Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
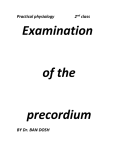
LABORATORY HANDBOOK HEART SOUNDS & BLOOD PRESSURE For the course Systems Biology Karolinska Institutet • Department of Physiology and Pharmacology • Physiology Education Postal address: 171 77 Stockholm Visiting address: Von Eulers väg 4a, plan 2 Tel exp: 08-524 872 29 • Tel vx: 08-524 864 00 • Fax: 08-524 872 31 Heart Sounds and Blood Pressure Introduction The following laboratory exercise will be an introduction to auscultation of the heart, palpatory and auscultatory blood pressure measurement, and blood pressure regulation during orthostatic challenge. Goals Heart sounds • Identify the first and second heart sounds during auscultation. • Locate where on the chest the different parts of the heart is best heard. • Auscultatory define systole and diastole. • Know the mechanisms behind the heart sounds. Blood pressure • Perform palpatory and auscultatory blood pressure measurements. • Understand the relationship between the Korotkoff sounds and systolic and diastolic pressure during auscultatory measurements. • Identify factors that affect the systolic and diastolic blood pressure. • Identify factors and sources of error that can affect a blood pressure measurement. Orthostatic test • Perform a simple orthostatic test. • Interpret a complete orthostatic test. • Understand how circulation is affected by standing up quickly, and how the body compensates for this. • Account for the symptoms that occur during orthostatic hypotension. • Understand the mechanism behind vasavagal syncope (fainting). Human Physiology Heart Sounds and Blood Pressure 1 BACKGROUND Auscultation of the heart When the heart beats, vibrations are set up in the heart and the major blood vessels. These vibrations are caused by the acceleration or deceleration of the blood, when the kinetic energy is converted into sound energy. Furthermore, the extent of vibrations depend upon turbulent flow which in turn is a function of the velocity and viscosity of the blood. The heart sounds can be divided into: Heart sounds (normal and extra) Accessory sounds (murmurs and friction rubs) Heart sounds The heart sounds are normally dependent on ventricular function. The primary origin of the sounds is the turbulence that occurs due to closing of the valves. The first heart sound (“lub”) occurs upon closure of the mitral and tricuspid valves. The second heart sound (“dub”) arises from the shutting of the aortic and pulmonary valves. The third heart sound is heard when the blood flows rapidly from the atria into the ventricles. It is predominantly heard in children and young, well-trained individuals. The fourth heart sound occurs during atrial contraction. It is considered to be pathological in all except infants and young children. The first sound marks the beginning of systole and diastole starts with the second sound. Accessory Heart Sounds An accessory heart sound that is strong enough to be palpated is called fremitus (fremissement in Swedish). If the mouth of a valve is too narrow, this is called a stenosis. A stenosis can cause a murmur because of the resulting turbulent flow. Note also that an increased amount of blood trying to get through a normal sized valve (e.g. during exercise) can also cause a murmur. The most common sites for stenosis is the mitral or aortic valve. An insufficiency arises when the a valve cannot shut tightly. An insufficiency can give rise to a murmur because of altered flow. An insufficiency in the atrioventricular valves (tricuspid and mitral valves), and a stenosis in the semilunar valves (aortic and pulmonary valves) demonstrates itself during systole. The opposite is true during diastole (insufficiency is heard in the semilunar valves and a stenosis in the atrioventricular valves). These conditions can be congenital or acquired. Human Physiology Heart Sounds and Blood Pressure 2 In the case of young, well-trained individuals, a soft murmur can be heard clearly during inspiration (increased venous return) and is most easily heard in the third left intercostal space (I3) at the sternal border. There is a characteristic area (the point of maximal impulse, PM ) where heart sounds or murmurs can be best heard. Unfortunately, this area can vary from person to person. In different illnesses, there will usually be a characteristic shift in the PM. Figure 1 The sound from different valves can best be heard in different locations on the chest. Note that the sound can project to different sites without being pathological. This is especially true in the case of the aortic and pulmonary components. (Lännergren et al. Fysiologi, 1996). Human Physiology Heart Sounds and Blood Pressure 3 Valve is Closed Open Closed Fig. 2 ECG-registration Valves Tricuspid Pulmonary Mitral Aortic Heart sounds Heartcycle Diastole “LUB” Systole “DUB” Diastole The Stethoscope The stethoscope has two possible modes of use. Low-pitched sounds are best heard with the bell side and high-pitched sounds with the flat diaphragm. Use the diaphragm side for blood pressure measurements. Make sure that the earpieces are set properly in your ears, they should point forwards and downwards in the same direction as the external ear canals to get the best sound quality. Human Physiology Heart Sounds and Blood Pressure 4 Blood Pressure The blood pressure is regulated continuously for each tissue to get enough blood flow and to keep the arterial pressure relatively constant. There are two main factors that regulate the arterial pressure; cardiac output and peripheral resistance. These are responsible for short term regulation of blood pressure. The total amount of fluid in the body will also affect the blood pressure over a longer period of time. The true value of blood pressure in the arterial system must be measured by inserting a catheter into a blood vessel. However, the method is not sufficiently easy and risk-free to be used except in exceptional cases such as research and intensive care. The most satisfactory method is the auscultatory method where one listens to the altered sound caused by changes blood flow in the blood vessels. The blood pressure is measured by using a blood pressure cuff to compress a large artery, usually in the upper arm. The palpatory method is able to provide a good estimate of the systolic pressure. Systolic-, diastolic-, pulse- and mean arterial pressure. The systolic pressure is produced by the pumping of blood from the heart into the arterial system. The stroke volume and the volume of blood that is already present in the arterial system are the determining factors for the amplitude of the pressure. A stiff blood vessel causes a considerably larger increase in systolic blood pressure than does an elastic blood vessel. The normal range is 90 to 140 mm Hg. The diastolic pressure is the lowest pressure that exists in the arterial system during the heart’s diastolic, or filling, phase. The blood pressure falls continuously because of the peripheral outflow of blood. Consequently a low heart rate increases the tendency for a low diastolic pressure because more blood leaves the aorta during the longer time between heartbeats. The diastolic pressure is also affected by the peripheral resistance; vasoconstriction causes an increase in the diastolic pressure. The normal range is 65 to 90 mm Hg. Repeated values of diastolic pressure over 90 mm Hg are considered to be indicative of hypertension. The typical normal or textbook value of systolic/diastolic blood pressure is 120/80, expressed verbally as 120 over 80. The pulse pressure is the difference between the systolic and diastolic pressure. The higher the pulse pressure, the larger pulsations in the vessels. During the ejection phase, the blood pressure increases in the aorta (to the systolic pressure) and the elastic walls are stretched. A pressure equalisation then occurs with the resultant pulse wave continuing in a peripheral direction. This pulse wave moves more rapidly than the blood flows (3 –10 m/s compared to less than 0.5 m/s). The pulse wave represents the movement of the pressure increase through the circulation system. The mean arterial pressure is of great importance for flow and transcapillary exchange. It is calculated as the sum of the diastolic pressure plus 1/3 of the pulse pressure. Human Physiology Heart Sounds and Blood Pressure 5 Auscultatory method of measuring blood pressure The figure below shows how the Korotkoff sounds are believed to develop. Fig 3 The principle of auscultatory measurement of blood pressure in the arm.. (Jonson et al. Klinisk fysiologi. 1998). When the pressure in the cuff is greater than the systolic pressure (A), there is no flow in the blood vessel and no sound is heard. If one reduces the pressure just below the systolic pressure (B), a turbulent flow starts (phase I). The flow of blood increases progressively as the pressure in the cuff falls (phase II, characterised by a roaring sound and phase III, this becomes more and more clear). When the cuff pressure is equal to the diastolic pressure (C), the Korotkoff sound disappears (phase IV) because the blood vessel is no longer compressed. Phase V is when the sound disappears completely. There are variations on this usual course of events. The most common is that the sound only subsides slowly. The standard procedure is then to accept the pressure at which the reduction in sound occurs as the diastolic pressure. If the difference between phases IV and V is less than 10 mm Hg, one should note both values (120/80-90). In certain cases, an auscultatory gap can exist. This is when all sound disappears from an interval between the systolic and diastolic pressures. The reason for this is unknown, but you should keep listening and slowly release pressure a short while after the diastolic sound has disappeared not to get a false high diastolic value due to the auscultatory gap. Note! If the diaphragm of the stethoscope is placed over the brachial artery without the cuff being inflated, there should be no sound. If a sound is heard this is due to a compression of the artery by the stethoscope resulting in turbulent flow. Human Physiology Heart Sounds and Blood Pressure 6 Sources of error Resting pressure: Somebody who is not relaxed can have a very variable blood pressure. Therefore, one should always try to measure the resting blood pressure as a lowest value. A person who is moving or not relaxed will get an inaccurately high measurement due to the cuff having to work against the muscle tone as well as static contractions giving a significant increase in blood pressure. Everything that activates the sympathetic nervous system can result in false highs; nervousness, pain, need to go to the bathroom, fear of the situation at the hospital or lab. Characteristics of the artery: If the blood vessels are stiff, much greater cuff pressure is needed to compress them. Because of this, the cuff pressure might be increased insufficiently and the systolic pressure will not be obtained. Limb position: The limb in which one measures the blood pressure must be at the same level as the heart. This avoids addition of a hydrostatic component to the blood pressure (Note, that the force of gravity acting on the limb and the heart is then the same!). This means that when the subject is laying down, the arm should be at the same level as half of the thoracic height. Cuff error: The pressure in the cuff is not transmitted perpendicular through the tissue to compress the blood vessel but is dissipated through the cuff and the highest pressure is in the middle of the cuff. A cuff that is too small or poorly placed on the arm will not dissipate properly. The result is that one can get a too high, false, measure of the blood pressure. The width of the cuff should be at least 30% of that of the limb. The stethoscope. The placement of the stethoscope can be a source of error during the blood pressure measurement. The sound will not be clear if the stethoscope is not placed directly above the artery. If too much pressure is applied, the artery can be compressed leading to turbulent flow. Inaccurate inflation. The pressure in the cuff should be decreased with the correct speed. If it is lowered too quickly, the heart beats will not be heard often enough and the inaccuracy will be great. The result tends to be too low (the heart should have time to beat at least once/3mmHg). A value that is too high is possible with a slow inflation or deflation if this leads to stasis on the venous side. Sphygmomanometer. The sphygmomanometer should work and be calibrated. Human Physiology Heart Sounds and Blood Pressure 7 a) The dashed lines represent the distribution of pressure under the cuff. b) The correlation between the pressure in the cuff and the character of the auscultated sound. Fig. 4 Lännergren et al. Fysiologi, 1996 Human Physiology Heart Sounds and Blood Pressure 8 Orthostatic test The principle behind the orthostatic (ortho = straight or upright, static = position) test is to register blood pressure and heart rate while the subject is in a horizontal and vertical position. Due to the effect of gravity on the blood volume, a person in a supine or lying position has a central reservoir of blood in the lungs and heart. Between 400 to 700 ml is redistributed when one rises from a supine position. In addition to the redistribution of blood from the lungs to the legs, there is also a change in the perfusion of the lung so that the upper parts get a lower perfusion. The reduced central blood volume leads to a reduced venous return which in turn leads to a reduced stroke volume. A reduction in stroke volume results in lowered arterial blood pressure. This is detected by the baroreceptors in the aortic arch and carotid sinus. The baroreceptors in the carotid sinus register a lower blood pressure than that generated by the heart since they are located approximately 30 cm above the heart in an upright position. In addition, it is thought that “low-pressure receptors” in the atrium and the large veins respond to the reduced central blood volume with an increased afferent discharge. The afferent signals from the different receptors leads to increased sympathetic activity from the vasomotor centre. The peripheral resistance increases and the heart rate increases to maintain the mean arterial pressure. The increased sympathetic tone affects the capacitance blood vessels and leads to an increased venous return. In the long run, there are also humoral compensation mechanisms. Secretion of antidiuretic hormone (ADH or vasopressin) from the neurohypophysis increases. In addition, the renin activity increases which acts via angiotensin (increases peripheral resistance) to increase aldosterone secretion from the adrenal glands and thereby increase the re-absorption of Na+ and water in the kidneys. Fig 5. Response of some haemodynamic parameters in a normal person in response to a change in position (After Bevegård, 19973). The blood pressure is measure at the level of the heart. STROKE VOLUME HEART RATE CARDIAC OUTPUT PERIPHERAL RESISTANCE BLOOD PRESSURE Human Physiology Heart Sounds and Blood Pressure 9 Certain people have difficulties making the adjustment from a supine to a standing position, and develop orthostatic hypotension. When these individuals get up quickly, they feel lightheaded. In more severe situations, people faint returning them to a horizontal position and blood circulation to the brain is restored. Asympathetic orthostatic hypotension describes a situation when the mechanisms for compensating for the decreased blood pressure that occurs when changing position from supine to standing not are enough and in some cases there is no increase in heart rate. This can be seen in elderly individuals as a result of treatment with pharmaceutical agents that block the sympathetic system, or it can be caused by damage to the autonomic nervous system (such as in diabetes and Parkinson’s disease) or the blood pressure regulating area in the medulla oblongata (for example following a myocardial infarction). Sympathetic orthostatic hypotension refers to an increased sympathetic tone or discharge which fails to maintain blood pressure at an appropriate level. There are two possible reasons for this; an inadequate effect of the sympathetic nerves on the blood vessels and/ or a reduced blood volume. Sympathetic orthostatic hypotension usually appears when the blood volume is reduced, such as after a large haemorrhage or bleeding over a longer time when a reduced renin activity leads to a decreased plasma volume. Tall individuals are affected to a greater extent by the effects of gravity and are thus more likely to be affected than short individuals. Training increases blood volume and also improves sympathetic function. In more severe cases, where physical training is not sufficient, one can use pharmaceutical agents that increase the tone of the capacitive blood vessels. Fig 6. Diagram of some of the compensation mechanisms that help to maintain blood pressure in a standing person (after Thulesius, 1970. Human Physiology Heart Sounds and Blood Pressure 10 Clinical use of the tilt bed Orthostatic test Investigation of the causes of syncope (fainting), dizziness and sensation of sickness that occur upon changes in posture. Rehabilitation Patients who have been bedridden for a long time can be trained to regain their orthostatic reflexes by means of the tilt bed. In this way, the renin activity can be increased stepwise and sympathetic function will be improved. Simple Orthostatic test A simple test of orthostatic function can be done during a routine measurement of blood pressure. Once the blood pressure has been measured at rest, the subject will stand up and heart rate and blood pressure will be measured immediately and after 2 minutes. Comprehensive Orthostatic test This is undertaken with a tilt bed to avoid the involvement of the muscle pump (activation of the muscle pump in the legs during movement will facilitate the venous return to the heart). It easier to control the speed of standing up, but this is a less “physiological” test. Heart rate and blood pressure are measured at rest and then every minute for 7 minutes after tilting the subject. In certain cases, a continuous record of ECG is also taken to study the sympathetic activity. Change in heart rate I III Normal range Fig 7 II Human Physiology Change in blood pressure Heart Sounds and Blood Pressure 11 Interpretation A change in blood pressure from the resting value is marked along the x-axis. The change in heart rate from the resting value is marked along the y-axis. The co-ordinate values (x,y) for the seven time points obtained after tilting the subject are plotted. In a normal subject, these values have returned to the normal range of resting values within 7 minutes. In the Figure above, this is marked as the “normal range”. A final value that ends up in the area marked “I” shows that the blood pressure fell despite a rise in heart rate and is indicative of sympathetic orthostatic hypotension. If the values end up in the area marked “II”, this indicates that there was no rise in heart rate when the blood pressure fell i.e. asympathetic orthostatic hypotension. Over-compensation by the sympathetic system leads to increased heart and elevated blood pressure (III). Such a response may be an early symptom of hypertension. Vasovagal reaction Either a reduced sympathetic tone or an increased parasympathetic tone (for example in very stressful situations, a decrease in central blood volume or venous return) can result in a decrease in heart rate and a fall in blood pressure and a risk of fainting. Fainting or syncope is often preceded by a vasovagal reflex in combination with dizziness, nausea, pallor and bradycardia. Human Physiology Heart Sounds and Blood Pressure 12 PROCEDURE – Auscultation of the Heart Be organised and focussed when you listen. Use an onomatopoetic chorus to describe the rhythm (for example lub-dub lub-dub lub-dub etc). Organisation Ideally, this laboratory procedure should be done in a QUIET room. Adjust your stethoscope so that you can hear well. Listen to one valve at a time. Begin by trying to identify the first heart sound. In every examination, begin by listening to the rhythm. Auscultate the first heart sound. Then auscultate the second heart sound. Finally listen for possible systolic or diastolic murmurs. Work in pairs. Be methodical. Follow the instructions below. 1. The subject should strip to the waist and lie comfortably on the examination table. The examiner should stand on the subject’s right side. 2. Palpate or feel where the heartbeat is strongest, this is the point of maximal impulse (PM). Mark that point on the chest. Is its rhythm regular? _____ Frequency: _____ beats/min 3. Palpate the radial pulse. Frequency: _____beats/min. A deficit is said to exist when the pulse is lower than the frequency of the heart. Is there a deficit? Yes ( ) No ( ). 4. Place the stethoscope over the third left intercostal space near the sternal border. Make yourself familiar with the rhythm. Try to determine the systolic and diastolic phases. 5. Listen to: a. The first heart sound b. The second heart sound c. The interval between the first and second heart sounds. Can you hear a systolic murmur? d. The interval between the second and first heart sounds. Can you hear a diastolic murmur? 6. Make you subject take a long and deep inspiration. Focus on the second heart sound, can you hear a split in the sound? Human Physiology Heart Sounds and Blood Pressure 13 7. Move the stethoscope over the chest and note where you best hear the following heart sounds. a. The first heart sound: _____ b. The second heart sound: _____ c. Identified murmur: _____ 8. Make your subject do a little intensive exercise, such as push-ups or sit-ups. Listen again to the heart. Now do you hear any murmurs? Yes ( ) No ( ) If yes, when? Systole ( ) Diastole ( ) Best area to hear this murmur The following is an example of how one can describe the heart sounds. “Regular rhythm with a heart rate of 80 beats/min. Normal heart sounds. Mid-systolic high-pitched murmur grade 3-4 can be heard in the second right intercostal space. Additional questions – auscultation of the heart These questions are only for your assistance and can be used as a tool to see if you have understood the background and practical work during this exercise. If you chose to answer them, you can ask your instructor for help. 1. When you now have performed the lab, can you identify the first and second heart sounds? 2. Was there a third and fourth sound? 3. Were you able to identify a split in the second sound induced by breathing? What is the mechanism behind this split? 4. Can you palpate the PM? 5. Do you know where you usually can best hear sounds from different parts of the heart? 6. Can you explain: a. the auscultatory definition of systole and diastole? b. the mechanisms behind the heart sounds? c. sinus arrhythmia? 7. What are the pathological changes that cause the most common murmurs? Human Physiology Heart Sounds and Blood Pressure 14 PROCEDURE – Blood Pressure Work in pairs. Do the measurements in duplicate. Fill in the results that you obtain in the spaces below. 1. Ask the subject to lie on the examination table and relax (ten minutes is the standard, but it is not necessary for this laboratory). Place the upper arm so that the elbow is accessible. 2. While the subject is relaxing, measure the circumference of the upper arm. Select and place a cuff of the right size on the upper arm. Get the stethoscope ready. Palpate the brachial artery at the elbow. Make sure that you know where it is. 3. Palpate the radial pulse and note the frequency (_____/min). Inflate the cuff until the pulse disappears (_____ mm Hg). Increase the pressure a further 20 to 30 mm Hg. What is this pressure called? Continue another 20-30 mmHg. 4. Place the stethoscope over the brachial artery and slowly extend the subject’s elbow. The subject has to be relaxed. Start to slowly deflate the cuff. 5. Remember the pressure at which you hear the first Korotkoff sound (_____ mm Hg) and when the Korotkoff sounds disappear (_____ mm Hg). Deflate the cuff completely. Was there any auscultatory gap? Yes ( ) No ( ) Blood pressure = _____/_____ mm Hg (systolic/diastolic). 6. Check with the laboratory assistant that you have done everything correctly. Swap with your partner and repeat the measurements. Additional questions – blood pressure 1. Do you know how to perform a palpatory and auscultatory blood pressure measurement? 2. How do you correctly chose the width of the cuff for different individuals? 3. What is the relationship between the Korotkoff sounds and the systolic and diastolic blood pressure during auscultatory measurements? 4. Which factors affect the systolic blood pressure? 5. Which factors affect the diastolic blood pressure? 6. Which factors can affect the blood pressure measurement? 7. What is the normal range for systolic and diastolic blood pressure? Human Physiology Heart Sounds and Blood Pressure 15 PROCEDURE – Orthostatic Test IMPORTANT NOTE: If a vasovagal response occurs, end the test immediately. Return the tilt board back to a horizontal position and leave the subject with the legs slightly raised. 1. Choose a volunteer, preferably somebody who is tall and thin. Strap the subject securely in a horizontal position on the tilt board. 2. Assign the following duties: 1 data collator 1 timekeeper 2 heart rate measurers (foot pulse!) 2 blood pressure measurers (one for each arm) 3. Mark where the pulses can be palpated on the front of the foot and at the ankle. Mark also the point where the brachial artery can be best heard. Remember to calculate the heart rate based on a 15 second measurement; since you will not have time to measure it every minute. 4. After the subject has rested for 5-10 minutes, measure the resting blood pressure and heart rate. Next the laboratory assistant tilts the bed and the clock starts. Start measuring heart rate and blood pressure immediately. 5. Measure the heart rate and blood pressure every minute for the next 7 minutes. The data collator checks how the subject feels. 6. After the experiment is finished, tilt he bed back to the original position and release the subject. Mark the data in the table. Go through the results with the laboratory assistant and use the simple plot (Figure 7) to discuss and interpret your results Human Physiology Heart Sounds and Blood Pressure 16 Table 1 Heart rate 1 Heart rate 2 Average heart rate Blood pressure 1 Blood pressure 2 Average blood pressure Rest 0 min 1 min 2 min 3 min 4 min 5 min 6 min 7 min The subjects reactions: _________________________________________________ ____________________________________________________________________ ____________________________________________________________________ Human Physiology Heart Sounds and Blood Pressure 17 Additional questions – orthostatic test 1. How is a simple orthostatic test performed? 2. How do you interpret a comprehensive orthostatic test? 3. How is circulation affected by a quick change in posture from supine to standing? 4. Which mechanisms compensate to maintain blood pressure when standing up quickly? 5. What are the two types of orthostatic hypotension? 6. List a couple of symptoms of orthostatic hypotension. 7. List some reasons for orthostatic hypotension. 8. What is the mechanism behind vasovagal syncope (fainting)? 9. What is the clinical use for the orthostatic test? Human Physiology Heart Sounds and Blood Pressure 18