Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
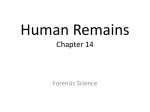
The Clivus Lesions: Crossroads Of Skull Base Poster No.: C-1617 Congress: ECR 2014 Type: Educational Exhibit Authors: E. S. Morales Deza, E. Santamarta, A. Saiz Ayala, E. Murias, P. Vega Valdes, J. L. LLorente Pendas; Oviedo/ES Keywords: Head and neck, Musculoskeletal bone, MR, CT, Imaging sequences, Education and training DOI: 10.1594/ecr2014/C-1617 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 53 Learning objectives The aim of this study is to show the radiological findings of the common and uncommon clival lesions including advanced MR sequences. Background The clivus is a "hidden" part of the base of the skull located between the foramen magnum and back of the sella and so far difficult to explore. Radiologists play a key role in the demonstration and description of the clivus pathology. There are many disease processes involving clivus, that are mixed due to their histological origin (bone, cartilage, notochord residues) and highly vascularized nature (metastasis). There are also "pseudo-lesions" or "incidentalomas" that we should to know and distinguish from the significant injuries. Endoscopic treatment techniques are becoming more common, which has increased the interest in this area. Anatomy: The clivus is a bony canal in the basilar of occipital bone, between the back of the sella and the foramen magnum. It is formed by the union of the posteroinferior part of the body of the sphenoid bone (basisphenoid) and the anterosuperior part of the occipital bone (basioccipital). The sphenoid synchondrosis is the junction between the sphenoid and occipital bones, which usually ends between 18-25 years. Anatomical relations: • • • • Anterior: Sphenoidal sinus. Posterior: Cisterns of the skull base. Inferior: Nasopharynx. Atlanto-occipital joint. Lateral: Petro-occipital fissures and condylar canals. The signal of cancellous bone depends on the degree of maturity of the bone marrow. The hematopoietic tissue, which predominates in young individuals, is usually hypointense on T1WI MR, but when fat metamorphosis occurs, it becomes more hyperintense. Most of lesions of the clivus are hypointense on T1WI and hyperintense on T2WI MR. The imaging techniques to study the skull base commonly include the MDCT and MRI, the last one with conventional (T1,T2, FST2, GRT2*, FLAIR, Dynamic GRE +C, T1 FS + Page 2 of 53 C), and special sequences (DWI, 3D FIESTA, etc). Each of them has its own contributions to the diagnosis. Images for this section: Fig. 1: Endoscopic treatment techniques are becoming more common, which has increased the interest in this area. Page 3 of 53 Fig. 2 Page 4 of 53 Fig. 3 Page 5 of 53 Fig. 4 Page 6 of 53 Fig. 5 Page 7 of 53 Fig. 6: Pneumatization begins at birth, grows backwards to invade the basisphenoid (BS) Page 8 of 53 Fig. 7: Bone marrow is composed predominantly of fat and water, Relative proportions of these, affect the signal intensity in MRI. Page 9 of 53 Fig. 8 Page 10 of 53 Fig. 9: CT identifies lytic or blastic lesions, and the presence of cartilage matrix or calcifications with great sensitivity. It is less sensitive to the infiltration of the bone marrow. Page 11 of 53 Fig. 10: The natural contrast of fat in adult bone marrow let to identify focal or infiltrative lesions with high sensitivity. Page 12 of 53 Fig. 11: Metastasis of Prostate: Small focal sclerotic lesion on CT and hypointense on T1WI, that increases its size in one year. Page 13 of 53 Fig. 12: Infiltrative tumor lesions alter the sign of the recognizable bone marrow in diffusion sequence (b 1000) as hyper intense areas. Page 14 of 53 Fig. 13: The detection of small "residual tumor" or "abscess" also benefits from the diffusion sequence. Page 15 of 53 Fig. 14: The presence of intramedullary enhancement in the clivus helps to detect metastatic lesions in doubtful cases. Page 16 of 53 Fig. 15: Presence of intra medullary enhancement helps to differentiate the bone edema (because of tumor proximity) from the true tumor infiltration. Page 17 of 53 Findings and procedure details This is a retrospective study of 62 patients with lesions involving the clivus between october 2006 and july 2013 in our database (HUCA). All patients were studied with a equipment of MRI 1.5 Tesla GE Signa MR LX and two multi-slice MDCT Toshiba scenners 16/64 channels. RESULTS: 1.-Primary Neoplasms: 11 Chordoma (8), chondrosarcoma (2), enchondroma (1) 2.-Secondary tumors: 34 Metastasis (16), nasopharyngeal carcinoma (7), rhabdomyosarcoma (1), juvenile angiofibroma (2), invasive pituitary adenoma (3) and meningiomas(5) 3.-Hematopoietic Disorders: 8 Myeloma (4), leukemias (2), histiocytosis (2) 4.-Pseudotumoral or dysplastic lesions: 11 Arachnoid granulations (2), intraosseous lipomas (3), fibrous dysplasia (2), Paget (1), simple cyst (1), meningocele (1), cholesterol cyst (1). 5.-Inflammatory and infectious lesions: 4 Osteomyelitis (1), mucopyocele (2), radiotherapy (1) 6.-Miscelanea: 3 Fístula (1), fracturas (2). Because his mixed histological origin (bone, chordomatous, cartilage, notochordal rest..) and his highly vascularised nature the are many pathological processes involving clivus which represent a diagnostic and a therapeutic challenge. MDCT appears to be a perfect diagnostic tool when bony involvement is present. So, TC is useful when cortical bone is affected or if obvious lytic or sclerotic bone lesions are present. Fibro-osseous and Page 18 of 53 calcified lesions are also well seen on MDCT. MRI appears to be more sensitive in detecting bone marrow involvement in the clivus and occipital bone. Isolated bone marrow metastasis or diffuse infiltrative processes of the skull base is best demonstrated on MRI. Sagittal and axial SE-T1 weighted and Dynamic GRE Gadolinium enhanced T1-weighted MR images are the most useful sequences. T2-weighted images are very sensitive for chordomas and chondrosarcomas. The apparent diffusion coefficient (ADC) value, determined from DWI, can help in cancer staging and detection small clivus metastasis or postoperative residual tumor. The ADC value also discriminates tumors from abscesses. Images for this section: Fig. 16 Page 19 of 53 Fig. 21: Rare malignant neoplasm (1% of intracranial T.), slow-growing, derived from remnants of the notochord. Affects the midline. 35% at the skull base: clivus: more frequent (spheno-occipital synchondrosis), sphenoid (30%) and petrous apex. Page 20 of 53 Fig. 18 Page 21 of 53 Fig. 17: a) Sag SE T1WI + C: large sphenoidal mass extending from the Sellar area to the rhino pharynx. b) Sag CT + C: erosion of the upper third of the clivus. c) Coronal T2-FSE: heterogeneous hyperintense mass in nasopharynx. d) Axial SE T1WI + C and FS : The lesion shows homogeneous enhancement and erosion of the lateral portion of the clivus. Page 22 of 53 Fig. 22: Slow growing chondroid neoplasm. They may occur in cartilage, endochondral bone or primitive mesenchymal cells of the brain, meninges or membranous bone of soft tissue. It may be secondary to bone diseases (fibrous dysplasia, Paget's disease, Ollier syndrome). Page 23 of 53 Fig. 19: Petroclival chondrosarcoma A) and B) Axial CT: typical chondroid calcifications. C)GR T2 * intratumoral calcifications. D)Axial SE T1 + C: parasellar lesion with little enhancement (heterogeneous) with clival involvement which extends to prepontine cistern. E) FSE T2 Fat Sat. F) DWI MR: Deformity of the lesion by magnetic susceptibility of the skull base and air interface. Page 24 of 53 Fig. 20: A) and B) Axial CT: petroclival lytic destructive lesion in the petro-occipital fissure. Small foci of calcifications with tumoral matrix are seen. C) Sag T1WI: clival mass with medial extension to prepontine cistern that compresses the brainstem. D) Diagram of skull base. E) and F) Axial and coronal SE T2 FS: hyperintense tumor with small hypointense foci. Page 25 of 53 Fig. 23: It particularly affects patients with breast carcinoma, lung, kidney and prostate. There are 5 syndromes according to metastasis location (orbitary, parasellar, middle cranial fossa, jugular foramen and condylar) Page 26 of 53 Fig. 24 Page 27 of 53 Fig. 25: Metastasis. In adults T1WI sequences are more sensitive than CT or T2. Diffusion sequences are helpful in selected cases, and dynamic sequences with contrast show in a better way the abnormal medullary enhancement. We report 2 cases with doubtful CT where DWI and dynamic study established the diagnosis. Page 28 of 53 Fig. 26: Highly invasive tumor, up to 30% with invasion of the skull base until initial diagnosis (because of paucity of symptoms). Page 29 of 53 Fig. 27: Bone invasion. A) and B) Axial SE without and with contrast: Infiltrative enhancing mass that originates from the nasopharynx, with bone destruction of the skull base, affecting the clivus, foramen ovale and foramen lace rum. C) Coronal SE FS + C: It infiltrates the left cavernous sinus and surrounds the ipsilateral carotid artery. D) Axial T2 FSE: shows an infiltrative pattern in the clivus and petrous apex. Page 30 of 53 Fig. 28: Sinus tumors are 2-3% of the head and neck tumors. Only 1-2% affect the sphenoid sinus. Histology: Squamous carcinoma (70-80%), only 6-17% are tumors from minor salivary glands, mucoepidermoid and undifferentiated carcinomas. A) Sagittal SET1: Expasive tumor (T) of the sphenoid sinus which extends to the nose and clivus. B) Coronal T2 FSE: sphenoid sinus expanded laterally and compression of the left cavernous sinus. Page 31 of 53 Fig. 29: 5% of pituitary adenomas can become "invasive" and simulate metastases or other aggressive tumors. A invasive adenoma, but benign, could not be distinguished from a pituitary carcinoma on imaging. Page 32 of 53 Fig. 30: A) and B) Axial CT: large expansive lytic lesion in the right sellar and parasellar region with typical benign bone margins. C) and D) Cor and Axial T1 + C: sellar mass that invades the skull base and extends through the right cavernous sinus and clivus. E) Sag T1 + C: cranially suprasellar extension surrounding the carotid. F) Diagram of the skull base. Page 33 of 53 Fig. 31: Benign tumors that arise from arachnoid cells of the meninges (15% of all primary brain tumors). Any sphenoid meningioma can extend extracranially through foramina of the skull base or by destruction and direct extension from the middle cranial fossa. Page 34 of 53 Fig. 32 Page 35 of 53 Fig. 33: MM represents >40% of primary malignant bone tumors. It is the most common primary malignant bone tumor. Page 36 of 53 Fig. 34: Plasmacytoma of skull base: A) Axial CT: diffuse destructive/lytic areas in the center of the base of the skull with sellar infiltration, basisphenoid and ethmoid. B) Diagram of the skull base. C) and D) Axial CT + C: Infiltrating soft tissue mass with moderate enhancement that affects the central skull base and both petrous apices. Multiple calcifications. Page 37 of 53 Fig. 35: Non-Hodgkin lymphoma (NHL) is a rare tumor of the skull base. Nasal and paranasal sinus NHL, with involvement of the skull base and intracranial affectation, represents advanced sinonasal primary disease. Page 38 of 53 Fig. 36: Diffuse infiltration of the bone marrow in hematological tumor processes is nonspecific and comparable to metastatic infiltration. Page 39 of 53 Fig. 37: Mucopyocele by Staphylocus hyicus (cocaine abuse): A), B) and C) Sag FSE T2 and T1 SE with and without contrast: expansive lesion in quadrilateral plate and clivus with cortical destruction. Occupation of the frontal sinus. Peripheral enhancement of the mucosa with central hypointensity in both lesions. D) and E) Axial DWI: signal hyperintensity with restrictrion on diffusion, indicative of abscesses. F) and G) axial and cor CT: bone destruction of clivus. Page 40 of 53 Fig. 38: Malignant otitis externa by Pseudomona aeruginosa in diabetic patient: A) and B) CT shows sclerosis in the right side of the clivus consistent with osteomyelitis by contiguity. C) and D) T1WI MR shows a large soft tissue inflammatory component of the masticator and parapharyngeal spaces with bone infiltration, compatible with edema and/ or osteomyelitis. Page 41 of 53 Fig. 39: Lesión pseudotumoral de morfología redonda, ovoidea y densidad similar a LCR en todas las secuencias estables en el tiempo, Normalmente son de pequeño tamaño, aunque existen forma pseusotumorales y en ocasiones se asocian a fístulas de LCR. A) sagital en T1, B) coronal en T2 y C) axial de TC con ventana ósea: lesión hipointensa en T1 e hiperintensa en T2, de bordes bien definidos y esclerosos. Page 42 of 53 Fig. 40: It is usually asymptomatic and incidentally discovered in CT or MRI. In TC can simulate a more aggressive lesion such as chroma. MRI fat suppression techniques allows diagnosis. A) CT axial, B) sagital T1WI, C) axial T1WI, D) FLAIR, E) T2WI, and F) Fat-suppressed T1: bone lesions with thin hypointense edges in the body of the sphenoid (secondary to reactive sclerosis), and hyperintense centre on T1 and T2WI wihch is suppressed on FS sequences. Page 43 of 53 Fig. 41: Cholesterol granuloma of the petrous apex: It is the most common lesion on the petrous apex, ad produces a characteristic expansive lytic lesion with cortical thinning, secondary to repeated bleeding. Petro-clival expansive lytic lesion. Sag SE T1WI shows the characteristic signal intensity due to the presence of chronic hematic elements and crystals of cholesterol (xanthochromic liquid). SE-T1 Fat Sat: to differentiate it from other lipomas. SE-T1 +C : no enhancement. DWI MR: heterogeneous hypointense signal (T2 dark through) by the presence of hemosiderin. Page 44 of 53 Fig. 42: Osteochondromas are uncommon in the region of the clivus. They can cause local mass effect and rarely compromise of the foramen magnum. Usually asymptomatic. A) 3D CT axial reconstrucción, B) and C) MPR CT coronal and sagital, D) and E) axial FLAIR and sagittal T1 SE MRI: hyperostotic bone reaction of the lower-left region of the clivus, and "pseudoarticulation" with the odontoid. Page 45 of 53 Fig. 43: Defects of neural tube closure during early embryonic development, with "herniation" of the dura through a bone defect, containing meninges and CSF. Signal equal to CSF on all MRI sequences (T1, T2, fat suppression). CT scan shows well-defined erosions of the clivus and petrous apex, with water density. Page 46 of 53 Fig. 44: Sagittal, axial and coronal CT with bone windowing: lytic and sclerotic multiple lesions distributed throughout the calotte and the skull base, which also affect the clivus. Page 47 of 53 Fig. 45: Also called Osteitis deformans: CT: varies according to the phase of the disease: Destructive osteoporotic/lytic or osteoclastic phase with forming bone. Simple RX and CT: Extensive bone involvement with thickening and "cotton wool" appearance in all the calotte and skull base. A) and B) CT in advanced stage: widening and thickening of the entire skull base and calotte, with "cotton wool" densities. Deformity and bone remodeling are characteristic. Page 48 of 53 Fig. 46: Axial and 3D reconstruction CT: expansive bone lesion with variable attenuation. Lesion with lucente centre, thin sclerotic margins, and "ground glass" density. Sphenoethmoidal involvement of the clivus and thickening due to fibrous dysplasia. Page 49 of 53 Fig. 47: CT (A, B, C and D), 3D CT (E): fracture lines, one horizontal across the upper third of the clivus (#) with avulsion of the sellar dorsum (#), sinus hemorrhage (* ) and pneumocephalus in a patient with severe TBI. Page 50 of 53 Fig. 48: A) and B) Sagittal T2 and T1WI MR: Pneumatization with fluid level in the sphenoid sinus (*). C) and D) axial and sagittal Mielo CT: bone dehiscence in the upper third of the clivus (basisphenoid) (#). E) Sagittal T2WI MR: hypointense postoperative material (tensor Fascia Latae) plugging the fistula (#). Page 51 of 53 Conclusion Combination of MDCT and MRI findings allow the correct diagnostic approach to the clivus pathology. Bone involvement is best demonstrated on MDCT with bone windowing, while MRI is more accurate in determining tumor margins, soft tissue involvement and diffuse intraosseous lesions. In our experience the most useful sequences were: T1 SE with and without Fat Sat, dynamic sequences with contrast, and difusion. Knowledge of tumor and tumor-like lesions of the petroclival area is important for a correct diagnosis. Personal information References 1. 2. 3. 4. 5. 6. 7. 8. 9. Gupta A, Harnsberger HR. Chordoma, clivus. In: Diagnostic Imaging: Head and Neck. Salt Lake City: Amirsys;2004 :I3-10 Chua R, Shapiro S. A mucopyocele of the clivus: case report. Neurosurgery 1996;39:589-90. Oruckaptan HH, Akdemir P, Ozgen T. Isolated sphenoid sinus abscess: clinical and radiological failure in preoperative diagnosis. Case report and review of the literature. Surg Neurol 2000;53:174-77. Nemeth AJ, Henson JW, Mullins ME, et al. Improved detection of skull metastasis with diffusion-weighted MR imaging. AJNR Am J Neuroradiol 2007;28:1088-92. Erdem E, Angtuaco EC, Van Hemert R, et al. Comprehensive review of intracranial chordoma. Radiographics 2003;23:995-1009. Hayashida Y, Hirai T, Yakushiji T, et al. Evaluation of diffusion-weighted imaging for the differential diagnosis of poorly contrast-enhanced and T2-prolonged bone masses: initial experience. J Magn Reson Imaging 2006;23:377-82 . Pui MH, Mitha A, Rae WI. Diffusion-weighted magnetic resonance imaging of spinal infection and malignancy. J Neuroimaging 2005;15:164-70 . Kainberger F. Diffusion weighted imaging of bone marrow pathologies. Eur J Radiol 2005;55:74-83. Wolfe JT III, Scheithauer BW. "Intradural chordoma" or "giant ecchordosis physaliphora"? Report of two cases. Clin Neuropath 1987;6:98-103 Page 52 of 53 10. Erdem E, Angtuaco E, Hemert R, et al. Comprehensive review of intracranial chordoma. Radiographics 2003;23:995-1009. 11. DiFrancesco LM, Castillo C, Temple WJ. Extra-axial chordoma. Arch Pathol Lab Med 2006;130:1871-74. 12. Masui K, Kawai S, Yonezawa T, et al. Intradural retroclival chordoma without bone involvement. Neurol Med Chir (Tokyo) 2006;46:552-55. 13. Madeline LA, Elster AD. Postnatal development of the central skull base: normal variants. Radiology 1995;196:757-63. 14. Hughes ML, Carty AT, White FE. Persistent hypophyseal (craniopharyngeal) canal. Br J Radiol 1999;72:204-06. 15. Marsot-Dupuch K, Smoker WR, Grauer W. A rare expression of neural crest disorders: an intrasphenoidal development of the anterior pituitary gland. AJNR Am J Neuroradiol 2004;25:285-88. 16. Barnes L. Pathology of selected tumors of the base of the skull. Skull Base Surg 1991;1:207-16. 17. Heffelfinger MJ, Dahlin DC, MacCarty CS, et al. Chordomas and cartilaginous tumors at the skull base. Cancer 1973;32:410-20. 18. King AD, Lei KI, Richards PS, et al. Non-Hodgkin's lymphoma of the nasopharynx: CT and MR imaging. Clin Radiol 2003;58:621-25. 19. Weber AL, al-Arayedh S, Rashid A. Nasopharynx: clinical, pathologic and radiologic assessment. Neuroimaging Clin N Am 2003;13:465-83. 20. Urquhart A, Berg R. Hodgkin's and non-Hodgkin's lymphoma of the head and neck. Laryngoscope 2001;111:1565-59. Page 53 of 53