGNITIVE ISSUES IRRITABILITY / IMPULSIVITY SOMATIC COMPLAINTS SELF-CARE ROUTINES* BEHAVIORAL HEALTH ISSUES EDUCATION: Expectaon of Recovery Figure 3. Traumatic brain injury step-care treatment model. *Includes sleep hygiene, diet, exercise, and avoiding further traumatic brain injury. MILD TBI, PTSD, AND POLYTRAUMA COMORBIDITY Fort Carson includes providing soldiers and their family members with the expectation for recovery and simultaneously addressing psychiatric symptoms (e.g., depression) first regardless of origin. Next steps include attending to somatic complaints (e.g., headaches) and self-care routines (e.g., sleep). Interventions focused on cognitive symptoms (e.g., memory loss) are not generally initiated until the above-stated symptoms are sufficiently addressed. Educating soldiers and their family members about the potential interplay between symptoms and the importance of monitoring symptoms and recommended interventions is inherent to the process. This approach is consistent with recently released mild TBI clinical practice guidelines (Department of Veterans Affairs & Department of Defense, 2009). Ultimately, this strategy is aimed at helping military personnel and veterans maintain or return to their social roles, thereby facilitating resilience in much the same manner as discussed by Séguin et al. (2007). Successful implementation of this step-care treatment model is likely to result in decreased utilization of medical services and disability benefits. Overall, the above-described approach supports recovery, health promotion, and enhanced resiliency. Moreover, struggles related to getting better, frequently referred to as secondary gain, could be addressed in treatment as barriers to recovery. Conclusions This article presented challenges related to the assessment and treatment of military personnel and veterans with a co-occurring history of mild TBI with persistent symptoms and PTSD. As noted above, factors complicating assessment, diagnosis, and treatment are diverse and multifaceted (e.g., military mindset and resultant biases, multiple symptoms and patterns of overlap across comorbidities). The existing literature regarding cumulative disadvantage may help to increase understanding regarding the complex and varied symptom patterns reported by those with comorbid conditions, and the importance of early screening and intervention. The authors would like to suggest that best practices include treating symptoms regardless of etiology to decrease military personnel and veteran burden of adversity. At the same time, further research is indicated to explore evidence-based treatments for those with co-occurring disorders, the impact in this cohort of delayed mild TBI education regarding the expectation for recovery, and the applicability of cumulative disadvantage theory to returning OEF/ OIF military personnel and veterans. References Belanger, H. G., Curtiss, G., Demery, J. A., Lebowitz, B. K., & Vanderploeg, R. D. (2005). Factors moderating neuropsychological outcomes following mild traumatic brain injury: A meta-analysis. Journal of the International Neuropsychological Society, 11, 215–227. Belanger, H. G., & Vanderploeg, R. D. (2005). The neuropsychological impact of sports-related concussion: A meta-analysis. Journal of the International Neuropsychological Society, 11, 345–357. Bradshaw, D. (2007). Traumatic brain injury (TBI) task force report recommendation summary. Washington, DC: Department of the Army. California Acute Stroke Pilot Registry Investigators. (2005). The impact of standardized stroke orders on adherence to best practices. Neurology, 65, 360 –365. Corrigan, J. D., & Bogner, J. (2007). Screening and identification of TBI. Journal of Head Trauma Rehabilitation, 22, 315–317. 245 Department of Veterans Affairs and Department of Defense. (2009). VA/ DOD clinical practice guideline for management of concussion/mild traumatic brain injury. Retrieved June 15, 2009, from http://www .healthquality.va.gov/mtbi/concussion_mtbi_full_1_0.pdf Evered, L., Ruff, R., Baldo, J., & Isomura, A. (2003). Emotional risk factors and postconcussional disorder. Assessment, 10, 420 – 427. Fann, J. R., Burington, B., Leonetti, A., Jaffe, K., Katon, W., & Thompson, R. S. (2004). Psychiatric illness following traumatic brain injury in and adult health maintenance organization population. Archives of General Psychiatry, 61, 53– 61. Ferraro, K. F., & Kelley-Moore, J. A. (2003). Cumulative disadvantage and health: Long-term consequences of obesity? American Sociological Review, 68, 707–729. Fox, D. D., Lees-Haley, P. R., Earnest, K., & Dolezal-Wood, S. (1995). Base rates of postconcussive symptoms in health maintenance organization patients and controls. Neuropsychology, 4, 606 – 611. Gawande, A. (2004). Casualties of war-military care for the wounded from Iraq and Afghanistan. New England Journal of Medicine, 351, 2471– 2475. Greiffenstein, F. M., & Baker, J. W. (2001). Comparison of premorbid and postinjury MMPI-2 profiles in late postconcussion claimants. Clinical Neuropsychologist, 15, 162–170. Hoge, C. W., Auchterlonie, J. L., & Milliken, C. S. (2006). Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. Journal of the American Medical Association, 295, 1023–1032. Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., & Koffman, R. L. (2004). Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine, 351, 13–22. Hoge, C. W., McGurk, D., Thomas, J. L., Cox, A. L., Engel, C. C., & Castro, C. A. (2008). Mild traumatic brain injury in U.S. soldiers returning from Iraq. New England Journal of Medicine, 358, 453– 463. Hoge, C. W., Terhakopian, A., Castro, C. A., Messer, S. C., & Engel, C. C. (2007). Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. American Journal of Psychiatry, 164, 150 –153. Iverson, G. I., & McCracken, L. M. (1997). Postconcussive symptoms in persons with chronic pain. Brain Injury, 11, 783–790. King, N. S. (1996). Emotional, neuropsychological, and organic factors: Their use in prediction of persisting postconcussion symptoms after moderate and mild head injuries. Journal of Neurology, Neurosurgery, and Psychiatry, 61, 75– 81. King, N. S. (2008). PTSD and traumatic brain injury: Folklore and fact? Brain Injury, 22, 1–5. Lesho, E. P., Myers, C. P., Ott, M., Winslow, C., & Brown, J. E. (2005). Do clinical practice guidelines improve processes or outcomes in primary care? Military Medicine, 170, 243–246. Lew, H. L., Vanderploeg, R. D., Moore, D. F., Schwab, K., Friedman, L., Yesavage, J., et al. (2008). Overlap of mild TBI and mental health conditions in returning OIF/OEF service members and veterans. Journal of Rehabilitation Research and Development, 45, x–xv. Luis, C. A., Vanderploeg, R. D., & Curtiss, G. (2003). Predictors for a postconcussion symptom complex in community dwelling male veterans. Journal of the International Neuropsychological Society, 9, 1001– 1015. McCrea, M., Pliskin, N., Barth, J., Cox, D., Fink, J., French, L., et al. (2008). Official position of the Military TBI Task Force on the role of neuropsychology and rehabilitation psychology in the evaluation, management and research of military veterans with traumatic brain injury. The Clinical Neuropsychologist, 22, 10 –26. Merton, R. K. (1968). The Matthew effect in science. Science, 159, 56 – 63. Merton, R. K. (1988). The Matthew effect in science, II. Cumulative 246 BRENNER, VANDERPLOEG, AND TERRIO advantage and the symbolism of intellectual property, ISIS, 79, 606 – 623. Milliken, C. S., Auchterlonie, J. L., & Hoge, C. W. (2007). Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. Journal of the American Medical Association, 298, 2141–2148. Morgan, C., Kirkbride, J., Hutchinson, G., Craig, T., Morgan, K., Dazzan, P., et al. (2008). Cumulative social disadvantage, ethnicity and firstepisode psychosis: A case-control study. Psychological Medicine, 38, 1701–1715. Nicholson, K. (2000). Pain, cognition and traumatic brain injury. NeuroRehabilitation, 14, 95–103. O’Rand, A. M. (1996). The precious and the precocious: Understanding cumulative disadvantage and cumulative advantage over the life course. Gerontologist, 36, 230 –238. Owens, B. D., Kragh, J. F., Wenke, J. C., Macaitis, J., Wade, C. E., & Holcomb, J. B. (2008). Combat wounds in Operation Iraqi Freedom and Operation Enduring Freedom. Journal of Trauma, 64, 295–299. Perlis, M. L., Artiola, L., & Giles, D. E. (1997). The incidence sleep complaints in minor head injured individuals. Perceptual and Motor Skills, 84, 595–599. Ponsford, J., Willmott, C., Rothwell, A., Cameron, P., Kelly, A. M., Nelms, R., et al. (2002). Impact of early intervention on outcome following mild traumatic brain injury in adults. Journal of Neurology, Neurosurgery and Psychiatry, 73, 330 –332. Preston, S. H., Hill, M. E., & Drevenstedt, G. L. (1998). Childhood conditions that predict survival to advanced ages among African–Americans. Social Science and Medicine, 47, 1231–1246. Price, R. K., Risk, N. K., Haden, A. H., Lewis, C. E., & Spitznagel, E. L. (2004). Post-traumatic stress disorder, drug dependence, and suicidality among male Vietnam veterans with a history of heavy drug use. Drug and Alcohol Dependence, 76, S31– 43. Ruff, R. M., Camenzuli, L., & Mueller, J. (1996). Miserable minority: Emotional risk factors that influence the outcome of a mild traumatic brain injury. Brain Injury, 10, 551–565. Séguin, M., Lesage, A., Turecki, G., Bouchard, M., Chawky, N., Tremblay, N., et al. (2007). Life trajectories and burden of adversity: Mapping the developmental profiles of suicide mortality. Psychological Medicine, 37, 1575–1583. Schneiderman, A. I., Braver, E. R., & Kang, H. K. (2008). Understanding sequelae of injury mechanisms and mild traumatic brain injury incurred during the conflicts in Iraq and Afghanistan: Persistent postconcussive symptoms and posttraumatic stress disorder. American Journal of Epidemiology, 167, 1446 –1452. Schretlen, D. J., & Shapiro, A. M. (2003). A quantitative review of the effects of traumatic brain injury on cognitive functioning. International Review of Psychiatry, 15, 341–349. Schwab, K. A., Ivins, B., Cramer, G., Johnson, W., Sluss-Tiller, M., Kiley, K., et al. (2007). Screening for traumatic brain injury in troops returning from deployment in Afghanistan and Iraq: Initial investigation of the usefulness of a short screening tool for traumatic brain injury. Journal of Head Trauma Rehabilitation, 22, 377–389. Soo, C., & Tate, R. (2007). Psychological treatment for anxiety in people with traumatic brain injury. Cochrane Database of Systematic Reviews, 3, CD005239. Tanielian, T., & Jaycox, L. H. (Eds.). (2008). Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation. Terrio, H. (2009, April). TBI screening: Evaluation and initial treatment. Presented at Grand Rounds at Brooke Army Medical Center, San Antonio, TX. Terrio, H., Brenner, L. A., Ivins, B. J., Cho, J. M., Helmick, K., Schwab, K., et al. (2009). Traumatic brain injury screening: Preliminary findings in a U.S. army brigade combat team. Journal of Head Trauma Rehabilitation, 24, 14 –23. Vanderploeg, R. D., Belanger, H. G., & Curtiss, G. (2009, June). Patterns of symptom overlap in mild TBI and PTSD: Implications for treatment. Paper presented at the Annual Meeting of the American Academy of Clinical Neuropsychology, San Diego, CA. Vanderploeg, R. D., Belanger, H. G., & Curtiss, G. (2009). Mild traumatic brain injury and posttraumatic stress disorder and their associations with health symptoms. Archives of Physical Medicine and Rehabilitation, 90, 1084 –1093. Vanderploeg, R. D., Curtiss, G., Luis, C. A., & Salazar, A. M. (2007). Long-term morbidity and quality of life following mild head injury. Journal of Clinical and Experimental Neuropsychology, 29, 585–598. Whittaker, R., Kemp, S., & House, A. (2007). Illness perception and outcome in mild head injury: A longitudinal study. Journal of Neurology, Neurosurgery and Psychiatry, 78, 644 – 646. Xydakis, M. S., Bebarta, V. S., Harrison, C. D., Conner, J. C., Grant, G. A., & Robbins, A. S. (2007). Tympanic-membrane perforation as a marker of concussive brain injury in Iraq. New England Journal of Medicine, 357, 830 – 831. Received May 7, 2009 Revision received June 20, 2009 Accepted June 22, 2009 䡲 E-Mail Notification of Your Latest Issue Online! Would you like to know when the next issue of your favorite APA journal will be available online? This service is now available to you. Sign up at http://notify.apa.org/ and you will be notified by e-mail when issues of interest to you become available!