Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
American Journal of Epidemiology
Copyright O 1996 by The Johns Hopkins University School of Hygiene and Public Health
All rights reserved
Vol. 143, No. 9
Printed In U.S.A
Projecting Disease When Death Is Likely
Donald R. Hoover,1 Yun Peng,1 Alfred J. Saah,1 Roger R. Detels,2 Charles R. Rinaldo, Jr.,3 and
John P. Phair4
Projecting disease incidence, prevalence, and net morbidity is often needed when individuals are likely to
die, either disease free or after the disease has developed. Examples of this include remission of cancer or
heart disease in elderly people who can die from these or other causes and occurrence of a particular acquired
immune deficiency syndrome illness in human immunodeficiency virus type 1 (HIV-1) disease. Death is not an
ancillary event but, rather, indicates either an end to disease morbidity or an end to risk to ever develop that
disease. Thus, time to disease survival analyses that censor disease-free individuals at death can produce
misleading results. This paper describes several useful quantifications of disease and death for this setting. A
paradigm that utilizes Kaplan-Meier functions to estimate these quantities is introduced. The approach
anchors on a four-stage disease/death model: stage A, living without disease; stage B, dead without ever
developing disease; stage C, developed the disease and living; and stage D, dead after developing the
disease. An application is made to projecting cytomegalovirus disease in a cohort of HIV-1-infected users of
zidovudine and Pneumocystis prophylaxis from the Multicenter AIDS Cohort Study (MACS) during 1989-1993.
At 3 years after a CD4 + count below 100//U.I, a man had an 18.7%, 46.3%, 5.3%, or 29.9% chance,
respectively, to be in stage A, B, C, or D. This man, on average, had 0.28 years of cytomegalovirus morbidity
during these 3 years. Am J Epidemiol 1996;143:943-52.
competing risks; death; disease; incidence; Kaplan-Meier estimates; morbidity; prevalence
Projection of death and morbidity from a given
disease in individuals likely to die from that disease
and other causes is often needed. Relapses of cancer
and heart disease are often evaluated in elderly populations likely to die of many causes. Estimating the
occurrence of a given end stage complication of human immunodeficiency virus type 1 (HTV-1) infections, such as cytomegalovirus disease, Kaposi's sarcoma, and lymphoma, is also important. However,
persons with HTV-1 disease will often die first from
other HTV-1 disease complications without developing
the given end stage HTV-1 disease of interest.
In this setting, estimates of disease occurrence and
morbidity are needed to 1) evaluate current and
planned clinical practice, 2) allocate resources, 3) develop screening or counseling programs, and 4) plan
clinical trials for treatment and prophylaxis. Depending on the specific question of interest, different types
of estimates will be needed. For example, consider
1,000 people infected with HTV-1 being monitored for
cytomegalovirus disease. If the goal is to allocate
resources for the prophylaxis against or diagnosis of
the initial cytomegalovirus disease manifestation, then
the incidence of this disease (either as a fraction of the
original 1,000 or as a fraction of those alive at a given
time) is needed. If the goal is to allocate resources for
continuing treatment, then the prevalence of the disease (either as a fraction of the original cohort or
among those still living at a given time) is needed.
In this situation, death is informative. Death in a
person without (cytomegalovirus) disease indicates
that the person will never require resources for prophylaxis, diagnosis, or treatment of that disease. Death
in a person with disease means that the person has
been removed (by that disease or by other causes)
from the population that needs to be treated.
Few applications of relevant incidence and prevalence estimates in this setting have been made. Com-
Received for publication March 7,1995, and In final form July 24,
1995.
Abbreviations: AIDS, acquired immune deficiency syndrome;
HIV-1, human immunodeficiency virus type 1.
1
Department of Epidemiology, The Johns Hopkins University
School of Public Health, Baltimore, MD.
2
University of California, Schools of Public Health and Medicine,
Los Angeles, CA.
3
University of Pittsburgh Graduate School of Public Health,
Pittsburgh, PA.
4
Howard Brown Memorial Clinic-Northwestern University Medical School, Chicago, IL
Reprint requests to Dr. Donald R. Hoover, Department of Epidemiology, Hampton House Room 784, 624 North Broadway, Baltimore, MD 21205.
943
944
Hoover et al.
peting risk formulations (1-3) can simultaneously
model transition into different disease and death states.
However, they require strong assumptions of independence (including Markovian transitions) that will be
impossible to validate from the data (4). They also
need software that is not available to medical researchers and may not be computationally feasible.
This paper defines relevant estimates of disease
incidence and prevalence for a population at high risk
of death from other causes. A four-stage transition
model illustrates these quantities and is a starting point
for developing estimates. An application is made to
evaluating cytomegalovirus disease occurrence and
morbidity in HTV-1-infected men.
the disease) at time t; /JDIS+,AIJVE> m e probability of
being in stage C (alive having developed the disease)
at time t; and ^*DIS+,DEAI» m e probability of being in
stage D (dead after developing the disease) at time t.
The sum of stages C and D gives P^iS+, the probability
of having developed the disease at or before time t.
The sum of stages B and D gives /'DEAD, the probability of having died at or before time t. The ratio at
time t of (stage C/(stage C + stage A)) gives
me
^DIS+IALIVE>
probability of having disease for a
person living at time t.
Each of the previously described quantities can be
estimated by reducing the four-stage process to an
appropriate two-stage subprocess and applying currently available Kaplan-Meier or binomial software.
MATERIALS AND METHODS
The disease and death model
Disease and death transition is a simple four-stage
process shown in figure 1. All subjects start in stage A
(living without the disease). With time, they move to
either stage B (dead without ever developing the disease) or stage C (living, having developed the disease).
From stage C they move to stage D (dead after developing the disease).
Longitudinal quantities of interest
The longitudinal quantities of interest with respect
to time, t, can be summarized in terms of the probabilities of being in each of four stages in figure 1:
e
^DIS".ALJVE> th probability of being in stage A (alive
without disease) at time t, /'DIS-.DEAD- m e probability
of being in stage B (dead without having developed
A
Kaplan-Meier estimation of P$ 8 + from a
two-stage submodel
For example, to estimate P&\s*' the nondiseased
stages (A and B) could be merged together into one
stage and the two diseased stages (C and D) together
into another (figure 2). The transition from the merged
nondiseased stage to the merged diseased stage could
then be estimated with a Kaplan-Meier approach.
For each study subject, i, let t2J be the time from the
study entry until the end of the study (or when the data
are analyzed), and let tltt be the time from study entry
until onset of disease. If the person never develops the
disease (i.e., dies first), then mathematically f,, could
be considered to equal infinity. Furthermore, t2J is
defined whether or not the subject was observed to die
during the study period. Let r, be the minimum of (r,,
and r 2 ,), and let cr, = (1 if disease was observed before
B.
Dead, never
diagnosed with
cytomegalovirus
disease
C.
Alive, diagnosed
with
cytomegalovirus
disease
Alive, without
cytomegalovirus
disease
D.
Dead, following a
cytomegalovirus
disease diagnosis
FIGURE 1. Transition stages to cytomegalovirus disease and death.
Am J Epidemiol
Vol. 143, No. 9, 1996
Projecting Disease When Death Is Likely
NONDISEASEO STAGE
DISEASED STAGE
Dead following
Disease
Dead without
Disease
Alive without
Disease
945
Alive with
Disease
FIGURE 2. The four-stage disease and death process subsumed into a two-stage nondiseased, diseased process.
the end of study, i.e., tXi < t2i and 0 otherwise). This
is analogous to 0 = censored and 1 = not censored. If
no dropout (loss to follow-up) occurs before the end of
study date, the standard Kaplan-Meier estimate applied to these (f,,o\) pairs obtains an appropriate estimate P$1S+ for P$IS+.
To demonstrate this, consider the following simple
example of two groups taken from two cities, each
with 100 HTV-1-infected men with follow-up beginning January 1, 1990. Assume that, for all men, complete data from registries are available on the onset of
cytomegalovirus disease through December 31, 1991
(i.e., t2i = 2 years). In each city, 15 men developed
cytomegalovirus disease during 1990 (a total of 30
men), and 15 men did so in 1991 (a total of 30 men).
Clearly, 15 percent (30 men) of the original 200 men
developed the disease in the first year after study
entry, 1990, and 15 percent (30 men) did so in the
second year, 1991. This can also be derived from a
Kaplan-Meier estimator, as is shown below in an
equivalent life table format subdivided into the 0- to
1-year interval and into the 1- to 2-year interval. The
men from each city are segregated in the numerators
and denominators, as the two cities will be treated
differently in subsequent modifications to the
example:
1
1
[100 - 15] + [100 - 15] _
[ioo]
n pg
U O J
do not develop disease in year 1;
n R«; vX
02. 0.85
_
_
[100
15] + [ ] 0 0
Vol. 143, No. 9, 1996
0
n SS V [(100 - 15) - 15] + [(100 - 15) - 85] _
/. u.&o x
[100
_ 15] + [(100 _ 15) _ g5]
n
7 n
- u. /u
do not develop disease in the first 2 years.
Provided no dropout occurs before the end of the
study, basing t21 on the planned (designed) follow-up
time unbiasedly reflects the time for observing the
event. Intuitively, it might seem as if this KaplanMeier estimator could be improved by incorporation
of knowledge of death without disease. However, to
extend t2i from knowledge of death without disease
(i.e., tu = °°) would make t2,- dependent on tu (i.e.,
longer when tx ( = °°) and bias the ensuing KaplanMeier estimate. For example, suppose that, in the city
censored at 1 year, 70 of the 85 men who had not
developed cytomegalovirus disease in the first year
had already died during that first year. One would be
tempted to let t2i = °° for those 70 men who will never
develop disease, leaving only 15 men from that city
censored at 1 year. The results would be to overestimate that
is] _
[(100 - 15) - 15] + [(100 - 15) - 15]
- 0.70
]5]
do not develop disease in the first 2 years.
The only removal from the denominator in modification 2 was the 30 men (15 from each city) who had
developed cytomegalovirus disease in the first year.
However, the Kaplan-Meier estimator remains accurate when censoring times vary. To see this, assume
that registry information in one city exists only from
January 1 to December 31, 1990. Then, t2i is 1 year
for the 100 men from that city and 2 years for the 100
men from the other city. We observe the 15 cytomegAm J Epidemiol
alovirus disease cases from the first year in the former
city, but we have no follow-up in that city for the
second year. The earlier censoring of 85 men who did
not develop cytomegalovirus disease in the first year
from one of the identical cities (reflected by their
removal from the numerator and denominator of modification 2) does not change the Kaplan-Meier estimate.
0.85 X
= 0.768
[100 - 15] + [(100 - 15) - 15]
do not develop disease in the first 2 years. There are no
other means to incorporate knowledge of death without disease into the Kaplan-Meier estimator without
biasing the results.
However, it should be noted that, if individuals in
stage A can be lost to follow-up before the end of the
study, then the t2i we propose will not reflect their
actual censor time. In addition, a t2i cannot be derived
for men remaining in the combined nondiseased stage
946
Hoover et aJ.
without creating a biased relation between t2i and
which will invalidate this Kaplan-Meier estimate.
Kaplan-Meier estimation for P$S,DEAD>
'>!?IS+.DEAD. and
g ^
PJ5IS-,DEAD- Death without disease is stage B. For a
subject who enters stage B, tt is ti it the time stage B
was entered, and cr, = 1. For a subject whose last stage
during the study was stage A, C, or D, tt is t2l, the time
from study entry until the end of the study, and cr, =
0. (However, for this t2i to be valid, persons in stages
A and C must not drop out before the end of study.)
The estimate PDI S -,DEAD obtains by subtracting from 1
the Kaplan-Meier survival estimate on these (f,-, cr,)
pairs.
^IS+.DEAD- Death following disease is stage D. For
subjects entering stage D, /,- is t,,, the time stage D was
entered, and cr,- = 1. For other subjects, f, is t2i, the
time from study entry until the end of the study, and cr,
= 0. (However, for this t2, to be valid, individuals in
stages A and C must not drop out before the end of
study.) Subtracting from 1 the Kaplan-Meier survival
estimate on these (tit cr,) gives ^DI S + ,DEADP$EAD- Death is stages B and D. For those who
enter these stages, r, is t{ „ the time of death, and <r, —
1. If follow-up is complete to the end of the study, then
tf = t2 „ the time from study entry until the end of the
study, and <r, = 0 for those whose last stage was stage
A or stage C. Subtracting from 1, the Kaplan-Meier
survival estimate on these (tt, cr,) pairs obtains /DEADIf loss to follow-up occurs before the end of the study
and is equally likely in stages A and C, then t2i should
be the last date the subject was observed.
Binomial estimation of P{?IS+IAIJVE a
n d
' J S > IS + ^UVE
The probability for a person living at time t to have
disease, /'DIS+IALTVE' is the ratio [stage C/(stage A +
stage C)]. Let n(t) be the number of subjects who are
living and under follow-up at time t, and let d(t) be the
number of these subjects who developed the disease at
or prior to time t. Then, assuming that diseased and
nondiseased persons have the same rate of loss to
follow-up, ^DIS+IALIVE = d{t)ln(t). If 100 people are
in the study alive at t = 1 year and if 50 of these
people have already developed the disease, then
0.50 = 50/100 estimates the proportion of people alive
at 1 year who have the disease. The variance of this
estimate is the well-known variance of a binomial.
By Bayes' theorem, /"DIS+^ALIVE ' S estimated by a
product of two previously described estimates:
DIS+.AUVE
\ AM
r
DEAD/
DIS+IALJVE-
(1)
For a fixed time t, the estimates
/*DIS+IALIVE are independent, ^DEAD is determined
only by the number and timing of deaths and censorings at and prior to t. ^DI S + IALIVE is based only on
subjects not dead or censored at or prior to /. Because
of the independence of individuals, the health status of
a person alive and under follow-up at time t is independent of the number of deaths and censorings
prior to t. Since the two estimators on the right-hand
side of formula 1 are independent, by Greenwood's (5)
formula:
vSr(Pg> s+iALIVE ) = (1 -
var
S+IALTVE)
DIS+
v a r
('DEAD) •
If the disease is not curable, then the expected amount
of disease morbidity time is the integral of the proportion diseased and alive:
[Expected time with disease morbidity]
• (2)
A commonly misused estimator of disease
incidence
A Kaplan-Meier estimate for the cumulative incidence of disease that censors disease-free individuals
at death is often used. We denote this estimate as
/>DIS CN DTH . For example, let 40 men be studied 2
years for the occurrence of cytomegalovirus disease.
Suppose that 30 men die without the disease in the first
year and that 10 others develop the disease during the
second year. Then, ^rs!.CNjOTH w i l 1 b e 1 0 - T ^ 3 0
first year deaths are censored, so only 10 men remained "under follow-up" in the second year, all of
whom developed disease. In contrast to this estimate,
only 0.25 (10/40) of the original cohort actually developed the disease. In the Discussion, we describe
how PDJ S CN D T H has been interpreted in the literature
and why these interpretations may be misleading, and
we show how the estimates derived here may be more
appropriate.
RESULTS
Monitoring HTV-1-infected persons with CD4 + cell
counts below 100/pil for cytomegalovirus disease is
now recommended (6, 7). Issues exist about cost effectiveness of prophylactic and therapeutic regimens
against this disease (8-11). Interactions of these medications with other anti-acquired immune deficiency
syndrome (AIDS) drugs and cumulative toxicities are
also of concern. Estimates on the timing of death and
Am J Epidemiol Vol. 143, No. 9, 1996
Projecting Disease When Death Is Likely
cytomegalovirus disease may help to answer questions
about the cost effectiveness of monitoring, treating,
and preventing this disease.
We evaluated 351 HTV-1-seropositive gay men
from the Multicenter AIDS Cohort Study (MACS)
(12) who used zidovudine and Pneumocystis carinii
prophylaxis and had CD4 + cell counts fall below
100//xl. Dates of cytomegalovirus disease and death
were determined with active and passive surveillance.
Participants had CD4 + cell counts measured every 6
months. Acquisition of these events is essentially complete even among men who quit study participation
(13). However, the men rarely discontinued study participation once immunosuppression became this poor
(i.e., CD4 counts below 100/p,l). Other analyses from
this cohort also censor (window) subjects at the date of
analysis (14, 15). Follow-up here begins at the date the
CD4 + count was first measured below 100//xl
(CD4100) and ends on December 31, 1993.
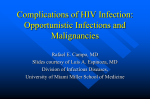
Figure 3 gives the probabilities over time to be in
each cytomegalovirus disease and death stage shown
in figure 1. At time t = 0, all participants start in the
middle unshaded region of figure 3, alive without
cytomegalovirus disease (stage A in figure 1). From
here, men can move to stage B, dead without diagnosis
of cytomegalovirus disease. This is the upper shaded
region of figure 3. Its lower boundary line is 1 M3IS-.DEAD- Transition into stage C, alive after the
diagnosis of cytomegalovirus disease, can also occur
from stage A. Stage C is the second to lowest shaded
947
region of figure 3. Its upper boundary line is
and its lower boundary is P^IS+ DEAD- From stage C,
participants move to stage D, dead after cytomegalovirus disease, the lowest shaded region of figure 3. Its
upper boundary line is ^DIS+,DEADTable 1 summarizes the regions in figure 3 at various times. At 1 year, 2 years, and 3 years, respectively,
after CD4 100 , only 68.4 percent, 31.0 percent, and 18.7
percent, respectively, remained alive without cytomegalovirus disease. By these times, 13.0 percent,
30.4 percent, and 35.2 percent, respectively, had developed cytomegalovirus disease. By 1,2, and 3 years,
respectively, after CD4 100 , 18.6 percent, 38.6 percent,
and 46.3 percent, respectively, had died without developing cytomegalovirus disease, while 4.5 percent,
15.8 percent, and 29.9 percent, respectively, had died
after developing this disease.
Also shown in figure 3 is a dashed line giving
CN DTH' m e Kaplan-Meier estimator of cytomegalovirus disease "cumulative incidence" which censors
disease-free individuals who die at their date of death.
These "cumulative incidences" are 14.1 percent for 1
year, 42.3 percent for 2 years, and 53.5 percent for 3
years. As we describe later, while this type of estimate
is often used, we believe it does not have a valid
interpretation.
Figure 4a gives the fractions of the original cohort
who were living with cytomegalovirus disease at given
times, PDIS+,ALIVE' a n ^ m e fractions initially diag-
6
CD
d
e
a.
q
d
Time after CD4 Counts First Fall below 100/pi
FIGURE 3. Longitudinal estimates of transition to cytomegalovirus disease and death. D, stage A (alive without cytomegalovirus disease);
B, stage B (dead having never been diagnosed with cytomegalovirus disease); B, stage C (alive and diagnosed with cytomegalovirus
disease); • , stage D (dead after diagnosis of cytomegalovirus disease);
, Kaplan-Meier "cumulative incidence" of cytomegalovirus
disease obtained by censoring at death.
Am J Epidemiol
Vol. 143, No. 9, 1996
948
Hoover et al.
TABLE 1. Longitudinal estimates of transition to cytomegalovirus disease and death stage with confidence intervals among men
receiving zidovudlne and Pneumocystis prophylaxis in the Mutticenter AIDS* Cohort Study, 1989-1993
Time after CD4+ cell counts first fall betow 100//J
2 years
1 year
Stage
Estimate
95% Cl'
Estimate
A (alive without
diagnosed
cytomegalovirus
disease)
68.4
62.6-73.4
31.0
B (dead without
diagnosed
cytomegalovirus
disease)
18.6
14.8-24.0
38.6
C and D (diagnosed with
cytomegalovirus
disease)
13.0
9.6-17.3
30.4
D (dead after diagnosis
of cytomegalovirus
disease)
4^5
2.3-7.2
1^8
• AIDS, acquired immune deficiency syndrome; Cl, confidence interval.
nosed with cytomegalovirus disease within 6 months
after that timepoint, [£<££ months) - Pg^HAt t = 0.5, 1.0, 1.5, 2.0, 2.5, and 3.0 years, respectively, after CD4 100 , 5.2 percent, 8.5 percent, 12.6
percent, 14.6 percent, 12.0 percent, and 5.6 percent,
respectively, of the initial subjects were living with
cytomegalovirus disease. Based on these numbers and
the trapezoidal rule for integrating formula (2), every
100 persons whose CD4 + counts fell below 100/jxl
generated 27.85 person-years, 100 \}h (0.052 + 0.085
+ 0.126 + 0.146 + 0.120) + V* (0.0 + 0.056)], of
cytomegalovirus disease during the next 3 years.
Figure 4b shows the fraction of the initial cohort
who have an initial manifestation of cytomegalovirus
disease during each 6-month interval. Between
0-0.50, 0.51-1.00, 1.01-1.50, 1.51-2.00, and 2.012.50 years, respectively, after CD4 100 , 5.3 percent, 7.5
percent, 9.8 percent, 7.1 percent, and 4.3 percent,
respectively, of the original cohort developed cytomegalovirus disease.
Figure 5a gives prevalences of cytomegalovirus disease among the men alive at t, ^DIS+IAIJVE (i-e> m e
ratio of stage C in figure 1 to the sums of stages A and
C). Among those men alive at 0.5, 1.0, 1.5, 2.0, 2.5,
and 3.0 years, respectively, after CD4 100 , 5.6 percent,
11.0 percent, 20.7 percent, 32.1 percent, 37.7 percent,
and 23.8 percent, respectively, also had cytomegalovirus disease.
Figure 5b gives the 6-month future incidences of
cytomegalovirus disease among men alive and disease
free at 0,0.5, 1.0, 1.5, and 2.0 years. The denominators
of these incidences are not the entire cohort but, rather,
the portions of the cohort in stage A at the beginning
of the interval. From 0-0.50, 0.51-1.00, and 1.01-
3 years
95% Q
Estimate
95% a
25.3-37.5
18.7
13.0-25.0
32.7-45.1
46.3
38.9-52.5
25.0-36.7
35.2
29.2^12.1
11.6-21.3
2O9
23.6-37.4
1.50 years, respectively, after CD4100, the 6-month
incidence of cytomegalovirus disease among surviving
subjects disease free rose from 5.3 percent to 8.5
percent and then to 14.2 percent. This 6-month incidence remained stable at 15.0 percent and 14.6 percent, respectively, from 1.51-2.00 and 2.01-2.50
years, respectively, after CD4 100 .
DISCUSSION
Potential uses of these estimates
Different questions call for different answers. The
standard analysis of time to event that censors at death
may not be answering a question that is relevant to a
given concern. We now discuss several relevant questions about disease incidence and prevalence in a
population at risk for death from other causes that one
might answer and indicate the appropriate estimates to
answer each.
The future timing for initial manifestations of disease is needed to plan screening programs or entry into
treatment studies. This information is provided by
examining the transition out of stage A into stage C, as
shown in figure 4b. For example, about 10 percent of
HTV-1-infected homosexual men reaching CD4 100 today will need to begin treatment for an initial cytomegalovirus condition between 1.0 and 1.5 years from
now.
Long-term future costs for the care of disease are
reflected by /*DIS+,ALIVE' th e "percentages of the original cohort in stage C, living with disease" at various
times, as shown in figure 4a. Of particular economic
interest is that, for every 100 HTV-1-infected homosexual men with CD4 + cell counts falling below
Am J Epidemiol
Vol. 143, No. 9, 1996
Projecting Disease When Death Is Ukely
949
a)
1
6
T
T
i I •
i
',
(
• " •
0.5 years
1.0 years
1.5 years
'
-
\
\
\
\
• • ' • ' —
Z 0 years
2.5 years
3.0 years
Time Points after CD4 Counts First Fall below 100//*/
n
1,
KM pWMia P
0-0.50 years
i
1
0.51-1.00 years 1.01-1.50 years 1.51-Z00 years 2.01 -2.50 years
Tbne Intervals after CD4 Counts Rrst Fan below 100//W
RQURE 4. a, fractions of the original cohort that are both alive and afflicted with cytomegaiovirus disease at selected time points (with 95%
confidence intervals); b, fractions of the original cohort that are initially diagnosed with cytomegaiovirus disease during selected 6-month
intervals (with 95% confidence Intervals), among human immunodeficiency virus type 1-infected users of zidovudine and Pneumocystis
prophylaxis in the Multicenter AIDS Cohort Study, 1989-1993.
100/fil today, 27.85 person-years of life with cytomegaiovirus disease morbidity can be expected over the
next 3 years.
Projecting short-term needs for counseling and treating
surviving immunosuppressed patients with initial manifestations of disease is important This is guided by the
incidences of disease among the living in figure 5b. If a
person continues to survive disease free more than 1 year
beyond the CD4 100 threshold, his chances of developing
cytomegaiovirus disease during the next 6 months remain between 14 and 15 percent.
Prophylaxis against diseases can be both expensive
and toxic (11). The effectiveness of a prophylaxis
must thus be based on whether it delays disease (stage
A), and if it 1) delays (or accelerates) the date of death
(stages B and D of figure 1); 2) delays the earliest of
the dates of disease and death (stages B and C of figure
1); and 3) delays the date of death attributable to the
disease (a subset of stage D in figure 1). The analyses
Am J Epidemiol
Vol. 143, No. 9, 1996
here provide normative data on the rates of these
events in subjects not receiving prophylaxis.
A prophylaxis trial starting at CD4 100 and lasting 1
year, aimed solely at detecting a protective effect
against death due to cytomegaiovirus disease, should
consider that 13.0 percent of subjects not receiving the
experimental agent would be expected to develop the
disease and that an additional 18.6 percent of subjects
die in that year. However, only 4.1 percent die in the
first year after previously developing cytomegaiovirus
disease. Thus, unless the sample size was huge, that
study would have almost no power to detect a prophylaxis effect on death from cytomegaiovirus disease.
Comparisons with a commonly misused
estimator of disease incidence
Many articles that analyze disease onset in settings
where death from other causes is likely fit Kaplan-
950
Hoover et al.
ID
d
(a)
in
d
cy
d
p
d
T
r.r .:•?::
0.5 years
1.0 years
1.5 years
2.0 years
2.5 years
3.0 years
Time Points after CD4 Counts First Fan below 100//W
d
in
6
IN
d
p
d
0-0.50 years
0.51-1.00 years 1.01-1.50 years 1.51-2.00 years 2.01-2.50 years
Time Intervals after CD4 Counts First FaD below 100//W
FIGURE 5. a, prevalences of cytomegalovirus disease among those still living at selected time points (with 95% confidence Intervals); b,
6-month incidences of cytomegalovirus disease among those still living and disease free at the beginning of the interval (with 95% confidence
intervals), among human immunodeficiency virus type 1 -infected users of zidovudine and Pneumocystis prophylaxis In the Multicenter AIDS
Cohort Study, 1989-1993.
Meier estimates (or actuarial, Poisson, and Cox model
analogs) that censor disease-free people at death (1624). This estimator is / ^ i s CN DTH> described in Materials and Methods. It has no direct medical or biologic meaning, but it has been misinterpreted in ways
that overestimate the occurrence of disease.
For example, ^DIS_CN_DTH *S °ft en reported to be
the cumulative probability of disease for the entire
cohort (16-21). However, PnisjCN_rrm from m e a n a l "
ysis here (figure 3, dashed line) was 53.5 percent. This
was almost 20 percent greater than PDI'F*™^ 3 5 - 2
percent, the correct estimate for the fraction of the
original cohort who had developed cytomegalovirus
disease by 3.0 years (from table 1).
Censoring disease-free people as "lost to follow-up"
at death mathematically assumes that these dead peo-
pie (in stage B of figure 1) continue to develop disease
(i.e., move into stage C) at the same rate as do the
living people in stage A. Dead people (in stage B) can
never develop disease (move into stage C or stage D),
whereas those alive but lost to follow-up can develop
disease. Thus, censoring disease-free people at death
overestimates the cumulative probability of disease for
the entire cohort.
If the processes leading to disease and death without
disease were independent, then / o i s CN DTH would
estimate the proportion who would develop disease by
time t if death from other causes could be eliminated.
It is, however, generally impossible to determine from
a given set of data whether two competing processes
are independent (4). Furthermore, independence of
these processes is medically unlikely. For example, in
Am J Epidemiol
Vol. 143, No. 9, 1996
Projecting Disease When Death Is Likely
general, sicker individuals may be both more likely to
develop the disease and to die of other causes (positive
dependence).
Estimates from Kaplan-Meier models that censor at
death (i.e., P^IS C N D T H ) are also often reported as
survivor prevalences" the probabilities of those living
at a given time, t, to have the disease (22-24). Again,
^DIS'CN ) DTH from the Kaplan-Meier model that censored at death in the example was 53.5 percent, more
than double PDIS^ALIVE . 23.8 percent, the observed
prevalence of disease among survivors 3.0 years after
CD4 100 (figure 5a).
The Kaplan-Meier estimate of the time to disease
that censors disease-free individuals at death increments the estimator as transitions from stage A to
stage C of figure 1 occur. However, it does not consider transitions to death from stages A and C. Usually
the disease is lethal; diseased cases in stage C die more
rapidly than those without disease in stage A. The
censor disease-free-at-death approach fails to account
for this shorter survival in those with disease and thus
overestimates disease prevalence among survivors.
Limitations and implications
We have given simple and important quantifications
of disease occurrence and morbidity in settings where
death from other causes is likely. We have presented
an approach that uses available statistical software to
estimate these quantities. One data requirement is that
participants not drop out before the end of the study. In
the example used for illustration here, that was the
case. We believe that this is also likely to be true in
general, as people at high risk for death are often
nonmobile and under intense observation.
Further research toward implementing these concepts with other parametric and nonparametric models
may be productive. For example, nonparametric formulations exist to simultaneously estimate the transition from one baseline stage to two (or more) adjacent
alternate stages (i.e., multiple decrements) (3). Unlike
the Kaplan-Meier model, software to implement these
models is not available nor have computationally feasible variances been demonstrated. However, multiple
decrement estimation could be incorporated into the
paradigm presented here and would eliminate the need
for an assumption of no dropout before the end of the
study.
Medical researchers have erroneously censored disease-free people at death, consequently overestimating
the magnitude of the disease. The concepts developed
here and the ability to produce estimates with accessible software may reduce this misapplication and
expand the information retrievable on disease occurrence and morbidity.
Am J Epidemiol
Vol. 143, No. 9, 1996
951
ACKNOWLEDGMENTS
This work was supported by NIH/NIAID cooperative
agreement UO1-AI-35043.
The authors acknowledge Dr. Lewis Schrager and Dr.
Harout Armenian, as well as Edith Muth for preparation of
the manuscript.
The Multicenter AIDS Cohort Study (MACS) includes
the following: Data Coordinating Center. The Johns Hopkins School of Hygiene and Public Health: A. Miifioz, C.
Enger, L. Epstein, S. Gange, D. Hoover, L. Jacobson, Y.
Peng, S. Piantadosi, and S. Su. Baltimore: The Johns Hopkins University School of Hygiene and Public Health: A.
Saah, H. Armenian, H. Farzadegan, N. Graham, N. Kass, C.
Lyketsos, J. Margolick, J. McArthur, and E. Taylor. Chicago: Howard Brown Memorial Clinic-Northwestern University Medical School: J. Phair, J. Chmiel, B. Cohen, M.
O'Gorman, D. Variakojis, J. Wesch, and S. Wolinsky. Los
Angeles: University of California, UCLA Schools of Public
Health and Medicine: R. Detels, B. Visscher, I. Chen, J.
Dudley, J. Fahey, J. Giorgi, M. Lee, O. Martinez-Maza, E.
Miller, H. Morgenstern, P. Nishanian, J. Taylor, and J.
Zack. Pittsburgh: University of Pittsburgh Graduate School
of Public Health: C. Rinaldo, Jr., R. Anderson, J. Becker, R.
Day, P. Gupta, M. Ho, L. Kingsley, J. Mellors, O. Ndimbe,
T. Silvestre, and S. Zucconi. NIH: National Institute of
Allergy and Infectious Diseases: L. Schrager; National Cancer Institute: D. Seminara.
REFERENCES
1. Chiang CL. Introduction to stochastic processes. New York:
John Wiley & Sons, Inc, 1968.
2. Hoel DG. A representation of mortality data by competing
risks. Biometrics 1972;28:475-88.
3. Aalen O. Nonparametric estimation of partial transition probabilities in multiple decrement models. Ann Stat 1978;6:
534-45.
4. Tsiatis AA. A nonidentifiability aspect of the problem of
competing risks. Proc Natl Acad Sri U S A 1975;72:20-2.
5. Greenwood M. The natural duration of cancer. In: Reports on
public health and medical subjects. Vol 33. London: Her
Majesty's Stationery Office, 1925:1-26.
6. Pertel D, Hirschtik R, Phair J, et al. Risk of developing
cytomegalovirus retinitis in persons infected with human
immunodeficiency virus. J Acquir Immune Defic Syndr 1992;
5:1069-74.
7. Luckie A, Ai E. Diagnosis and management of cytomegalovirus retinitis in AIDS. Curr Opin Ophthalmol 1993;4:81-9.
8. Palestine AG, Polis MA, De Smet MD, et al. A randomized,
controlled trial of foscamet in the treatment of cytomegalovirus retinitis in patients with AIDS. Ann Intern Med 1991;
115:665-73.
9. Holland GN, Buhles WC Jr, Mastre B, et al. A controlled
retrospective study of ganciclovir treatment for cytomegalovirus retinopathy. Use of a standardized system for the assessment of disease outcome. UCLA CMV Retinopathy Study
Group. Arch Ophthalmol 1989; 107:1759-66.
10. Mortality in patients with the acquired immunodeficiency
syndrome treated with either foscamet or ganciclovir for
cytomegalovirus retinitis. Studies of Ocular Complications of
AIDS Research Group, in collaboration with the AIDS Clinical Trials Group. N Engl J Med 1992;326:213-20.
11. Gallant JE, Moore RO, Chaisson RE. Prophylaxis for oppor-
952
12.
13.
14.
15.
16.
17.
Hoover et al.
tunistic infections in patients with HTV infection. Ann Intern
Med 1994;120:931-44.
Kaslow RA, Ostrow DG, Detels R, et al. The Multicenter
AIDS Cohort Study: rationale, organization, and selected
characteristics of the participants. Am J Epidemiol 1987;126:
310-18.
Hoover DR, Mufioz A, Carey V, et al. Using events from
dropouts in nonparametric survival function estimation with
application to incubation of AIDS. J Am Stat Assoc 1993;88:
37-43.
Stein DS, Graham NM, Park LP, et al. The effect of the
interaction of acyclovir with zidovudine on progression to
AIDS and survival. Analysis of data in the Multicenter AIDS
Cohort Study. Ann Intern Med 1994;121:100-8.
Lyketsos CG, Hoover DR, Guccione M. Depression as predictor of medical outcomes in HTV infection. JAMA 1993;88:
37-43.
Gallant JE, Moore RD, Richman DD, et al. Incidence and
natural history of cytomegalovirus disease in patients with
advanced human immunodeficiency virus disease treated with
zidovudine. J Infect Dis 1992;166:1223-7.
Chin DP, Hopewell PC, Yojko DM, et al. Mycobacterium
avium complex in the respiratory or gastrointestinal tract and
the risk of M. avium complex bacteremia in patients with
18.
19.
20.
21.
22.
23.
24.
human immunodeficiency virus infection. J Infect Dis 1994;
169:289-95.
Eddy DM. Screening for cervical cancer. Ann Intern Med
1990;l 13:214-26.
Applebaum FR, Barrall J, Storb R, et al. Bone marrow transplantation for patients with myelodysplasia. Pretreatment variables and outcome. Ann Intern Med 1990;l 12:590-7.
Veronegi U, Luiui A, Del Vecchio M, et al. Radiotherapy after
breast-preserving surgery in women with localized cancer of
the breast N Engl J Med 1993;328:1587-91.
Ovencia A, Bailey K, Yawn B, et al. Effect of gender on
long-term outcome of angina pectoris and myocardial
infarction/sudden unexplained death. JAMA 1993;269:
2392-7.
Phillips AN, Elford J, Sabin C, et al. Immunodeficiency and
the risk of death in HIV infection. JAMA 1992;268:2662-6.
Nightingale SD, Byrd LT, Southern PM, et al. Incidence of
Mycobacterium avium-intracellulare complex bacteremia in
human immunodeficiency virus-positive patients. J Infect Dis
1992; 165:1082-5.
Leoung GS, Feigal DW, Montgomery AB, et al. Aerosolized
pentamidine for prophylaxis against Pneumocystis carinii
pneumonia. N Engl J Med 1990;323:769-75.
Am J Epidemiol
Vol. 143, No. 9, 1996