Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
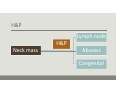
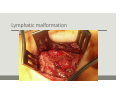
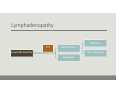
Pediatric Neck Masses A N D R EW R . S I M O N S E N , D.O. P E D I ATRI C OTO L A RYN GO LOGY JAC KS O N V I LL E, F L Pediatric neck masses Unlike adults most are benign 1 in 10 of all pediatric neck masses after excision are malignant. 29% of biopsied benign appearing neck masses are malignant. ◦ Torsiglieri AJ Jr, Tom LW, Ross AJ 3rd, et al. Pediatric neck masses: guidelines for evaluation. Int J Pediatr Otorhinolaryngol 1988;16(3):199–210 Objectives 1. Systematic approach ◦ Inflammatory, congenital, neoplastic 2. Appropriate and cost effective studies 3. Rule out malignancy 4. Diagnosis 5. Timely resolution H&P Lymph node H&P Neck mass Abscess Congenital History Age of onset Duration of signs and symptoms Pain Change in size ◦ Rate of change Involvement of other organ systems ◦ Recent H&N infections ◦ Fatigue, weight loss, fever, night sweats Environmental exposures ◦ Cats, nondomestic animals, insects, travel, humans with TB Prior treatment Physical Complete H&N exam ◦ Begin away from mass ◦ Scalp Full body exam ◦ Primary inoculation site ◦ Adenopathy ◦ Skin lesions ◦ Hemangiomas, café au lait spots ◦ Liver, spleen Physical Location of the mass ◦ May M. Neck masses in children: diagnosis and treatment. Pediatr Ann 5:8, 1976. Palpation of the mass ◦ ◦ ◦ ◦ Tender Cystic Lymph node Enlarges with straining Draining fistula Diagnostic studies Labs Radiologic FNA Prenatal Congenital TGDC Imaging Dermoid Congenital Branchial anomaly Vascular malformation Congenital ‐‐ midline Thyroglossal duct cyst ◦ May present after birth with infection ◦ Moves superiorly with swallowing or protrusion of the tongue ◦ Ultrasound of mass and thyroid ◦ Excision ‐ Sistrunk Dermoid ◦ ◦ ◦ ◦ ◦ Present at birth Moves independently with skin Doughy Epidermal and dermal components Neck is second most common site ◦ Pryor SG. Pediatric dermoid cysts of the head and neck. Otolaryngol Head Neck Surg 2005;132:938‐42 ◦ 18% on the neck ◦ No imaging was necessary ◦ Ultrasound ◦ Simple excision Congenital ‐‐ branchial Branchial cleft cysts ◦ First ◦ Work types I and II1 ◦ Second ◦ Third/fourth Studies ◦ CT/MRI Treatment ◦ Excision 1WORK W. NEWER CONCEPTS OF FIRST BRANCHIAL CLEFT DEFECTS. LARYNGOSCOPE 1972;82:1581‐93 First branchial arch ADAPTED FROM: BLUESTONE, SURGICAL ATLAS OF PEDIATRIC OTOLARYNGOLOGY 2002, DC DECKER Second branchial arch ADAPTED FROM: BLUESTONE, SURGICAL ATLAS OF PEDIATRIC OTOLARYNGOLOGY 2002, DC DECKER Figure 2 (A) Artist rendition of excision of second BA cyst with sinus tract extending into the pharynx above the carotid bifurcation. Schroeder J W et al. Otolaryngology -- Head and Neck Surgery 2007;137:289-295 Copyright © by American Academy of Otolaryngology- Head and Neck Surgery Second branchial arch cyst PHOTOS COURTESY OF AIYSHA BALBOSA, D.O. DRISCOLL CHILDREN'S HOSPITAL, CORPUS CHRISTI, TX Third branchial arch ADAPTED FROM: BLUESTONE, SURGICAL ATLAS OF PEDIATRIC OTOLARYNGOLOGY 2002, DC DECKER Figure 2 Theoretical pathway of a third branchial arch fistula. Nicoucar K et al. Otolaryngology -- Head and Neck Surgery 2010;142:21-28 Copyright © by American Academy of Otolaryngology- Head and Neck Surgery Fourth branchial arch ADAPTED FROM: BLUESTONE, SURGICAL ATLAS OF PEDIATRIC OTOLARYNGOLOGY 2002, DC DECKER Fourth branchial arch Congenital ‐ Vascular Lymphatic malformations ◦ Perkins JA. Lymphatic malformations: Review of current treatment. Otolaryngol Head Neck Surg 2010;142:795‐803. ◦ Imaging ◦ CT/MRI ◦ Staging ◦ de Serres LM. Lymphatic malformations of the head and neck. A proposal for staging. Arch Otolaryngol Head Neck Surg 1995;121:577‐82. ◦ Macro v microcystic ◦ Sclerotherapy v excision Perkins J A et al. Otolaryngology -- Head and Neck Surgery 2010;142:795-803.e1 Copyright © by American Academy of Otolaryngology- Head and Neck Surgery 3 year old Female Right neck mass Presented after diagnosed with ear infection by pediatrician Unchanged >3 months Asymptomatic Branchial cyst? Lymphatic malformation? Plan for the worst Lymphatic malformation Lymphatic malformation Congenital ‐ Vascular Hemangiomas ◦ Complete resolution ◦ 50% by 5 years ◦ 70% by 7 years ◦ Propranolol ◦ Leaute‐Labreze C, Dumas de la Roque E, Hubiche T, et al. Propranolol for severe hemangiomas of infancy. N Engl J Med 2008;358:2649‐2651. ◦ Cushing SL. Initial experience with a multidisciplinary strategy for initiation of propranolol therapy for infantile Hemangiomas. Otolaryngol Head Neck Surg 2011;144:78‐ 84. Hemangioma Lymphadenopathy Infectious ??? Inflammatory Lymphadenopathy Non‐infectious Neoplastic Lymphadenopathy (>2 cm) 90% of children 4‐8 yrs will have cervical adenopathy ◦ Park YW. Evaluation of neck masses in children. Am Family Physician 1995;51:1904‐1912 Infection v Cancer? When to biopsy? FNA v Excisional biopsy? Infectious Viral (most common) ◦ Nonspecific (URI) ◦ Epstein‐Barr virus ◦ HIV Bacterial ◦ AOM, pharyngitis, odontogenic, sinusitis, cat scratch, mycobacteruim ◦ Timothy T. The rising incidence of methicillin‐resistant Staphylococcus aureus in pediatric neck abscesses. Otolaryngol Head Neck Surg. 137; 2007 ◦ 245 patients, Dallas TX ◦ MRSA 27% ◦ MSSA 23% ◦ Group A Strep 20% ◦ B. henselae 2% ◦ Mycobacterium <1% Non‐infectious ◦ Kawasaki disease ◦ 19/100,000 children in US ◦ Fever >5 days ◦ Cervical lymphadenopathy ◦ Edema/erythema palms/soles ◦ B/L conjunctivitis ◦ Strawberry tongue ◦ Kikuchi‐Fujimoto disease ◦ Rosai‐Dorfman ◦ Langerhans cell histiocytosis JONATHAN D.K. TRAGER, M.D. KAWASAKI'S DISEASE. N ENGL J MED 1995; 333:1391 Neoplastic Lymphoma (most common in children) Rhabdomyosarcoma (second most common in children) Thyroid carcinoma (third most common), (adolescent girls) Salivary gland (uncommon) Neurogenic sarcoma, NPC, neuroblastoma Lymphadenopathy – Clinical approach Acute < 2 weeks ◦ Broad spectrum antibiotic – 2 week course Subacute 2‐6 weeks ◦ ◦ ◦ ◦ ◦ ◦ ◦ CBC PPD CXR EBV Bartonella ? Toxoplasma, HIV, Syphilis, LDH (lymphoma), urine VMA (neuroblastoma) ? Biopsy Chronic > 6 weeks ◦ Biopsy Lymphadenopathy ‐‐ Clinical approach Biopsy ◦ ◦ ◦ ◦ Supraclavicular node 2‐6 weeks, > 3 cm, no response to abx, 2‐6 weeks with risk factors for malignancy > 6 weeks FNA? ◦ Excisional bx is gold standard ◦ Chau et al. Rapid access multidisciplinary lymph node clinic: analysis of 550 patients. Br J Cancer 2003;10:354‐61. ◦ 289 lymph node FNAs ◦ 97% specificity, 49% sensitivity, 45% false negative rate ◦ 83% of false negatives were lymphomas Atypical mycobacterium M. avium‐intracellulare, M. haemophilum (90%) Submandibular (50%), cervical (25%), preauricular (10%) PPD + (85%) Observation +/‐ abx ◦ 6 months (71%) ◦ 9 months (98%) ◦ 12 months (100%)1 Surgical excision or curettage 1ZAHARIA A. MANAGEMENT OF NONTUBERCULOUS MYCOBACTERIA‐INDUCED CERVICAL LYMPHADENITIS WITH OBSERVATION ALONE. PEDIATR INFECT DIS J 2008;27:920‐2 Cat scratch disease Bartonella Henselae C. Felis (cat fleas) Primary inoculation lesion Serology Self limited, 6‐12 weeks Doxycycline, erythromycin ◦ Immunocompromised patient Surgery rarely indicated ◦ Biopsy often negative