Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
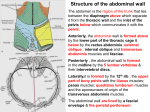
Visualização do documento Abdominal wall(1).doc (80 KB) Baixar 4  TOPOGRAPHIC ANATOMY OF THE ANTERIOR ABDOMINAL WALL, OF THE INGUINAL CANAL, OF THE FEMORAL CANAL. OPERATIONS IN HERNIAS.  The boundaries of the anterior abdominal wall are: superiorly – Âthe costal arches and xiphoid process, inferiorly – the iliac crests, inguinal folds (projection of the inguinal ligaments), pubic tuÂbercles and the superior margin of the symphysis pubis, laterally – the vertical line, which connects the end of the 11 rib with the iliac crests (Lesgaft's line). This line is the continuation of the midaxillary line, and it separates the abdominal region from the lumbar region. The surface landmarks are the following: xiphoid process, costal margin, iliac crest, pubic tubercle, symphysis pubis, inÂguinal ligament, superficial inguinal ring, linea alba, umbiliÂcus, rectus abdominis muscle. The anterior abdominal wall can be divided by horizontal and vertical planes (lines) into a number of regions which are of use to the clinician when describing the site of pain felt by a patient or of abnormal physical sings such as areas of tenderness or tumors. Two transverse and two vertical planes (lines) divide the anterior abdominal wall into three midÂline, three left, and three right regions. The vertical right and left lateral planes almost correspond to the midclavicular planes of the thorax and pass through the midpoint of a line joining the anterior superior iliac spine and the symphysis pubis (the midinÂguinal point). The subcostal plane joins the lowest point of the costal margin on each side, that is the tenth costal cartilage. The subÂcostal plane lies at the level of the third lumbar vertebra. The interspinal plane (linea bispinalis) joins the anterior superior iliac spine on each side. The midline regions are called the epiÂgastric, umbilical, and hypogastric regions. The lateral regions are called the hypochondriac, the lateral and inguinal (iliac) regions. Structures of the abdominal wall. Skin. The natural lines of cleavage in the skin are constant and run almost horizontally around the trunk. This is important cliÂnically, since an incision along a cleavage line will heal as a narrow scar, whereas one that crosses the lines will heal as a wide or heaped-up scar. The skin is supplied by the cutaneous branches of the seventh to twelfth intercostal nerves and by the first lumbar nerve in the form of the iliohypogastric nerve. A pleurisy involving the lower costal parietal pleura will cause pain in the overlying skin that may radiate down into the abdoÂmen. Although it is unlikely to cause rigidity of the abdominal muscles, it may cause confusion in making a diagnosis unless theÂse anatomical facts are remembered. Beneath the skin is located the subcutaneous tissue. The layer of adipose tissue is very vaÂriable thickness. Cutaneous arteries, which are branches of the superior and inferior epigastric arteries, supply the area near the midline, and branches from the intercostal, lumbar, and deep circumflex iliac arteries supply the flanks. . The venous blood is collected into a network of veins that radiates out from the umbilicus (thoracoepigastric, intercostal, and superficial epigastric veins). The network is drained above into the axillary vein via the lateral thoracic vein and below into the femoral vein via the superficial epigastric and great saphenous veins. A few small veins, the paraumbilical veins, conÂnect the network through the umbilicus and along the teres ligament to the portal vein. They form an important portal-systemic venous anastomosis. The superficial veins around the umbilicus and the paraumbiÂlical veins connecting them to the portal vein may become grossly distended in cases of portal vein obstruction. The distended subÂcutaneous veins radiate out from the umbilicus, producing the clinical picture referred to as caput Medusae. If there is obsÂtruction in the superior vena or inferior vena cava, the venous blood causes distention of the veins running from the anterior chest wall to the thigh. The superficial fascia is divided into a superficial and deÂep layer. The superficial layer of the superficial fascia is conÂtinuous with a superficial fascia of the thigh. The deep layer of the superficial fascia (Tomson's plate) or membranous layer is attached to the inguinal ligament and form similar layer in the perineum. It is important clinically, since beneath it the is a potential closed space that does not open into the thigh, but is continuous with the superficial perieneal pouch via the penis and scrotum. Rupture of the penile urethra may be followed by extraÂvasation of urine into the scrotum, perineum and penis and then up into the lower part of the anterior abdominal wall deep to the membranous layer of the superficial fascia. The urine is excluded from the thigh because of the attachment of the Tomson's plate to the inguinal ligament. In the anterior abdominal wall the proper or deep fascia is merely a thin layer covering the muscles. THE MUSCLES OF THE ANTERIOR ABDOMINAL WALL The musculature of the anterior and lateral walls of the abÂdomen is made up of a trilaminar sheet on either side of a pair of vertically oriented muscles. The thin aponeurotic tendons of the three lateral muscles form a sheath around each vertical muscle before fusing in the midline at the linea alba. The trilaÂminar sheet is composed of: 1.     The external oblique muscle. 2.     The internal oblique muscle. 3.     The transversus abdominis muscle. The vertically oriented muscles are the rectus abdominis muscles. In the lower part of the rectus sheath there may be preÂsent a small muscle called the pyramidalis. The cremaster muscle, which is derived from the lower fibers of the internal oblique, passes inferiorly as a covering of the spermatic cord and the scrotum. The external oblique muscle arises as digitations from the outer surfaces of the lower eight ribs. The fleshy fibers fan out downward and medially over the anterior abdominal wall. There is a free posterior margin to the muscle where its most posterior fibers run from the twelfth rib to the anterior half of the outer margin of the iliac crest. The remaining more obliquely running fibers become an aponeurotic sheet which contributes to the anteÂrior sheath of the rectus muscle before fusing with its fellow at the linea alba in the midline. The lower free margin of the aponeurosis extends from the anÂterior superior iliac spine to the pubic tubercle and is called the inguinal ligament. From the medial end of the ligament the lacunar ligament extends backward and upward to the pectineal liÂne on the superior ramus of the pubis. Its sharp, free crescentic edge forms the medial margin of the femoral ring. On reaching the pectineal line, the lacunar ligament becomes continuous with a thickening of the periosteum called the pectineal ligament. To the inferior rounded border of the inguinal ligament is attached the deep fascia of the thigh – the fascia lata. A triangular-shaped defect in the external oblique aponeuroÂsis lies immediately above and medial to the pubic tubercle. This is known as the superficial inguinal ring. The spermatic cord (or round ligament of the uterus) passes through this opening and carries the external spermatic fascia (or the external covering of the round ligament of the uterus) from the margins of the ring. The internal oblique muscle arise from the thoracolumbar fascia, the anterior two-thirds of the iliac crest deep to the attachment of the external oblique, and from the lateral two-thirds of the inguinal ligament. The fibers fan out from this origin. The uppermost run upward and medially to become attached to the costal margin. The intermediate fibers become aponeurotic and help in the formation of the rectus sheath before joining the linea alba. The lowermost are attached by a flattened tendon to the pectineal line on the superior pubic ramus. The fibers of transversus abdominis muscle arise from a long origin which extends from the deep surface of the costal margin, the thoracolumbar fascia, the anterior two-thirds of the medial margin of the iliac crest, and the outer half of the inguinal ligament. Running approximately transversely across the abdominal wall, the fibers also become aponeurotic and contribute to the rectus sheÂath before joining the linea alba. The muscular fibers form the linea semilunaris (Spigelii) in the passage to the aponeurosis. This line extends from the inguinal ligament to the sternum. THE RECTUS ABDOMINIS The two rectus abdominis muscles form the vertical component of the anterior abdominal musculature and lie on either side of the linea alba. The muscles are broad superiorly and narrow infeÂriorly. Each is attached to the fifth, sixth, and seventh costal cartilages above and below by tendinous and fleshy insertions to the pubic crest and the symphysis pubis. The anterior surface of the muscle is crossed by three tendinous intersections. One of these lies at the level of the umbilicus and two are above. These intersections are strongly attached to the anterior wall of the rectus sheath. The rectus abdominis is enclosed between the apoÂneuroses of the external oblique, the internal oblique, and the transversus, which form the rectus sheath. The piramidalis muscle is often absent. It arises by its baÂse from the anterior surface of the pubis and is inserted into the linea alba. It lies in front of the lower part of the rectus abdominis. THE RECTUS SHEATH Each rectus abdominis muscle is enclosed in a fibrous sheath formed by the aponeurotic tendons of the three lateral muscles. The external oblique contributes to the anterior layer the sheath over its whole extent. Below the costal margin the internal obliÂque aponeurosis splits around the muscle contributing to anterior and posterior layers and the aponeurosis of the transversus abdoÂminis passes into the posterior layer. Midway between the umbilicus and the symphysis pubis, the posterior wall of the sheath becomes deficient since all aponeuÂroses pass anterior to the rectus abdominis. At the level at which the aponeuroses of all three lateral muscles fuse to form only the anterior layer of the sheath, the posterior sheath terÂminates at a free margin called the arcuate line (Douglasi line). It is here that the inferior epigastric artery enters the sheath to run superiorly on the deep surface of the rectus abdominis muscle. The artery anastomoses with the superior epigastric arteÂry, which has entered the sheath from above by passing deep to the costal margin. Below the level of the arcuate line the rectus abdominis lies on the transverse fascia. The muscles of the anterior abdominal wall are supplied by the lower six thoracic and first lumbar segmental nerves. The thoracic nerves emerge beÂneath the costal margin and run downward and forward the abdomiÂnal wall between the internal oblique and transversus abdominis muscles. The nerves are accompanied by branches of the musculophrenic or the first lumbar artery. To thoracic (intercostal) nerves are added the iliohypogastric and ilioinguinal nerves which are deriÂved from the first lumbar nerve. These supply the lower fibers of the external oblique, internal oblique, and transversus abdominis muscles. In addition to branches of the musculophrenic and lumbar arteries, which supply the lateral muscles, the superior and inÂferior epigastric arteries supply the rectus abdominis muscle. THE RETROMUSCULAR LAYERS They include: the fascia transversalis, the extraperitoneal (preperitoneal) fat, the parietal peritoneum. The fascia transversalis is a thin layer of fascia that liÂnes the transversus abdominis muscle and is continuous with a siÂmilar layer lining the diaphragm and the iliacus muscle. It is important to understand that the fascia transversalis, the diaphÂragmatic fascia, the iliacus fascia, and the pelvic fascia form one continuous lining to the abdominal and pelvic cavities. The extraperitoneal fat is a thin layer of connective tissue that contains a variable amount of fat and lies between the fasÂcia transversalis and the parietal peritoneum. The walls of the abdomen are lined with parietal peritoneum. This is a thin serous membrane and is continuous below with the parietal peritoneum lining the pelvis. The parietal peritoneum lining the anterior abdominal wall is supplied segmentally by inÂtercostal and lumbar nerves, which also supply the overlying muscles and skin. The linea alba extends from the xiphoid process down to the symphysis pubis and is formed by the fusion of the lateral muscÂles of the two sides. Wider above the umbilicus, it narrows down below the umbilicus to be attached to the symphysis pubis. The linea alba has the through slitlike spaces. The vessels, nerves and fat (which connects the extraperitonial fat with subcutaneous fat) pass through this spaces. This slits can be by the places of outlet of the herniae. It is called the hernia of the linea alba or the epigastric hernia. The linea alba is a weak place of the anterior abdominal wall. The umbilicus is located in the middle of the line which connects the apex of the xiphoid process with the superior margin of the symphysis pubis. The umbilicus is drawn in scar which is formed in place of the umbilical ring. The umbilical ring is the foramen which is limited by the aponeurotic fibers of the linea alba. The urachus, umbilical vein, two umbilical arteries pass through the umbilical ring in the intrauterine development. Then this structures are turned into the ligaments. The urachus is turned into the median umbilical ligament. The umbilical vein is turned into the ligament teres of the liver. The umbilical arteÂ... Arquivo da conta: gblnetto Outros arquivos desta pasta: Head(1).doc (2891 KB) Abdominal cavity(1).doc (109 KB) Examinational questions(2).doc (82 KB) Amputations and exarticulations(1).doc (621 KB) Abdominal wall(1).doc (80 KB) Outros arquivos desta conta: Galeria Medicine Privada Relatar se os regulamentos foram violados Página inicial Contacta-nos Ajuda Opções Termos e condições PolÃtica de privacidade Reportar abuso Copyright © 2012 Minhateca.com.br