Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
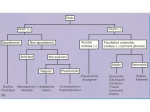
CCl Introductory Characteristics Obligate anaerobes Gram positive Capable of producing endospores Rod-shaped, named after Greek word for spindle, kloster Club-shaped, as well: endospores form club end Saprophytes found in soil, water, decomposing matter Classification: A. Tetanus – Cl.tetani B. Gas gangrene – 1. Established pathogens-Cl.perfringens Cl.septicum Cl.novyi 2. Less pathogenic – Cl.histolyticum Cl.fallax 3. Doubtful pathogens- Cl.bifermentans Cl.sporogenes C. Food poisoning- 1. Gastroenteritis – Cl.perfringens (type A) 2. Necrotising enteritis – Cl.perfringens ( type C) 3. Botulism – Cl.botulinum D. Acute colitis – Cl.difficle Gram positive, spore forming bacilli, highly pleomorphic Shape and position of spores varies in different species and is useful in identification of clostridia Distribution of spores: 1. Central or equatorial – Cl.bifermentans 2. Sub-terminal – Cl.perfringens 3. Oval and terminal – Cl.tertium 4. Spherical and terminal – Cl.tetani Culture: Clostridia grow well on ordinary media under anaerobic conditions Liquid media- Robertson’s cooked meat broth (RCM), thioglycollate broth are very useful RCM contains unsaturated fatty acids which take up oxygen, reaction being catalysed by hematin in meat and sulphydryl compounds (they lower down the redox potential) Thioglycollate broth contains reducing agent thioglycollate More important than the absence of oxygen is the provision of a sufficiently low redox potential in the medium Reducing substances that can be used are- unsaturated fatty acids, ascorbic acid, glutathione, cysteine, thioglycollic acid, alkaline glucose, sulphites, metallic iron Growth of clostridia results in turbid broth Most species produce gas Saccharolytic species turn the meat pink Proteolytic species turn the meat black and produce foul smell Small concentration of CO2 enhances growth Inoculated plates ( eg: blood agar) are placed in anaerobic jar and incubated at 370 C for 2-3 days Resistance: spores exhibit variable resistance Cl.tetani spores persist for years in dried earth Cl.perfringens spores are destroyed by boiling for less than 5 mins except type A which takes several hours Cl.botulinum spores are not killed completely even at 1050C for less than 100 mins All spores get killed at 1210C for 20 mins (autoclaving) Halogens, glutaraldehyde are effective Clostridium tetani Causative agent of tetanus Widely distributed in soil and intestine of man and animals Morphology: Gram positive slender bacilli Spherical terminal spores giving the characteristic drumstick appearance Non capsulated, motile Culture: Obligate anaerobe Grow well on Robertson’s cooked meat broth, thioglycollate broth, blood agar In RCM growth occurs as turbidity and gas formation seen Meat is not digested, but becomes black on prolonged incubation Bacilli produce swarming growth on blood agar ( thin spreading film) Biochemical reactions : Cl.tetani has mild proteolytic but no saccharolytic property Does not ferment any sugar Greenish fluorescence is produced on media containing neutral red (MacConkey’s agar) Resistance: Spores can survive for years in soil Autoclaving kills all spores Classification: 10 serological types (I to X) based on type specific flagellar H antigens by agglutination test Toxins: Tetanolysin (hemolysin) Tetanospasmin (neurotoxin) Tetanolysin is heat labile oxygen labile toxin causing lysis of RBC Tetanospamin is a heat labile oxygen stable powerful neurotoxin, protein in nature, good antigen, responsible for pathogenesis of tetanus, neutralised by antitoxin Tetanus Is characterised by tonic muscular spasms, usually commencing at the site of infection and becoming generalised, involving the whole of somatic muscular system Etiology: Clostridium tetani Route of entry of pathogen: following any injury, puncture wounds, surgical operations with a lapse in asepsis, local suppuration, Otitis media, dental procedures, septic abortion, application of cow dung on umbilical stump or rituals like ear boring, circumcision Incubation period: 2 days to several weeks, commonly 6-12 days depending on factors like site and nature of wound, dose and toxigenicity of the strain, immune status of the patient IP is of prognostic significance, grave prognosis when it is short IP Tetanus was a serious disease with high mortality rate in the past Even with proper treatment case fatality rate varies from 15-50% Tetanus neonatorum and uterine tetanus are grave conditions with very high fatality rate Tetanus is more common in developing countries, where climate is warm, rural areas where soil is fertile, where human and animal populations live in close association, where unhygienic practices are common and medical facilities are poor In rural India, neonatal tetanus was common Pathogenesis: Infection strictly remains localised in the wound Germination of Cl.tetani spores and toxin production occur only if favourable conditions exist like: Reduced O-R potential, devitalised tissues and foreign bodies Toxin that is produced locally is absorbed by the motor nerve endings and transported to the central nervous system intra-axonally The toxin is specifically and avidly fixed by gangliosides of grey matter of nervous system Pathogenic effects are mainly due to tetanospasmin It resembles strychnine in its effects It specifically blocks synaptic inhibition in the spinal cord, presumably at the inhibitory terminals that use glycine and GABA as neurotransmitters The abolition of spinal inhibition causes uncontrolled spread of impulses initiated anywhere in the CNS This results in muscle rigidity and spasms due to simultaneous contraction of agonists and antagonists, in the absence of reciprocal inhibition Lock Jaw- initial symptom The convulsion pattern is determined by the most powerful muscles at a given point In most it is characterised by tonic extension of the body and of all limbs Muscular spasms leading to Opisthotonos in tetanus Laboratory diagnosis: Clinical diagnosis by history, symptoms and signs 1. Microscopy: Gram’s staining show Gram positive bacilli with drumstick appearance 2. Culture: Blood agar incubated at 370C for 24-48 hours under anaerobic conditions 3. Toxigenicity test: Animal testing Prophylaxis for tetanus: 1. Surgical 2. Antibiotics 3. Immunisation 1. Surgical: Removal of foreign body, blood clots etc to prevent favourable anaerobic conditions Simple cleaning of the wound to radical excision 2. Antibiotics: Penicillin, erythromycin 3. Immunisation: Tetanus is a preventable disease A) Active immunisation: Most effective method of prophylaxis Tetanus toxoid (formol toxoid) either as ‘plain toxoid’ or adsorbed on aluminium hydroxide( better antigen) Dosage: 0.5 ml Doses: 3 doses with an interval of 4 to 6 weeks Given as triple vaccine along with Diphtheria toxoid and pertussis vaccine Booster doses If wounding occurs 3 years or more after full course, booster dose given B) Passive immunisation: Antitetanus serum (ATS) prepared by immunising horses with toxoid Dose is 1500 IU by intramuscular route immediately after the person is wounded Risk of hypersensitivity reaction Homologous serum prepared from humans (HTIG) is with less risk of hypersensitivity Dose 250 units C) Combined prophylaxis: In non-immune person Combining active with passive immunisation First dose of TT in one arm along with administration of ATS or HTIG in another arm, followed by 2nd and 3rd doses of TT Adsorbed toxoid should be used here, plain toxoid may be interfered with ATS Treatment: Treated in special isolation unit in-order to protect from noise and light which may provoke convulsions Person to person transmission does not occur Controlling spasms, maintaining airway by tracheostomy Antitoxin, antibiotic therapy penicillin Recovering patients should receive full course of active immunisation, an attack of disease does not confer immunity Nature of wound Immune person Partially immune Non-immune Clean wound ( wound cleaning done within 6 hours) Toxoid 1 dose Toxoid 1 dose toxoid 3 doses Contaminated (Soil or other foreign material Toxoid 1 dose Toxoid 1 dose, TIG, antibiotics Toxoid 3 doses, TIG, antibiotics Infected wound Toxoid 1 dose, antibiotics Toxoid 1 dose, TIG, antibiotics Toxoid 3 doses, TIG, antibiotics Clostridium perfringens Also called Cl.welchii Is a commensal in large intestine of man and animals Spores are commonly found in soil and dust Morphology: Large, stout, Gram positive bacillus with sub-terminal spore Capsulated, non-motile Spores are rarely seen in ordinary culture media or in tissue (Characteristic feature), induced only in special media Culture: RCM, thioglycollate broth, blood agar Biochemical reactions: Predominantly saccharolytic but also have mild proteolytic action In litmus milk, lactose fermentation leads to formation of acid, which changes the colour of litmus from blue to red The acid coagulates the casein(acid clot) and the clotted milk is disrupted due to vigorous gas production This is known as Stormy fermentation Classification: Cl.perfringens produce 12 toxins Classification is based on production of 4 major toxins: alpha, beta, epsilon and iota 1. type A strains produce alpha toxin 2. type B strains produce alpha, beta and epsilon toxins 3. type C strains produce alpha and beta toxins 4. type D strains produce alpha and epsilon toxins 5. type E strains produce alpha and iota toxins Alpha (α ) toxin: Produced by all types of cl.perfringens but most abundantly by type A strains Chemically it is lecithinase C Is responsible for profound toxaemia in gas gangrene Relatively heat stable, lethal, dermonecrotic, hemolytic It splits lecithin, an important constituent of mammalian cell membrane This special effect is utilised for rapid detection of Cl.perfringens in clinical specimen (Nagler reaction) Nagler reaction: Cl.perfringens is grown on a medium containing 6% agar, 5% Filde’s peptic digest of sheep blood and 20% human serum or 5 % egg yolk Antitoxin is spread on one half of the plate and incubated at 370C for 24 hours Colonies on the half of plate without antitoxin will be surrounded by opacity while colonies on the other half with antitoxin shows no opacity This is due t0 specific neutralisation of the alpha toxin Alpha toxin splits lecithin into phosphoryl choline and a diglyceride (lipid) This lipid deposits around the colonies resulting in opacity Reverse CAMP test: Is similar to the CAMP test for identifying group B streptococci Here Clostridium species is inoculated in place of Staphylococcus aureus and a known group B streptococci is used Only Cl.perfringens exhibits accentuated zone of hemolysis as butterfly appearance Other major toxins: Beta, epsilon and iota toxins have lethal and necrotising properties Minor toxins: Gamma, eta have only minor lethal actions Delta toxin is lethal and hemolytic Theta toxin is oxygen labile Kappa toxin is a collagenase Lambda toxin is a proteinase and gelatinase Mu toxin is a hyaluronidase Nu toxin is a deoxyribonuclease Enterotoxin: Some strains of type A cause food poisoning and diarrhoea by producing this toxin Other soluble substances: Haemagglutinins, neuraminidase, fibrinolysin, hemolysin, histamine Bursting factor has specific action on muscle tissue and is responsible for the characteristic muscle lesions in gas gangrene Pathogenesis: 1. Gas gangrene: Cl.perfringens type A is the predominant bacterial agent causing gas gangrene When a wound gets contaminated by faecal matter or soil, it may lead to simple wound contamination, anaerobic cellulitis or myonecrosis When the muscle tissue is invaded it results in gas gangrene IP- 6 hours to 6 weeks 2. Food poisoning: Some strains of Type A produce enterotoxin IP 8-12 hours Cause: ingestion of cold or warmed up meat dish When contaminated meat is cooked, the spores in the interior may survive During storage or warming they germinate and multiply in the anaerobic environment in cooked meat Large numbers of clostridia is consumed which escapes gastric acid due to high protein in meal Reaches intestine and produces enterotoxin Symptoms: Pain abdomen, diarrhoea, vomiting Self-limited illness Recovery in 24-48 hours Diagnosis by isolating heat resistant Cl.perfringens type A from stool and food 3. Necrotising enteritis: Type C strains cause a severe and fatal necrotising jejunitis 4. Gangrenous appendicitis: Type A strains and occasionally type D strains 5. Other diseases: Urogenital infections, brain abscess, meningitis, panophthalmitis and puerperal infection Gas gangrene Is a rapidly spreading, edematous myonecrosis Occurs in association with severe wounds of extensive muscle masses that have been contaminated with pathogenic clostridia Etiology: 1. Established pathogens-Cl.perfringens Cl.septicum Cl.novyi 2. Less pathogenic – Cl.histolyticum Cl.fallax 3. Doubtful pathogens- Cl.bifermentans Cl.sporogenes Others: anaerobic streptococci, E.coli, Proteus, Staphylococci Route of entry of pathogen: Along with implanted foreign s like soil, road dust, bits of clothing etc Pathogenesis: MacLennon’s description of 3 types of anaerobic wound infections: Simple wound contamination Anaerobic cellulitis Anaerobic myositis or gas gangrene Favourable conditions for development of gas gangrene: crushing tissue or tearing of arteries produce anoxia of the muscle The Eh and pH of damaged tissues fall, breakdown of carbohydrates and muscle proteins provides a nourishing environment for anaerobes S/S: Increasing pain, tenderness, edema of the affected part along with systemic signs of toxaemia Thin watery discharge from the wound, later becomes profuse and sero-sanguinous Accumulation of gas makes the tissues crepitant Death occurs due to circulatory failure Lab diagnosis of gas gangrene: Specimen: exudates from wound, necrotic tissue and muscle fragments Direct microscopy: Gram’s staining of the specimen Culture: Aerobic and anaerobic culture Bacterial isolates are identified by morphology, cultural characteistics, biochemical reactions and reverse CAMP test Animal pathogenicity: To determine the toxigenicity of the strain Prophylaxis: Surgery: all damaged tissue should be removed promptly and wound is irrigated with antiseptic solution Antibiotics: metronidazole, penicillin, tetracycline etc Antitoxin: passive immunisation by anti-gas gangrene serum Clostridium botulinum Causes a severe form of food poisoning named botulism Widely distributed saprophyte, found in soil, animal manure, vegetables, sea mud Morphology: Gram positive, non-capsulated bacilli, motile Sub-terminal, oval bulging spores Culture: Obligate anaerobe Blood agar, cooked meat broth at 350 C under anaerobic atmosphere Hemolysis around colonies in blood agar Resistance: Spores are resistant and can withstand heat for several hours at 1000C and for up to 10 minutes at 1200C Classification; Eight types based on antigenically distinct toxins Types A, B, C1, C2, D, E, F and G Toxin: Powerful exotoxin Differs from other exotoxins in that it is not released during the life of bacterium Produced intracellularly and is released on autolysis of the cell Synthesised as non-toxic protoxin which is converted to active toxin by trypsin, other proteolytic enzymes Action: neurotoxin, acts slowly, takes several hours to kill Type A toxin is the most potent Preformed toxin in food is destroyed by boiling for 20 minutes Is a good antigen and can be neutralised specifically by its antitoxin The toxin acts by blocking the production or release of acetylcholine at synapses and neuromuscular junctions Death occurs due to respiratory failure Botulism Etiology : Clostridium botulinum Pathogenicity is due to the action of preformed toxin Botulism is of 3 types: 1. Foodborne botulism 2. Infant botulism 3. Wound botulism 1. Foodborne botulism: Due to preformed toxin in food contaminated with Cl.botulinum Types A,B,E are usually associated with human disease, rarely types C,F and G Source of infection: preserved foods- meat, fish, vegetables Contaminated food usually shows signs of spoilage Cans with preserved food may be inflated and show bubbles on opening There may be no alteration in taste 2. Infant botulism: Seen in infants below 6 months Disease due to ingestion of food contaminated by spores of Cl.botulinum Source of infection: honey S/S : constipation, poor feeding, weakness, lethargy, pooled oral secretions, weak or altered cry, floppiness and loss of head control, respiratory complications “floppy baby syndrome” Patient excretes toxin and spores in faeces Severity- mild illness to fatal disease 3. Wound botulism: Rare condition Wound infection by Cl.botulinum Toxin produced is absorbed into blood Symptoms similar to foodborne botulism except for gastrointestinal components Type A is more common Laboratory diagnosis: Confirmation of clinical diagnosis by demonstration of the bacillus or the toxin in faeces or left over food 1. Microscopy: Gram’s staining shows Gram positive sporing bacilli 2.Culture: Blood agar, RCM 3. Demonstration of toxin: Animal testing Prophylaxis: Proper canning and preservation of food By the time symptoms develop, toxin is fixed to nervous tissue and it can no longer be inactivated by antitoxin Intensive supportive therapy, maintenance of respiration needed Prophylactic dose of antitoxin is given to all others who have consumed the food which was the source of infection Immunisation: 2 doses of toxoid given at an interval of 10 weeks followed by booster after a year Can be used for lab workers exposed to risk Clostridium difficle Morphology: Long, slender, Gram positive bacillus with oval and terminal spores Toxins: Produces 2 toxins, an enterotoxin (toxin A) and a cytotoxin (toxin B) Enterotoxin is responsible for diarrhoea and cytotoxin produces cytopathogenic effects Pathogenesis: Causes antibiotic associated colitis / pseudomembranous colitis Patients on long term oral antibiotic therapy can go in for acute colitis with or without membrane formation Lincomycin and clindamycin are particularly prone to cause pseudomembranous colitis Active multiplication of Cl.difficle and the production of enterotoxin and cytotoxin causes antibiotic associated colitis If the condition is not recognised early and properly treated, it can be fatal Laboratory diagnosis: 1. Isolation of bacilli: From the faeces of the patient Cycloserine-cefoxitin-fructose agar (CCFA) is a selective medium for primary isolation of Cl.difficle 2. demonstration of toxin: Toxin can be demonstrated in the faeces by its effect on human diploid cells and Hep-2 cells, ELISA Treatment: Metronidazole Clindamycin and lincomycin should be avoided