Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
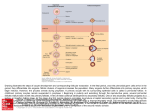
Hum. Reprod. Advance Access published January 27, 2009 Human Reproduction, Vol.1, No.1 pp. 1– 5, 2009 doi:10.1093/humrep/den497 CASE REPORT Reproductive endocrinology Evidence of ‘genuine empty follicles’ in follicular aspirate: a case report† N. Desai 1, C. Austin, F. AbdelHafez, J. Goldfarb, and T. Falcone Cleveland Clinic Foundation, Department of OB/GYN, 26900 Cedar Road, Beachwood, OH, 44122, USA 1 Correspondence address. Tel: þ216-839-3150; Fax: þ216 839-3180; E-mail: [email protected] Failure to retrieve oocytes after normal ovarian stimulation has been labeled ‘empty follicle syndrome’ (EFS). The existence of genuine EFS has been questioned and is still controversial. Here, we report an unusual case in which an extraordinary number of empty follicle-like structures were identified in the ovarian aspirate at the time of retrieval. A 31-year-old woman presented with a 4-year history of primary infertility and underwent ovulation induction. The patient was given hCG and oocyte retrieval was performed 36 h later. During the oocyte retrieval, more than 200 tiny structures resembling pre-antral follicles were noted in the ovarian aspirate. They exhibited two to three layers of granulosa cells and appeared to enclose an immature oocyte. They showed a great variation in size ranging between 40 and 80 mm. These structures were further characterized by electron microscopy and cultivated in vitro to assess hormone secretion. The follicles were found to be devoid of oocytes, but each had a readily identifiable zona. Hormone assays revealed that these follicles were secreting increasing levels of estradiol. A second in vitro fertilization attempt gave similar results. These data are suggestive of some failure in the oocyte maturation process. We speculate that this may be the first actual evidence to support the existence of true empty follicles, which if left to grow in vivo might lead to empty graffian follicles and genuine EFS. Key words: empty follicle syndrome / ovulatory dysfunction / in vitro fertilization / zona pellucida Introduction Failure to retrieve oocytes after normal ovarian stimulation has been labeled ‘empty follicle syndrome’ (EFS). It was described for the first time by Coulam et al. (1986). Incidence of EFS ranges from ,1 (Awonuga et al., 1998) to 7% (Bartfai et al., 1987). This syndrome is not well characterized and its cause remains controversial. Although rare, failure of oocyte retrieval is very stressful for both the patient and the physician. Three main causes have been suggested for the pathogenesis of this syndrome: ovarian dysfunction, iatrogenic causes and technical causes. Iatrogenic causes may be due to the use of inappropriate batches, dosing or timing of hCG which is injected for the final steps of maturation (reviewed in Bustillo (2004)). Some investigators question the existence of ‘genuine EFS’ and prefer to call it unsuccessful oocyte retrieval as they believe that iatrogenic and technical causes are responsible in almost all cases of EFS (Aktas et al., 2005). The term ‘borderline form of EFS’ has been applied to describe cases where very few mature or immature oocytes are retrieved from the aspiration of several follicles after a satisfactory ovarian stimulation regimen (Isik and Vicdan, 2000; Nikolettos et al., 2004). Here, we report a case of a patient undergoing routine in vitro fertilization (IVF) retrieval who had an extraordinary number of empty folliclelike structures in her follicular aspirate. In a subsequent IVF cycle, these empty follicles were once again observed. This may be the first documentation of ‘true empty follicles’ at their earliest developmental stage. Case report The patient is a nulligravida woman who presented at an age of 29 with a 4-year history of infertility. Her menstrual cycles were regular: 26 –28 days in length. She described her periods as 7 days long, heavy, with moderate dysmenorrhea. She was on no medications and had no history of prior abdominal surgery. Hysterosalpingogram (HSG) revealed bilateral fill and spill of the fallopian tubes, but the fundus had a concave shape suggestive of an extrinsic pressure effect. Ultrasound confirmed multiple uterine fibroids including a large posterior one measuring 51 46 mm. The patient was treated empirically with two cycles of clomid with intrauterine insemination before undergoing an abdominal myomectomy. Following her surgery, the couple attempted to conceive without treatment for approximately six cycles. When she returned to resume treatment, a repeat HSG was performed revealing a normal uterine cavity, fill and spill of the left fallopian tube, but only partial filling of the right tube. She completed one more cycle of clomid with insemination. †Presented in part at the 64th annual meeting of the American Society for Reproductive Medicine, 8–12 November 2008, San Francisco, CA, USA. & The Author 2009. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: [email protected] 2 Desai et al. The couple then decided to change their treatment to IVF. The patient was 31 at the time of her first IVF attempt. Ovarian stimulation was carried out using the long luteal phase Lupron protocol with 200 U of recombinant FSH for 10 days. The peak estradiol level on Day 11 was 1779 pg/ml. Seven follicles were documented by ultrasound, measuring 17–20.5 mm average diameter. The patient was given hCG (Ovidrel) on the evening of Day 11, and oocyte retrieval was scheduled 36 h later. Transvaginal ultrasound-guided follicular aspiration was performed using a standard double lumen needle. The process of oocyte retrieval was uneventful and 14 oocytes were recovered. Only three oocytes were mature and two were fertilized after intracytoplasmic sperm injection. The embryos were transferred to the patient’s uterus on Day 3 at the 7–9-cell stage. What was striking about this case was that during the oocyte retrieval, the embryologist noted 20–30 tiny follicle-like structures in each tube of follicular aspirate. These structures were examined at 300 magnification using an inverted microscope (Fig. 1). The follicles showed a great variation in size, ranging from 40 to 80 mm in diameter. They appeared to have an intact thecal layer and a zona. We did notice that the central region with the ‘oocyte’ appeared a little odd: it was smooth with a clear appearance. The pooled aspirates contained over 200 of these pre-antral follicles. Convinced that these were indeed primary and secondary follicles, we placed some follicles in in-vitro maturation medium (IVM) medium, vitrified some for future studies and fixed some for transmission electron microscopy. The IVM medium was minimum essential medium with 1% protein supplemented with insulin (10 mg/ml) and FSH (100.5 mIU/ml). The follicles attached to the culture surface within 24 h of plating. Granulosa cell (GC) proliferation was demonstrated by an increase in diameter of plated follicles. An hormone profile revealed increasing levels of estradiol secretion starting from 152 (8 pg/follicle plated) to 1462 pg/ml (or 77 pg per follicle) after 13 days of culture. Progesterone was not detected in the follicle culture supernatants. We examined few follicles after just 24 h of in vitro culture. Follicles were treated with hyaluronidase to remove cumulus cells and to determine nuclear status of the oocyte. Interestingly, all of the follicles examined were determined to be devoid of an oocyte; yet there was clear evidence of a very thin zona pellucida (Fig. 2). This was later corroborated by the electron microscopy studies (Fig. 3). The patient did not become pregnant and underwent a second IVF cycle. In light of the poor yield of mature oocytes and the bizarre, unexplained presence of so many pre-antral -like follicles in her first cycle, a different IVF stimulation regimen was attempted. Luteinizing hormone (LH) was added to the stimulation protocol, the follicles were allowed to grow to a larger diameter before administration of hCG and the retrieval was scheduled for 38 h after hCG rather than 36 h, which is our standard practice. The patient was down-regulated with Lupron and stimulated with 225 U of recombinant FSH and 75 U of recombinant LH for 11 days. Her peak estradiol level was 1794 pg/ml on Day 11. On an ultrasound scan, seven follicles were seen and measured 19–22 mm in diameter. We retrieved nine oocytes; six were mature and injected with husband’s sperm. Four of these oocytes were fertilized. Two embryos were transferred at the seven and five cell stage and none were frozen. Again, the patient did not become pregnant. Figure 1 Photomicrographs of follicle-like structures observed at the time of oocyte retrieval. Over 200 or more structures were recovered from the ovarian aspirates. A wide range of sizes were observed; they ranged from 40 to 80 mm in diameter. 3 Evidence of empty follicles Figure 2 The follicle-like structures after treatment with hyaluronidase to remove GCs. Structures were devoid of oocytes but thin zonae were clearly visualized. Figure 3 Transmission electron micrographs of follicle-like structures. (A) Follicle-like structure composed of GCs but no oocyte (800). (B) Inset magnified showing cytoplasmic organelles within a GC; MV: microvilli; ER: endoplasmic reticulum; M: mitochondria (22 000). Once again follicle-like structures were observed in the follicular aspirate, although in far lower numbers than in the first cycle, possibly due to the changes in the stimulation protocol. This time the ‘follicle-like’ structures were treated with hyaluronidase and assessed immediately upon recovery for the presence of an oocyte. Once again, no oocytes could be identified within these structures. 4 There was also no evidence of a degenerate oocyte. The unusual findings with this patient are being further investigated. This investigation on the discarded follicle-like structures found at the time of oocyte retrieval was conducted in accordance with the policies of the Cleveland Clinic Institutional Review Board. Discussion EFS remains a controversial topic, with many scientists questioning its actual existence. The term was first used to describe the absence of oocytes after IVF oocyte retrieval from a patient who responded normally to follicular stimulation with rising estradiol levels and increasing follicular diameters as measured by ultrasound (Coulam et al., 1986). Although dysfunctional folliculogenesis has been offered as an explanation, there is little direct evidence to explain the etiology of this event. Other explanations offered for the absence of oocytes have included technical difficulties during the retrieval, premature LH surge and pharmacological problems related to the lack of bioactive product in the hCG injection (reviewed in Bustillo (2004)). This case report may be the first direct evidence of the existence of true EFS as a symptom of ovarian dysfunction. These follicle-like structures must have been prevalent in the ovarian cortex of this patient. Upon piercing of the ovary to aspirate mature follicles, these tiny structures were simultaneously aspirated. The presence of close to 200 pre-antral follicles in the aspirate, the presence of thin zonae and the clear lack of oocytes are suggestive of some failure in the oocyte maturation process. It has been previously theorized that the absence of oocytes in EFS may be attributed to increased apoptotic gene expression and a reduction in transcripts whose products are responsible for healthy follicular growth. Without proper signaling, it is postulated that the oocyte may undergo atresia (Inan et al., 2006). This may explain our current findings. The recurrence of these same follicle-like structures in the patient’s second IVF attempt lends credence to the idea of genuine ovarian dysfunction rather than technical or pharmacological artifact. The in vitroplated follicles were clearly capable of growth expansion and increasing levels of estradiol secretion. Extrapolating from these data and observations, one might hypothesize that the continued growth within the ovary of such follicles in the absence of a viable oocyte would ultimately result in what presents as EFS. There have been other reports of primary and secondary follicles being isolated from follicular aspirate, along with mature oocytes after ovarian stimulation (Wu et al., 1998; Moskovtsev et al., 2002; Zhang et al., 2002). However, all of these studies claim the presence of an oocyte at the time of isolation and suggest that degeneration occurred later, after in vitro culture for 48 h due to suboptimal culture conditions. Our case was unique in that we found no evidence of an oocyte even on the initial day of recovery. The present case may be a borderline form of EFS since some oocytes were retrieved but the number of mature ones was very low. In EFS, the absence of oocytes may be attributed to increased apoptosis and reduced healthy follicular growth (Inan et al., 2006). Thus, the oocyte may have been originally present and then underwent atresia and apoptosis. It is still a matter of debate, especially in humans, as to whether the oocyte alone (Bousquet et al., 1981; Epifano et al., 1995) or Desai et al. in conjunction with GCs (Lee and Dunbar, 1993; Hinsch et al., 1994; Sinowatz et al., 2001; Bogner et al., 2004; Gook et al., 2004) can express and deposit the proteins needed to form the zona. Eberspaecher et al. (2001) concluded that in mice, monkey and humans, the zona proteins are expressed and assembled exclusively by the oocyte and not by the GCs. They suggested that the previous observations that showed the involvement of GCs in zona pellucida formation may be due to improper fixation of tissues leading to disruption of zona pellucida. If this is correct, the presence of a thin zona in the retrieved follicle-like structures in our present case study may be a further proof of the ovulatory dysfunction theory, in the sense that the oocyte may have been present and then undergone atresia after the formation of a zona pellucida. In summary, we report here a case of borderline EFS where ovulatory dysfunction seems to be the main cause for its pathogenesis. To the best of our knowledge this is the first clear evidence of true empty follicles, which we believe that, if left to grow in vivo, would have resulted in empty Graffian follicles and genuine EFS. References Aktas M, Beckers NG, van Inzen WG, Verhoeff A, de Jong D. Oocytes in the empty follicle: a controversial syndrome. Fertil Steril 2005; 84:1643 – 1648. Awonuga A, Govindbhai J, Zierke S, Schnauffer K. Continuing the debate on empty follicle syndrome: can it be associated with normal bioavailability of b-human chorionic gonadotrophin on the day of oocyte recovery? Hum Reprod 1998;13:1281 – 1284. Bartfai G, Feinman M, Barad G. Empty follicle syndrome. Fertil Steril 1987; 47:1040. Bogner K, Hinsch KD, Nayudu P, Konrad L, Cassara C, Hinsch E. Localization and synthesis of zona pellucida proteins in the marmoset monkey (Callithrix jacchus) ovary. Mol Hum Reprod 2004; 10:481 – 488. Bousquet D, Leveille MC, Roberts KD, Chapdelaine A, Bleau G. The cellular origin of the zona pellucida antigen in the human and hamster. J Exp Zool 1981;215:215 – 218. Bustillo M. Unsuccessful oocyte retrieval: technical artefact or genuine ‘empty follicle syndrome’? Reprod Biomed Online 2004;8:59– 67. Coulam CB, Bustillo M, Schulman JD. Empty follicle syndrome. Fertil Steril 1986;46:1153 – 1155. Eberspaecher U, Becker A, Bringmann P, van der Merwe L, Donner P. Immunohistochemical localization of zona pellucida proteins ZPA, ZPB and ZPC in human, cynomolgus monkey and mouse ovaries. Cell Tissue Res 2001;303:277– 287. Epifano O, Liang LF, Familari M, Moos MC Jr, Dean J. Coordinate expression of the three zona pellucida genes during mouse oogenesis. Development 1995;121:1947 – 1956. Gook D, Matric M, Borg J, Edgar D. Identification of zona pellucida proteins during human folliculogenesis. Hum Reprod 2004;19(Suppl. 1):140. Hinsch KD, Hinsch E, Meinecke B, Topfer-Petersen E, Pfisterer S, Schill WB. Identification of mouse ZP3 protein in mammalian oocytes with antisera against synthetic ZP3 peptides. Biol Reprod 1994; 51:193 – 204. Inan MS, Al-Hassan S, Ozand P, Coskun S. Transcriptional profiling of granulosa cells from a patient with recurrent empty follicle syndrome. Reprod Biomed Online 2006;13:481 – 491. Evidence of empty follicles Isik AZ, Vicdan K. Borderline form of empty follicle syndrome: is it really an entity? Eur J Obstet Gynecol Reprod Biol 2000;88:213 –215. Lee VH, Dunbar BS. Developmental expression of the rabbit 55-kDa zona pellucida protein and messenger RNA in ovarian follicles. Dev Biol 1993; 155:371–382. Moskovtsev SI, Griffin JT, Peterson CM, Carrell DT. Primordial and pre-antral follicles are not commonly observed in IVF aspirates. Hum Reprod 2002;17:1783–1787. Nikolettos N, Asimakopoulos B, Simopoulou M, Al-Hasani S. A borderline form of empty follicle syndrome. Case report. Clin Exp Obstet Gynecol 2004;31:79 –80. 5 Sinowatz F, Topfer-Petersen E, Kolle S, Palma G. Functional morphology of the zona pellucida. Anat Histol Embryol 2001;30:257– 263. Wu J, Zhang L, Liu P. A new source of human oocytes: preliminary report on the identification and maturation of human preantral follicles from follicular aspirates. Hum Reprod 1998;13:2561– 2563. Zhang P, Hreinsson JG, Telfer E, Hovatta O. Few instead of many: human follicle collection from follicular aspirates at oocyte retrieval. Hum Reprod 2002;17:3190– 3192. Submitted on November 25, 2008; resubmitted on December 17, 2008; accepted on December 28, 2008