Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
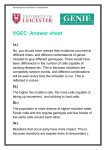
BMB reports Distinct mutations in MLH1 and MSH2 genes in Hereditary Non-polyposis Colorectal Cancer (HNPCC) families from China 1,# 2,# 1,3,# 3 4 1 1 2 Wenqian Wei , Fangqi Liu , Lei Liu , Zuofeng Li , Xiaoyan Zhang , Fan Jiang , Qu Shi , Xiaoyan Zhou , Weiqi 2 2 3 2 1 Sheng , Sanjun Cai , Xuan Li *, Ye Xu * & Peng Nan * 1 Ministry of Education Key Laboratory for Biodiversity Science and Ecological Engineering, School of Life Sciences, Fudan University, Shanghai 200433, 2Colorectal Surgery, Shanghai Cancer Hospital of Fudan University, Shanghai 20032, 3Shanghai Center for Bioinformation Technology, Shanghai, 200235, 4School of Life Science and Technology, Tongji University, Shanghai 200092, China Hereditary non-polyposis Colorectal Cancer (HNPCC) is an autosomal dominant inheritance syndrome. HNPCC is the most common hereditary variant of colorectal cancer (CRC), which accounts for 2-5% CRCs, mainly due to hMLH1 and hMSH2 mutations that impair DNA repair functions. Our study aimed to identify the patterns of hMSH2 and hMLH1 mutations in Chinese HNPCC patients. Ninety-eight unrelated families from China meeting Amsterdam or Bethesda criteria were included in our study. Germline mutations in MLH1 and MSH2 genes, located in the exons and the splice-site junctions, were screened in the 98 probands by direct sequencing. Eleven mutations were found in ten patients (11%), with six in MLH1 (54.5%) and five in MSH2 (45.5%) genes. One patient had mutations in both MLH1 and MSH2 genes. Three novel mutations in MLH1 gene (c.157_160delGAGG, c.2157dupT and c.-64G>T) were found for the first time, and one suspected hotspot in MSH2 (c.1168C>T) was revealed. [BMB reports 2011; 44(5): 317-322] INTRODUCTION Hereditary nonpolyposis colorectal cancer (HNPCC) (MIM#120435), also known as Lynch syndrome, is the most common known form of hereditary colorectal cancer (CRC) (1). It accounts for approximately 2-5% of all the colorectal cancer cas- *Corresponding author. Peng Nan, Tel: 86-21-65642957; Fax: 8621-65642468; E-mail: [email protected], Ye Xu, Tel: 86-2164175590 Ext1106; Fax: 86-21-64035387; E-mail: xu.shirley021@ gmail.com, Xuan Li, Tel: 86-21-54924305; Fax: 54924015; E-mail: [email protected] # These authors contributed equally to this work. DOI 10.5483/BMBRep.2011.44.5.317 Received 4 January 2011 , Accepted 22 February 2011 Keywords: HNPCC, MLH1, MSH2, Mutations http://bmbreports.org es (2). It is an autosomal dominant inheritance syndrome associated with heritable defects in DNA mismatch repair genes (MMR). HNPCC is characterized by earlier onset of colorectal cancer, proximal colonic cancer predominance, and an increased incidence of cancer in extracolonic organs such as endometrial, stomach, ovary, small bowel, hepatobiliary tract, renal pelvis, ureter, skin, and brain (3, 4). Germline mutations in at least 5 DNA mismatch-repair genes (MMR) cause HNPCC: MLH1 (3p21-23) (MIM*120436), MSH2 (2p21) (MIM*609309), MSH6 (2p21) (MIM*600678), PMS1 (2q31- q33) (MIM*600258), and PMS2 (7p22) (MIM*600259). Most (90%) of the mutations were found in two MMR genes: MLH1 (50%) and MSH2 (40%), whereas 7% mutations occurred in MSH6 and 3% for the remaining genes (5). The Amsterdam criteria were established by the International Collaborative Group on Hereditary Nonpolyposis Colorectal Cancer (ICG-HNPCC) in 1990. As the widely accepted criteria for diagnosis of HNPCC, it has some limitations. It is too restrictive and difficult to identify HNPCC cases in small family (2). Thus, some other guidelines, such as Bethesda criteria, were also formed to identify suspected patients (6). The golden standard for diagnostic of HNPCC is germline mutation in MMR genes. At present, direct sequencing is the key procedure in recognizing MMR genes defects. As most studies of HNPCC are limited in race and sample sizes, several MMR gene mutation databases were established to share data around the world. The most authoritative one is InSiGHT (http://www.insight-group.org/mutations/), set up by the International Society of Gastrointestinal Hereditary Tumors. InSiGHT collected a large amount of data on MLH1 and MSH2 genes. The total number of variants for MLH1 was 6079, and for MSH2 was 4428 (accessed in May 2010). Also there is a database with unclassified variants (www.mmruv.info) supporting the InSiGHT. Our previous studies based on InSiGHT suggested there were differences in MLH1 and MSH2 mutations between Caucasian and Asian populations (7). In the meantime, Sheng et al. indicated that the incidence of early onset CRC in Hong BMB reports 317 Mutations in MLH1 & MSH2 genes in HNPCC families from China Wenqian Wei, et al. Kong, was more than Western countries (8). A predominance of distal tumors (9) and primary extracolonic tumors in stomach (10) in Asian HNPCC patients were reported, which were also different from those in Western countries. Kim et al. found the three novel germline mutations in MLH1 and MSH2 in Korea (11). The study was to analyze MLH1 and MSH2 mutations in 98 unrelated probands of the suspected HNPCC families, which is one of the large scale studies in Chinese population. In addition to those reported, several novel MLH1 and MSH2 mutations and a suspected hotspot in the group of Chinese HNPCC patients were identified. RESULTS A total of eleven mutations were found in ten patients (11%) from the 98 probands, with six in MLH1 (54.5%) and five in MSH2 (45.5%) genes (Table 1). Four families who met the Amsterdam criteria harbored mutations, and six families who met Bethesda criteria had mutations. Three novel mutations which had never been reported were founded in patients H76 (MLH1 c.157_160delGAGG), H86 (MLH1 c.-64G>T) and H224 (MLH1 c.2157dupT). There were five mutations previously reported, including one known polymorphism in MLH1 c.655A>G (dsSNP1799977). Interestingly, c.1168C>T of MSH2, a missense mutation, was found in four unrelated probands (H88, H224, H231 and H245). Furthermore, one patient (H224) was a compound heterozygote for a novel pathogenic frameshift mutation in MLH1 and a missense mutation in MSH2. Patient H86 Sequence analysis of MLH1 revealed a novel G>T substitution at nucleotide -64 (Fig. 1a), which is in the promoter area. It may result in alteration or loss of MLH1 gene function. No mutation was identified in MSH2. Patient H76 Sequence analysis of MLH1 coding area revealed the deletion of four nucleotides GAGG at 157_160 in exon 2 (Fig. 1b). This deletion caused a frameshift mutation, results in the replacement of a Gly with an Ala at codon 54, and early termination at two amino acids after. Comprehensive sequence analysis of MLH1 and MSH2 genes revealed no other mutations. Patient H224 An insertion (c.2157dupT, Fig. 1c) in MLH1 was found in patient H224, which resulted in a frameshift mutation and replacement of Val with Cys at codon 720, and ended in three amino acids. Meanwhile, a C>T substitution at nucleotide 1168, resulted in the replacement of a phenylalanine-encoding codon with a leucine-encoding codon at codon 390 in MSH2 gene. DISCUSSION In this study, eleven germline mutations were found in ten probands. Among them were eight distinct mutations, all of which were heterozygote. Although some researchers found bi-allelic mutations in HNPCC patients, most alterations are mono-allelic. Among the eight germline mutations we identified, four are missense mutations, two are frameshift mutations, one is aberrant splicing, and one is in promoter area. Missense mutations are also the common mutation type in Chinese population. The missense mutations (MLH1 c.655A>G, MLH1 c.2042C>T, MSH2 c.23C>T and MSH2 c.1168C>T) were identified as “missense mutations of unknown significance”, functions of which were controversial. Four probands had one same mutation - MSH2 c.1168C>T (p.L390P). We searched for MSH2 c.1168C>T in InSiGHT database and the original papers, and found the mutations (about 80%) frequently occurred in East Asia populations, including Table 1. Germline MLH1 and MSH2 mutations in all patients Family ID H9 H76 H86 H88 H166 H167 H224 H231 H236 H245 Mutation Gene Exon MSH2 MLH1 MLH1 MSH2 MLH1 MLH1 MLH1 MSH2 MSH2 MLH1 MSH2 1 2 1 7 8 17 19 7 7 18 7 Nucleotide c.23C>T c.157_160del GAGG c.-64G>T c.1168C>T c.655A>G c.1989G>A c.2157dupT c.1168C>T c.1168C>T c.2042C>T c.1168C>T Consequence p.Thr8Met p.Gly54Alafs*2 p.Phe390Leu p.Ile219Val p.Val720Cysfs*3 p.Phe390Leu p.Phe390Leu p.Ala681Val p.Phe390Leu Type Missense Frameshift Uncertain Missense Missense Aberrant splicing Frameshift Missense Missense Missense Missense Clinical criteria Amsterdam Amsterdam Bethesda Bethesda Amsterdam Amsterdam Bethesda Bethesda Bethesda Bethesda Having been reported (times)# Yes (5) No No Yes (34) Yes (224) Yes (2) No Yes (34) Yes (34) Yes (1) Yes (34) # According to the InSiGHT database (http://www.insight-group.org/mutations/), InSiGHT database is the largest and most authoritative database in HNPCC studies, which integrated the data from MMR Gene Unclassified Variants Database (www.mmruv.info), Mismatch Repair Genes Variants Database (www.med.mun.ca/MMRvariants), and the Human Gene Mutation Database (www.hgmd.cf.ac.uk/ac). By May 2010, the InSiGHT database lists a total number of 6079 and 4428 variants and 1079 and 924 unique DNA mutations for MLH1 and MSH2, respectively. 318 BMB reports http://bmbreports.org Mutations in MLH1 & MSH2 genes in HNPCC families from China Wenqian Wei, et al. Fig. 2. Reported MSH2 c.1168C>T variants. The percentage of the patients’ number in MSH2 c.1168 C>T based on the InSiGHT database and the original papers. Fig. 1. Three novel mutations found in patients H86, H76 and H224. (a) A single nucleotide substitution (G>T) at position -64 in the promoter region of the MLH1 gene in patient H86. (b) Comparison of sequence pattern of exon 2 in MLH1 both normal and patient H76, deletion of four nucleotides (GAGG) in patient H76. (c) Sequence analysis of exon 19 in MLH1, insertion of one nucleotide (T) in patient H224. http://bmbreports.org Chinese Han, Japanese, Korean and Singaporean (Fig. 2). However, in a study of 1721 German suspected HNPCC families, Mangold detected no instance of MSH2 c.1168C>T (12). Although this mutation was first reported by Konishi in 1996, its function is still controversial (13). Banno et al. found this mutation in two out of eleven (18%) endometrial cancer patients who had family histories of colorectal and endometrial carcinoma. Later, a high occurrence rate (7%) of the mutation was observed among 179 healthy Japanese individuals, so it was reported to be a polymorphorism but not a causative mutation for CRC (14). Kim et al. also reported this mutation as SNP in healthy Korean individuals, which showed no association with sporadic colorectal cancer (15), and was recently identified as SNP (dsSNP17224367). However, Chen et al. suggested this mutation might cause a polarity change at the margin of the interaction region of MSH2 (16). Fan et al. analyzed molecular epidemiologic, structural, bioinformatic and functional information of MSH2 c.1168C>T. They found this variant in 4.89% of CRC and only in one healthy individual (0.89%). This variant resulted in a phenotype relevant to young sporadic CRC or GC, which was suspected as predisposing factor to gastrointestinal cancer (17). In the same year, Zhang et al. found significant difference in the frequency of MSH2 c.1168C>T between young-age patients and control individuals, and considered this mutation associated with an increased GC risk (18). In our study the incidence of MSH2 c.1168C>T is up to 4% in 98 HNPCC probands. This result is different from those Japanese and Korean studies. In Chinese study, incidence of MSH2 c.1168C>T is much higher in patients than in controls. MLH1 c.655A>G mutation was reported 224 times in InSiGHT database. In our study, one patient who fulfilled the Amsterdam criteria harbor MLH1 c.655A>G mutation. The BMB reports 319 Mutations in MLH1 & MSH2 genes in HNPCC families from China Wenqian Wei, et al. significance of the sequence alteration is controversial. The c.655A>G variant is considered a polymorphism (dsSNP1799977) and was reported in HapMap database (www.hapmap.org). MLH1 c.655A>G is in a conserved region of exon 8, and both alleles result in non-polar and pH-neutral amino acids. Functional analyses suggest that the variant has DNA repair efficiency (19, 20) and binding properties to PMS2 are similar to the wild type (21). According to the result by SIFT (http://sift.jvci.org), this polymorphism may be tolerated by MLH1 protein. But it is not an entirely benign mutation. Among sporadic colorectal cancer and young-onset lung cancer cases, c.655A>G was correlated with reduced MLH1 protein expression (15). This variant may even compromise the MLH1 function due to code change or change in the secondary structure of mRNA (22). Recently Takahashi et al. provided evidence to support this hypothesis by in vitro MMR assay (23). Campbell et al. reported association of the MLH1 c.655A>G variant with colon cancer risk for the people with a high Western diet pattern (24). The association was extended to CRC patients by Nejda et al., who showed patients with this variant displayed a better outcome in sporadic colorectal cancer (25). This variant is not only involved in colorectal cancer, but also in some other types of cancers. MLH1 c.655A>G was associated with an almost fivefold increased risk of ulcerative colitis (26), and 6- to 16-fold increased risk of acute lymphoblastic leukaemia when combined with known genotypes of increased susceptibility to leukeamia (27). The variant may be associated with the young-onset of lung cancer, especially in histological squamous cell type (28), and may influence the disease onset of prostate cancer (29). Our results suggest a possible role of MLH1 c.655A>G polymorphism in the Chinese HNPCC group, and it remains to be further investigated with additional samples. We found three novel germline mutations. Two of these novel mutations caused frameshift mutations in MLH1 gene (H76 and H224) and made the coding terminate earlier. Both of them were considered as pathogenic. The other one (H86) was found in the promoter area of MLH1 (c.-64G>T). Previous researches found connection between mutations in promoter area and diseases. The most frequent one in MLH1 gene is −93G>A, While it is considered a SNP, some researchers noticed it was associated with CRC. Campbell et al. and Raptis et al. found that −93G>A was associated with an increased risk of MSI-H CRC (24, 30). And in the study by Allan et al., the risk in developing CRC increased to 3-fold, particularly in patients with somatic loss of MLH1 protein expression (31). In addition, Zhong et al. found MLH1 −107C> G in three out of 163 CRC patients. They also found that this variant reduced transcriptional activity by 51% and impeded the promoter-binding capacity of nuclear proteins (32). Green et al. demonstrated that the MLH1 promoter with −42C>T was less effective in binding nuclear proteins, and had only 37% of the activity of the wild-type promoter in driving the expression of a reporter gene in vivo (33). So this novel mutation 320 BMB reports we found in MLH1 promoter area may impair MLH1 protein function and may be associated with HNPCC. We described one proband (H224) fulfilling Bethesda criteria with two different mutations in MLH1 and MSH2 - one was a novel pathogenic frameshift mutation MLH1 c.2157 dupT, and the other one was a missense mutation MSH2 c.1168C>T. Such rare case of double mutations was reported before by others, in which patients were found to have two alterations in both MLH1 and MSH2 genes, and in most of the cases, one was a deletion and the other one was a point mutation (34). MATERIALS AND METHODS Patients Ninety-eight families with HNPCC or suspected HNPCC were studied from 1994 to 2008 in Shanghai Cancer Hospital of Fudan University. All were native Chinese without immigrant ancestors. Fifteen families fulfilled Amsterdam II criteria and were classified as Amsterdam group. The rest 83 families who met the Bethesda criteria were classified as Bethesda group. The study was approved by the Ethics Committee of Shanghai Cancer Hospital of Fudan University, and the number of Ethics Committee was 050432-4-1008A. Extraction of DNA from blood Blood samples were taken from 98 probands. Genomic DNA was isolated from peripheral blood lymphocytes according to the manufacturer’s instructions (TIANGEN BIOTECH, BEIJING). o The extracted genomic DNA was stored at −20 C for further analysis. Mutation of MLH1 and MSH2 genes Exons 1-19 of MLH1 and exons 1-16 of MSH2, including the splice-site junctions, were amplified by polymerase chain reaction (TaKaKa Biotechnology, Dalian). The PCR products were purified by 1.5% agarose gel electrophoresis, following the manufacturer’s instructions (TIANGEN BIOTECH, BEIJING). All the purified products were sequenced by Shanghai Sunny Biotechnology Co., Ltd with 3730XL of ABI. Each mutation was amplified both the sense and antisense strand, and then the experiment was repeated at least once. If the mutation was exactly the same through at least three repeated experiments, the mutation was confirmed. By comparing with the reference sequences, missense and frameshift mutations were identified. We submitted eleven mutations, six from MLH1 and five from MSH2 gene from ten patients to InSiGHT database (http:// www.insight-group.org/mutations/). The IDs of the three novel mutations are: MLH1-01495, MLH1-01496, and MLH1-01497. Definition of pathogenic mutations Sequence variants which would obviously impact the function of MLH1 or MSH2 proteins, such as nonsense and frameshift mutations, were considered pathogenic. Besides, the mutahttp://bmbreports.org Mutations in MLH1 & MSH2 genes in HNPCC families from China Wenqian Wei, et al. tions at highly conserved splice sites were also considered pathogenic. All the missense mutations were assessed for pathogenicity by searching against the InSiGHT database (http:// www.insight-group.org/mutations/), MMR Gene Unclassified Variants Database (www.mmruv.info), Mismatch Repair Genes Variants Database (www.med.mun.ca/MMRvariants), and the Human Gene Mutation Database (www.hgmd.cf.ac.uk/ac). If the missense mutations affected the promoter site, or have been reported as pathogenic mutations in other studies, they were also considered pathogenic. Those missense mutations whose pathogenicity could not be confirmed were classified as uncertain. Acknowledgements This study was supported by the grants from the 863 Hi-Tech Program of China (2009AA02Z308, 2007AA02Z332, 2008AA02Z126), the Shanghai Project (07D19505, B111). REFERENCES 1. Lynch, H. T. and Smyrk, T. (1996) Hereditary nonpolyposis colorectal cancer (Lynch syndrome): An updated review. Cancer 78, 1149-1167. 2. Lynch, H. T. and de la Chapelle, A. (1999) Genetic susceptibility to non-polyposis colorectal cancer. J. Med. Genet. 36, 801-818. 3. Ricciardiello, L. and Boland, C. (2005) Lynch syndrome (hereditary non-polyposis colorectal cancer): Current concepts and approaches to management. Curr. Gastroenterol. Rep. 7, 412-420. 4. Lynch, H. T. and de la Chapelle, A. (2003) Hereditary colorectal cancer. New Engl. J. Med. 348, 919-932. 5. Peltomaki, P. and Vasen, H. (2004) Mutations associated with HNPCC predisposition - Update of ICG-HNPCC/ INSiGHT mutation database. Dis. Markers 20, 269-276. 6. Wijnen, J. T., Vasen, H. F. A., Khan, P. M., Zwinderman, A. H., van der Klift, H., Mulder, A., Tops, C., Møller, P., Fodde, R., Menko, F., Taal, B., Nagengast, F., Brunner, H., Kleibeuker, J., Sijmons, R., Griffioen, G., BröckerVriends, A., Bakker, E., van Leeuwen-Cornelisse, I., Meijers-Heijboer, A., Lindhout, D., Breuning, M., Post, J., Schaap, C., Apold, J., Heimdal, K., Bertario, L., Bisgaard, M. L. and Goetz, P. (1998) Clinical findings with implications for genetic testing in families with clustering of colorectal cancer. New Engl. J. Med. 339, 511-518. 7. Wei, W. Q., Liu, L., Chen, J., Jin, K., Jiang, F., Liu, F. Q., Fan, R., Cheng, Z., Shen, M., Xue, C. Y., Cai, S. J., Xu, Y., and Nan, P. (2010) Racial differences in MLH1 and MSH2 mutation: an analysis of yellow race and white race based on the InSiGHT. J. Bioinform. Comp. Biol. 8 (Suppl 1), 111-125. 8. Sheng, J. Q., Chan, T. L., Chan, Y. W., Huang, J. S., Chen, J. G., Zhang, M. Z., Guo, X. L., Mu, H., Chan, A. S., Li, S. R., Yuen, S. T. and Leung, S. Y. (2006) Microsatellite instability and novel mismatch repair gene mutations in northern Chinese population with Hereditary non-polyposis colorectal cancer. Chinese J. Digest. Dis. 7, 197205. http://bmbreports.org 9. Chew, M. H., Koh, P. K., Ng, K. H., Lim, J. F., Ho, K. S., Ooi, B. S., Tang, C. L. and Eu, K. W. (2008) Phenotypic characteristics of hereditary non-polyposis colorectal cancer by the Amsterdam criteria: an Asian perspective. ANZ J. Surg. 78, 556-560. 10. Cai, S. J., Xu, Y., Cai, G. X., Lian, P., Guan, Z. Q., Mo, S. J., Sun, M. H., Cai, Q. and Shi, D. R. (2003) Clinical characteristics and diagnosis of patients with hereditary nonpolyposis colorectal cancer. World J. Gastroenterol. 9, 284-287. 11. Kim, Y. M., Choe, C. G., Cho, S. K., Jung, I. H., Chang, W. Y. and Cho, M. (2010) Three novel germline mutations in MLH1 and MSH2 in families with Lynch syndrome living on Jeju island, Korea. BMB Rep. 43, 693697. 12. Mangold, E., Pagenstecher, C., Friedl, W., Mathiak, M., Buettner, R., Engel, C., Loeffler, M., Holinski-Feder, E., Muller-Koch, Y., Keller, G., Schackert, H. K., Kruger, S., Goecke, T., Moeslein, G., Kloor, M., Gebert, J., Kunstmann, E., Schulmann, K., Ruschoff, J. and Propping, P. (2005) Spectrum and frequencies of mutations in MSH2 and MLH1 identified in 1,721 German families suspected of hereditary nonpolyposis colorectal cancer. Int. J. Cancer 116, 692-702. 13. Konishi, M., Kikuchi-Yanoshita, R., Tanaka, K., Muraoka, M., Onda, A., Okumura, Y., Kishi, N., Iwama, T., Mori, T., Koike, M., Ushio, K., Chiba, M., Nomizu, S., Konishi, F., Utsunomiya, J. and Miyaki, M. (1996) Molecular nature of colon tumors in hereditary nonpolyposis colon cancer, familial polyposis, and sporadic colon cancer. Gastroenterology 111, 307-317. 14. Banno, K., Susumu, N., Nozawa, S. and Sugano, K. (2004) Met688Ile and Leu390Phe of the MSH2 gene are not functional mutations, but polymorphisms in Japanese individuals. Cancer Genet. Cytogenet. 155, 92. 15. Kim, J. C., Roh, S. A., Koo, K. H., Ka, I. H., Kim, H. C., Yu, C. S., Lee, K. H., Kim, J. S., Lee, H. I. and Bodmer, W. F. (2004) Genotyping possible polymorphic variants of human mismatch repair genes in healthy Korean individuals and sporadic colorectal cancer patients. Fam. Cancer 3, 129-137. 16. Chen, C. H., Huang, R. L., Yu, M. S., Wong, L. J., Chao, T. F. and Chu, T. Y. (2001) Hereditary nonpolyposis colorectal cancer with gynecologic malignancies: report of two families in Taiwan. J. Formos. Med. Assoc. 100, 269-273. 17. Fan, Y., Liu, X., Zhang, H., Dai, J., Zhang, X., Zhu, M., Gao, X. and Wang, Y. (2006) Variations in exon 7 of the MSH2 gene and susceptibility to gastrointestinal cancer in a Chinese population. Cancer Genet. Cytogenet. 170, 121-128. 18. Zhang, Y., Liu, X., Fan, Y., Ding, J., Xu, A., Zhou, X., Hu, X., Zhu, M., Zhang, X., Li, S., Wu, J., Cao, H., Li, J. and Wang, Y. (2006) Germline mutations and polymorphic variants in MMR, E-cadherin and MYH genes associated with familial gastric cancer in Jiangsu of China. Int. J. Cancer 119, 2592-2596. 19. Raevaara, T. E., Korhonen, M. K., Lohi, H., Hampel, H., Lynch, E., Lönnqvist, K. E., Holinski-Feder, E., Sutter, C., McKinnon, W., Duraisamy, S., Gerdes, A.-M., Peltomäki, P., Kohonen-Ccorish, M., Mangold, E., MacRae, F., BMB reports 321 Mutations in MLH1 & MSH2 genes in HNPCC families from China Wenqian Wei, et al. 20. 21. 22. 23. 24. 25. 26. 27. Greenblatt, M., de la Chapelle, A. and Nyström, M. (2005) Functional significance and clinical phenotype of nontruncating mismatch repair variants of MLH1. Gastroenterology 129, 537-549. Trojan, J., Zeuzem, S., Randolph, A., Hemmerle, C., Brieger, A., Raedle, J., Plotz, G., Jiricny, J. and Marra, G. (2002) Functional analysis of hMLH1 variants and HNPCC-related mutations using a human expression system. Gastroenterology 122, 211-219. Kondo, E., Suzuki, H., Horii, A. and Fukushige, S. (2003) A yeast two-hybrid assay provides a simple way to evaluate the vast majority of hMLH1 germ-line mutations. Cancer Res. 63, 3302-3308. Marais, G. and Duret, L. (2001) Synonymous codon usage, accuracy of translation, and gene length in caenorhabditis elegans. J. Mol. Evol. 52, 275-280. Takahashi, M., Shimodaira, H., Andreutti-Zaugg, C., Iggo, R., Kolodner, R. D. and Ishioka, C. (2007) Functional analysis of human MLH1 variants using yeast and in vitro mismatch repair assays. Cancer Res. 67, 4595-4604. Campbell, P. T., Curtin, K., Ulrich, C. M., Samowitz, W. S., Bigler, J., Velicer, C. M., Caan, B., Potter, J. D. and Slattery, M. L. (2009) Mismatch repair polymorphisms and risk of colon cancer, tumour microsatellite instability and interactions with lifestyle factors. Gut 58, 661-667. Nejda, N., Iglesias, D., Moreno Azcoita, M., Medina Arana, V., González-Aguilera, J. J. and Fernández-Peralta, A. M. (2009) A MLH1 polymorphism that increases cancer risk is associated with better outcome in sporadic colorectal cancer. Cancer Genet. Cytogenet. 193, 71-77. Bagnoli, S., Putignano, A. L., Melean, G., Baglioni, S., Sestini, R., Milla, M., d'Albasio, G., Genuardi, M., Pacini, F., Trallori, G. and Papi, L. (2004) Susceptibility to refractory ulcerative colitis is associated with polymorphism in the hMLH1 mismatch repair gene. Inflamm. Bowel Dis. 10, 705-708. Mathonnet, G., Krajinovic, M., Labuda, D. and Sinnett, D. (2003) Role of DNA mismatch repair genetic polymorphisms in the risk of childhood acute lymphoblastic 322 BMB reports leukaemia. Br. J. Haematol. 123, 45-48. 28. An, Y., Jin, G., Wang, H., Wang, Y., Liu, H., Li, R., Wang, H., Qian, J., Sun, W., Ma, H., Miao, R., Hu, Z., Jin, L., Wei, Q., Shen, H., Huang, W. and Lu, D. (2008) Polymorphisms in hMLH1 and risk of early-onset lung cancer in a southeast Chinese population. Lung Cancer 59, 164-170. 29. Fredriksson, H., Ikonen, T., Autio, V., Matikainen, M. P., Helin, H. J., Tammela, T. L. J., Koivisto, P. A. and Schleutker, J. (2006) Identification of germline MLH1 alterations in familial prostate cancer. Eur. J. Cancer 42, 2802-2806. 30. Raptis, S., Mrkonjic, M., Green, R. C., Pethe, V. V., Monga, N., Chan, Y. M., Daftary, D., Dicks, E., Younghusband, B. H., Parfrey, P. S., Gallinger, S. S., McLaughlin, J. R., Knight, J. A. and Bapat, B. (2007) MLH1 -93G>A promoter polymorphism and the risk of microsatellite- unstable colorectal cancer. J. Natl. Cancer I. 99, 463-474. 31. Allan, J. M., Shorto, J., Adlard, J., Bury, J., Coggins, R., George, R., Katory, M., Quirke, P., Richman, S., Scott, D., Scott, K., Seymour, M., Travis, L. B., Worrillow, L. J., Bishop, D. T. and Cox, A. (2008) MLH1 −93G>A promoter polymorphism and risk of mismatch repair deficient colorectal cancer. Intl. J. Cancer 123, 2456-2459. 32. Zhong, X., Arita, M., Yamada, K., Sugiyama, H., Tan, K., Kanazawa, S., Koike, J., Teramoto, T. and Hemmi, H. (2007) A single nucleotide substitution (−107C→G) in the hMLH1 promoter found in colorectal cancer population reduces transcriptional activity. Biochem. Genet. 45, 671-681. 33. Green, R., Green, A., Simms, M., Pater, A., Robb, J. and Green, J. (2003) Germline hMLH1 promoter mutation in a Newfoundland HNPCC kindred. Clin. Genet. 64, 220227. 34. Lee, S. C., Guo, J. Y., Lim, R., Soo, R., Koay, E., SaltoTellez, M., Leong, A. and Goh, B.-C. (2005) Clinical and molecular characteristics of hereditary non-polyposis colorectal cancer families in Southeast Asia. Clin. Genet. 68, 137-145. http://bmbreports.org