Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
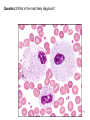
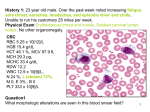
History 1: 23 year old male. Over the past week noted increasing fatigue, sore throat, earaches, headaches, and episodic fever and chills. Unable to run his customary 25 miles per week. Physical Exam Erythematous throat and tonsils. Swollen cervical lymph nodes. No other organomegaly. CBC RBC 5.25 x 10[12]/L HGB 15.4 g/dL HCT 46.1 %, MCV 87.9 fL MCH 29.3 pg, MCHC 33.4 g/dL RDW 12.2 WBC 12.9 x 10[9]/L, N 24 % L (shown) 73%, M 0, E 3% , B 0 PLT 333 x 10[9]/L Question1 What morphologic alterations are seen in this blood smear field? 1 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, Normochromic WBC morphology: Most of the lymphocytes are reactive. They are large cells with a smudged chromatin pattern and abundant cytoplasm with radial and/or peripheral basophilia. Some of the larger cells have finer chromatin and nucleoli. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 2 Answer 2 Further Laboratory Studies: Heterophil antibody screen: positive Question 3: What is the most likely diagnosis? 3 Answer 3 Diagnosis: Infectious mononucleosis Clinical Course Three weeks later, the patient's symptoms had abated, and his WBC count was 7.6 x 10[9]/L, with 56% lymphocytes 4 History 2: 70 year old female. Symptoms of dyspnea on exertion, easy fatigability, and lassitude for past 2 to 3 months. Denied hemoptysis, GI, or vaginal bleeding. Claimed diet was good, but appetite varied. Physical Exam:Other than pallor, no significant physical findings were noted. Occult blood was negative. CBC RBC 3.71 x 10[12]/L HGB 5.9 g/dL HCT 20.9 % MCV 56.2 fL MCH 15.9 pg MCHC 28.3 g/dL RDW 20.2 WBC 5.9 x 10[9]/L N 82 %, L 13% M 1%, E 4%, B 0 PLT 383 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 5 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: 2+ hypochromasia 3+ microcytosis 2+ anisocytosis 2+ elliptocytes and target cells occ teardrops and fragments WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 6 Answer 2 Further Laboratory Studies Iron studies were performed, and results were: serum ferritin <10 ng/mL (RI 12-86) serum iron 24 µg/dL (RI 65-175) TIBC 729 µg/dL (RI 250-410) saturation 3 % (RI 20-55) Question 3 What is the most likely diagnosis? 7 Answer 3: Diagnosis Iron deficiency anemia Clinical Course Diagnostic procedures included upper GI endoscopy, colonoscopy, and small bowel biopsy. All were negative. The patient received packed RBC transfusions and was started on iron therapy. The etiology of her iron deficiency anemia could not be determined, but it was most likely nutritional. 8 History 3: 51 year old male. Seen by physician for routine preoperative exam prior to dental surgery. Found to have low hemoglobin and a large left upper quadrant mass. Physical Exam: Marked splenomegaly extending from the left costal margin to just above the iliac crest. No other organomegaly. CBC RBC 3.36 x 10[12]/L HGB 10.9 g/dL HCT 31.2 % MCV 92.8 fL MCH 32.4 pg MCHC 34.9 g/dL WBC 9.3 x 10[9]/L N 14 % L 15 % Abnormal cells 71% (shown) PLT 59 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 9 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: The abnormal cells have round or indented nuclei with a fairly coarse chromatin pattern. They have variable amounts of grainy blue-gray cytoplasm with irregular ragged borders and numerous projections. PLT morphology: Within normal limits Question 2: What further laboratory studies, if any, are indicated? 10 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: Marrow was difficult to obtain. A small amount of fluid was aspirated, and the differential showed 78.1% abnormal cells similar to those in the blood. Sections: Hypocellular with a diffuse loosely structured infiltrate of mononuclear cells. Increased areas of fibrosis. Cytochemistry: Tartrate resistant acid phosphatase (TRAP) stain of abnormal cells: positive Immunophenotyping: Not done. Question 3 What is the most likely diagnosis? Answer 3 Diagnosis Hairy cell leukemia Clinical Course The patient was treated with appropriate therapeutic agents and responded well. 11 History 4 25 year old male. Recurrent upper respiratory infections with fever, nausea, and submandibular swelling for several months prior to admission. Noted that cuts on his hands did not heal well. Physical Exam Submandibular adenopathy. No other organomegaly CBC RBC 2.70 x 10[12]/L HGB 9.9 g/dL HCT 28.7 % MCV 106.3 fL MCH 36.9 pg MCHC 34.8 g/dL WBC 7.9 x 10[9]/L N 4 %, L 16%, M 1%, E 0, B 0 Abnormal cells 79% (shown) PLT 50 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 12 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normochromic 1+ polychromasia 1+ macrocytosis WBC morphology: The abnormal cells are medium-sized blasts. The nuclei are often irregular in shape, and some have invaginations or deep clefts. Most have a fine chromatin pattern and one or more prominent nucleoli. The cytoplasm is basophilic, and thin Auer rods are seen. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 13 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: The differential showed 93.6% blasts similar to those in the blood. Dyserythropoiesis was not seen in the red cell precursors. Sections: Markedly hypercellular. Cytochemistry: Myeloperoxidase: positive Sudan black B: positive Non-specific esterase: negative Immunophenotyping: Not done. Cytogenetics: Not done. Question 3 What is the most likely diagnosis? 14 Answer 3 Diagnosis Acute myeloblastic leukemia (AML) FAB M1 Clinical Course Chemotherapy was started, and remission was induced within one month. The post-induction marrow showed normal regeneration, with 2.5% blasts. The patient was placed on consolidation chemotherapy, and followed in Oncology Clinic. He was still in remission 4 years after diagnosis. Note: The patient's MCV returned to the normal range shortly after induction was started, and the cause of his mild macrocytosis was not investigated. 15 History 5 34 year old female. Two day history of ecchymoses, petechiae, and hematuria. She had noted headaches, nausea, and increasing dysphoria over the past week. Physical Exam: Mild scleral icterus. Scattered ecchymoses and petechiae. Appeared anxious and agitated. CBC RBC 2.38 x 10[12]/L HGB 6.6 g/dL HCT 18.4 % MCV 77.5 fL MCH 27.7 pg, MCHC 35.8 g/dL RDW 23.8 WBC 16.9 x 10[9]/L, N 78 % L 14% M 8%, E 0, B 0 PLT 14 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 16 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normochromic 2+ polychromasia 3+ anisocytosis 3+ fragments 2+ spherocytes WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 17 Answer 2: Further Laboratory Studies Coagulation: PT 12.2 sec (RI 11.0-13.5), PTT 29.2 sec (RI 23-34) TT 22.9 sec (RI 13-18), Fibrinogen 0.43 g/dL (RI 0.17-0.37) FDP 80 µg/mL (RI 0-10), D dimer 2320 ng/mL (RI 0-420) Chemistry: BUN 41 mg/dL (RI 9-23) Creatinine 0.8 mg/dL (RI 0.3-1.0) Bilirubin Conj. 0.5 mg/dL (RI 0.0-0.3) Total 2.8 mg/dL (RI 0.0-1.3) Haptoglobin <5 mg/dL (RI 50-150) Urinalysis: Large amount of blood present Protein positive (100 mg/dL) Question 3 What is the most likely diagnosis? 18 Answer 3 Diagnosis Thrombotic thrombocytopenic purpura (TTP) Clinical Course Plasma exchange was commenced promptly after admission. Initially, she became more acutely ill, and developed neurologic symptoms (combative and irritable, with fluctuating levels of consciousness). She was continued on plasma exchange and given other appropriate therapy. Over the next several days, her physical and mental status improved, signs of hemolysis diminished, and her PLT count gradually increased. She was discharged to be followed in Hematology Clinic. 19 History 6 6 year old male. Well until 3 weeks prior to admission. Developed upper respiratory symptoms, persistent headaches, bone pain, and easy bruising. Physical Exam: Adenopathy: submandibular, axillary, and cervical. Hepatosplenomegaly. Petechiae and bruises on trunk and limbs CBC RBC 3.34 x 10[12]/L HGB 9.0 g/dL HCT 27.2 % MCV 82.0 fL MCH 27.2 pg MCHC 33.4 g/dL RDW 13.9 WBC 92.4 x 10[9]/L N 4 % L 8%, M 1% E 0 B 1% Abnormal cells 86 (shown) PLT 18 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 20 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: The abnormal cells are small to medium-sized blasts. They have a relatively fine chromatin pattern, one or more indistinct nucleoli, and scanty basophilic cytoplasm. Occasional cells show nuclear clefts. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 21 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: The differential showed 89.1% blasts similar to those in the blood. Sections: Markedly hypercellular. Cytochemistry: Myeloperoxidase negative Sudan black B negative PAS positive (intensely staining clumps in cytoplasm) Immunophenotyping: TdT positive, B precursor markers positive, T precursor markers negative, Myelomonocytic markers negative Cytogenetics: 46, XY. No numerical or structural abnormalities found. Cerebrospinal fluid analysis: Clear, colorless CSF, Glucose 62 mg/dL (RI 50-80), Protein 25 mg/dL (RI 20-60), RBC 85 x 10[6]/L, WBC 2 x 10[6]/L Gram stain negative Culture negative Question 3 What is the most likely diagnosis? 22 Answer 3 Diagnosis B precursor ALL (acute lymphoblastic leukemia), FAB L1 Clinical Course Induction chemotherapy was started. Since there were several poor prognostic factors (high WBC, organomegaly), protocol included intrathecal therapy. Two weeks later, the marrow was hypocellular with 1% blasts. The patient's physical signs and laboratory values returned to normal, and he was discharged to the care of the Pediatric Oncology Clinic. He continues in remission. 23 History 7 72 year old male. Symptoms of itching, rash, skin discomfort, and malaise increasing over several months. Physical Exam: Generalized erythroderma. Skin appeared leathery, cracked, and peeling. Bilateral epitrochlear and inguinal adenopathy. CBC RBC 4.80 x 10[12]/L HGB 14.2 g/dL HCT 42.4 % MCV 88.3 fL MCH 29.7 pg MCHC 33.6 g/dL WBC 10.8 x 10[9]/L N 35 % L 13 M 8 E 4 B 0 Abnormal cells 40 (shown) PLT 158 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 24 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normocytic, normochromic WBC morphology: The abnormal cells have convoluted cerebriform nuclei. The cytoplasm is basophilic, and occasionally contains small vacuoles. Both small and large cell types are seen. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 25 Answer 2 Further Laboratory Studies Cytochemistry: PAS: many of the abnormal cells show punctate PAS positivity around the nuclei. Immunophenotyping: Elevated CD3 and CD4 positivity consistent with helper T cell phenotype. Question 3 What is the most likely diagnosis? 26 Answer 3 Diagnosis Sezary syndrome (Confirmed by skin and lymph node biopsy.) Clinical Course The patient was treated with photochemotherapy and topical medications. His pruritis, cutaneous discomfort, and erythroderma gradually improved. 27 History 8 34 year old male. Seen for treatment of superficial skin wounds resulting from a shotgun accident while grouse hunting. Family physician noted slight pallor, jaundice, and scleral icterus. History of cholecystectomy five years prior to admission. At that time the patient was told he had Gilbert's syndrome. He stated he had always had "low blood," and that his father and paternal grandfather both had "liver ailments." Physical Exam: Somewhat pale yellowish skin with scattered small surface wounds-mostly over the face, scalp and upper extremities. Moderate scleral icterus. Spleen palpable 3 cm below the left costal margin. CBC (with microscopic differential) RBC 3.93 x 10[12]/L HGB 11.3 g/dL HCT 33.1 % MCV 84.1 fL MCH 28.8 pg MCHC 34.4 g/dL RDW 18.7 WBC 5.0 x 10[9]/L N 53 % , L 31%, M 8%, E 6%, B 2% PLT 362 x 10[9]/L 28 Question 1 What morphologic alterations are seen in this blood smear field? Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normochromic 2+ polychromasia 2+ anisocytosis 2+ spherocytes 1+ echinocytes WBC morphology:Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limit Question 2 What further laboratory studies, if any, are indicated? 29 Answer 2 Further Laboratory Studies Hematology: Reticulocytes 14.3 % Absolute 562 x 10[6]/L Osmotic fragility (unincubated) Initial hemolysis 0.65% NaCL Complete hemolysis 0.40% NaCL Control: Initial 0.50%; Complete 0.20% Osmotic fragility (incubated) Initial hemolysis 0.85% NaCL Complete hemolysis 0.60% NaCL Control: Initial 0.60%; Complete 0.20% Chemistry: Bilirubin Conj. 0.5 mg/dL (RI 0.0-0.3) Total 5.8 mg/dL (RI 0.0-1.3) Question 3 What is the most likely diagnosis? 30 Answer 3 Diagnosis Hereditary spherocytosis Clinical Course The patient was referred to a hematologist to evaluate the advisibility of a splenectomy 31 History 9 15 year old male. Flu-like symptoms with a severe sore throat for two weeks prior to admission. Physical Exam: Cervical and axillary adenopathy. No other organomegaly. CBC RBC 3.15 x 10[12]/L HGB 9.9 g/dL HCT 28.5 % MCV 90.5 fL MCH 31.4 pg, MCHC 34.7 g/dL RDW 15.2 WBC 42.6 x 10[9]/L L 12 % Abnormal cells 88 (shown) PLT 22 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 32 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normochromic 1+ teardrops 1+ elliptocytes 1+ fragments WBC morphology: There is a spectrum of abnormal cells. The most immature are blast forms with ovoid nuclei, delicate chromatin, single large nucleoli, and a moderate amount of gray-blue cytoplasm. The more mature cells have folded or convoluted nuclei, less obvious nucleoli, and abundant blue-gray cytoplasm with variable numbers of fine azurophilic granules. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 33 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: The differential showed 100% cells similar to those seen in the blood. Sections: Markedly hypercellular. Cytochemistry: Myeloperoxidase negative Sudan black B negative Non-specific esterase positive Immunophenotyping: Not done. Chemistry: Serum lysozyme 162 mg/L (RI 4-13) Question 3 What is the most likely diagnosis? 34 Answer 3 Diagnosis: Acute monocytic leukemia with differentiation (FAB M5b) Clinical Course Induction chemotherapy was complicated by DIC. Remission was never obtained. The patient's condition progressively worsened. At his and his family's request, therapy was stopped, and he was discharged to be cared for at home. He died one week later. 35 History 10: 30 year old male. Almost 4 years prior to admission, he was diagnosed with a malignant brain tumor. It was removed surgically and he received chemotherapy. After about three years, the tumor recurred. He was treated with radiation, and chemotherapy was resumed. During a clinic visit he was found to have a fever of 101°F, WBC of 1.0 x 10[9]/L, and absolute neutrophil count of 0 (zero). He was admitted to the hospital and started on IV antobiotics and daily G-CSF injections. This CBC is from the sixth day of growth factor therapy. CBC RBC 3.17 x 10[12]/L HGB 10.4 g/dL HCT 30.0 % MCV 94.7 fL MCH 32.9 pg MCHC 34.7 g/dL RDW 11.9 WBC 23.9 x 10[9]/L N seg 52 % N band 13 N meta 8 N myelo 8 N pro 4 Myeloblast 1 L 8 M 3 E 3 PLT 103 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 36 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normocytic, normochromic 1+ polychromasia WBC morphology: Both mature and immature stages of neutrophils have intense azurophilic granulation. Some bands and segmented forms contain Dohle bodies. Some have bubbly, vacuolated cytoplasm. Neutrophil nuclei are deeply stained, and nuclear projections are seen. Some promyelocytes are extremely large. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 37 Answer 2 Further Laboratory Studies: None Question 3 What is the most likely diagnosis? Answer 3 Diagnosis Shift to the left and reactive changes in neutrophils consistent with response to G-CSF or GM-CSF therapy Clinical Course Following the good response to G-CSF therapy, the patient's fever subsided and he was discharged with plans to continue treatment through the Oncology Clinic. 38 History 11; 33 year old female. Immigrated to the United States from Laos four years prior to admission. History obtained through an interpreter. Multiple transfusions and splenectomy two years prior to admission. Reason and/or diagnosis unclear to patient. Presented with flu-like symptoms of fever, malaise, epigastric discomfort and nonproductive cough. CBC RBC 4.15 x 10[12]/L HGB 8.1 g/dL HCT 28.6 % MCV 68.9 fL MCH 19.5 pg MCHC 28.2 g/dL RDW 22.3 WBC (corrected) 8.0 x 10[9]/L N 51 % L 36 M 7 E 4 B 2 NRBC/100 WBC 83 PLT 540 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 39 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: 3+ hypochromasia 1+ polychromasia 2+ anisocytosis 3+ target cells occ spherocytes and fragments Howell Jolly bodies present WBC morphology: Within normal limits PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 40 Answer 2 Further Laboratory Studies Hemoglobin electrophoresis: Hemoglobin E 80 % Hemoglobin F 5 % Other hemoglobins* 15 % *Identified as hemoglobin A2, hemoglobin Barts and a hemoglobin H mutant. Iron studies: Serum ferritin 3234 ng/mL (RI 12-86) Serum iron 140 µg/dL (RI 65-175) TIBC 152 µg/dL (RI 250-410) Saturation 92 % (RI 20-55) Question 3 What is the most likely diagnosis? 41 Answer 3 Diagnosis Homozygous hemoglobin E disease and alpha thalassemia Clinical Course The patient's flu-like symptoms subsided; they were presumed to be viral in origin. She was referred to the Hematology Clinic, and placed on iron chelation therapy. After 18 months, her serum ferritin had fallen to 114 ng/mL. Her hemoglobin remained in the 7 to 9 g/dL range. Chelation was discontinued, with plans to monitor the ferritin level every six months and resume treatment when needed. 42 History 12; 19 month old male. Referred for evaluation of dysmorphic features. On physical exam, noted to have a large head, coarse facial features, short stature (10th percentile) and moderate hepatomegaly. His mother stated that his early developmental milestones were not delayed (crawled at 6 months, walked alone at 12 months). CBC RBC 3.55 x 10[12]/L HGB 10.3 g/dL HCT 30.3 % MCV 85.3 fL MCH 29.0 pg MCHC 34.0 g/dL RDW 18.5 WBC 6.0 x 10[9]/L N (shown) 29 % L (shown) 68%, M 2%, E 0, B 1% PLT 91 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 43 Answer 1 Morphologic Alterations: Results of the blood smear exam were: RBC morphology: normocytic, normochromic WBC morphology: Some of the lymphocytes have cytoplasmic inclusions which appear as dark purple coarse granules surrounded by a "halo." The neutrophils contain dense azurophilic granulation. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 44 Answer 2 Further Laboratory Studies Biochemical Genetics: WBC enzymes: arylsulfatase B 1.5% of normal mean Urinary mucopolysaccharides, quantitative: 43.1 g/mol cr (RI 3.8-15.3) fractionated: elevated amounts of both heparan and dermatan sulfate detected. Question 3 What is the most likely diagnosis? 45 Answer 3 Diagnosis Mucopolysaccharidosis (MPS) VI (Maroteaux-Lamy syndrome) Clinical Course Initial assessments by the Pediatric Neurology Clinic showed the patient's cognitive and motor skills to be within normal limits for his age. However, he gradually regressed, and by age 4 showed significant developmental delays. His only sibling, a sister, also had MPS VI. Other family members were evaluated as possible bone marrow donors. None of them was a satisfactory match, and he was transplanted with marrow from an unrelated donor. Engraftment was not successful. Note: This patient's lymphocytes contain the distinctive cytoplasmic inclusions often found in cases of MPS. His neutrophils also show the "Alder Reilly anomaly" granulation sometimes seen in MPS. 46 History 13 57 year old male. History of fatigue and blistering of sun-exposed skin for past five years. Physical exam showed extensive blistering of face and hands, and splenomegaly. CBC RBC 3.28 x 10[12]/L HGB 10.8 g/dL HCT 32.5 % MCV 99.1 fL MCH 32.9 pg MCHC 33.2 g/dL RDW 20.8 WBC (corrected) 12.1 x 10[9]/L N 61 % L 29% M6E0B2 NRBC/100 WBC 40 PLT 44 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 47 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normochromic 1+ polychromasia 2+ anisocytosis 1+ macrocytes occ acanthocytes and fragments basophilic stippling present numerous Pappenheimer bodies* WBC morphology: Within normal limits PLT morphology: Within normal limits *Confirmed with Prussian stain: iron granules seen in >90% of RBCs. Question 2 What further laboratory studies, if any, are indicated? 48 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: 63% erythroblasts. Dyserythropoietic changes, including nuclear lobulation and karyorrhexis. On unstained preparations, the erythroblasts were fluorescent when exposed to ultraviolet light. Sections: Hypercellular marrow with erythroid and megakaryocytic hyperplasia. Cytochemistry: Prussian blue iron stain: Increased sideroblasts. Most RBC were iron-laden siderocytes. Urine Chemistries: routine urinalysis: unable to perform due to interfering substances-urine was burgundy-colored. coproporphrin 20,600 µg/24 hr (RI 50-280) uroporphrin 62,550 µg/24 hr (RI 0-50) Question 3 What is the most likely diagnosis? 49 Answer 3 Diagnosis Congenital erythropoietic porphyria Clinical Course The patient was advised to avoid ultraviolet light. His treatment plan (including a splenectomy) resulted in some abatement of his symptoms; however, his thrombocytopenia persists. He continues to be followed in Hematology Clinic. Adult onset of this type of porphyria is very rare. 50 History 14; 37 year old male. Lifelong history of a seizure disorder, treated since age two. At a routine check with his neurologist, he complained of fatigue, exertional dyspnea, and lightheadedness over the past 2-3 months. He appeared pale, but otherwise his physical exam was within normal limits. He was found to have a decreased hemoglobin, and was referred to Hematology Clinic. CBC RBC 1.26 x 10[12]/L HGB 5.7 g/dL HCT 16.3 % MCV 130 fL MCH 45.2 pg MCHC 34.9 g/dL RDW 18.1 WBC 6.2 x 10[9]/L N 73 % L 21 M 1 E 4 B 1 PLT 219 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 51 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normochromic 3+ macrocytosis 3+ anisocytosis Numerous oval macrocytes Occ teardrop cells and fragments WBC morphology: Many neutrophils show nuclear hypersegmentation PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 52 Answer 2 Further Laboratory Studies Bone marrow biopsy Aspirate : Erythroid hyperplasia with megaloblastic maturation. Large polychromatic and orthochromatic megaloblasts show nuclear karyorrhexis and other dyserythropoietic changes. Multiple Howell Jolly bodies are seen in both megaloblasts and oval macrocytes. eutrophils show premature nuclear segmentation, with giant metamyelocytes and band forms. Sections:Appear hypercellular Chemistry: Serum folate <1.0 µg/L (RI 3.5-15) RBC folate 131 µg/L (RI 160-600) Serum B12 136 ng/L (RI 250-900) Question 3 What is the most likely diagnosis? 53 Answer 3 Diagnosis Megaloblastic anemia due to folate deficiency Clinical Course The patient was given large doses of folic acid, and within 6 days his reticulocyte count was 15.2%. One month later, his hemoglobin was 12.7 g/dL, MCV was 92 fL, and his blood smear morphology was normal. The anticonvulsant drug he had been taking is known to interfere with folate metabolism. In addition, the patient had been trying to lose weight, and over the past few months his diet had consisted mainly of TV dinners, with little or no fresh vegetables or fruits. A nutritional consult was arranged, and he was instructed to add folic acid to his daily medications. Note: Patients with folic acid deficiency occasionally show decreased levels of vitamin B12. Because of the patient's history and lack of typical neurologic symptoms, concurrent pernicious anemia was considered very unlikely. 54 History 15 70 year old male. Previously healthy and physically active. Noted sudden onset of fatigue, fever and shaking chills four days prior to admission. Physical Exam: Temperature of 103.5°F. Otherwise, within normal limits. CBC RBC 4.86 x 10[12]/L HGB 14.2 g/dL HCT 42.8 % MCV 88.1 fL MCH 29.2 pg MCHC 33.2 g/dL RDW 14.2 WBC 2.7 x 10[9]/L N 74 % L 24 M 2 E 0 B 0 PLT 16 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 55 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: Rare neutrophils (less than 1%) contain intracytoplasmic inclusions (three examples are shown). PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 56 Answer 2 Further Laboratory Studies Coagulation and chemistry panels were within normal limits. Blood cultures collected at the time of admission were negative. Question 3 What is the most likely diagnosis? 57 Answer 3 Diagnosis Human granulocytic ehrlichiosis. Note: Human granulocytic ehrlichiosis (HGE) is a tick-borne illness caused by rickettsia-like coccobacilli of the genus Ehrlichia. The organisms infect the patient's neutrophils, forming characteristic cytoplasmic inclusions known as morulae. On a Wright-Giemsa stained blood smear, the morula appears as a small (1µ to 3µ diameter) mulberry-shaped intracytoplasmic cluster of bluish coccobacillary organisms. In HGE, morulae are found in the neutrophils, but in a closely related form of ehrlichiosis they occur primarily in monocytes and macrophages. Finding morulae confirms a diagnosis of ehrlichiosis; however, they are not seen in every case. Upon further questioning, it was learned that this patient lived in a wooded area frequented by deer. Although he could not recall a tick bite, he did have a deer feeder in his yard. Clinical Course Following appropriate antibiotic therapy, the patient's condition improved. His fever subsided, his leukopenia and thrombocytopenia resolved, and morulae could no longer be found in his neutrophils. He was discharged in stable condition. 58 History 16 32 year old female. Symptoms of fatigue and chronic headache. Stated she had been treated for "anemia" as a child, but did not recall the reason or the duration of the treatment. No history of familial disease, and no known exposure to chemicals or environmental toxins. Physical Exam The tip of the spleen was palpable. No other significant findings were noted. CBC RBC 3.87 x 10[12]/L HGB 12.9 g/dL HCT 37.3 % MCV 96.4 fL MCH 33.3 pg MCHC 34.5 g/dL RDW 12.4 WBC 6.1 x 10[9]/L N 57 % L 30 M 10 E 1 B 2 PLT 484 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 59 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: dimorphic population (mostly normochromic; some very hypochromic cells) 1+ teardrop cells 1+ target cells 1+ elliptocytes occ fragments basophilic stippling present WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits. Question 2 What further laboratory studies, if any, are indicated? 60 Answer 2 Further Laboratory Studies Chemistry Serum ferritin 536 ng/mL (RI 12-86) Serum iron 105 µg/dL (RI 65-175) TIBC 195 µg/dL (RI 250-410) Saturation 54 % (RI 20-55) Serum folate 4.2 µg/L (RI 3.5-15) Serum B12 236 ng/L (RI 250-900) Bone marrow biopsy: Aspirate: 28.9% erythroblasts. Dyserythropoietic changes not seen. Other cell lines also appeared morphologically normal. Sections: Normocellular marrow. Prussian blue iron stain: Sideroblasts increased in number; 21% type III (ringed) sideroblasts. Question 3 What is the most likely diagnosis? 61 Answer 3 Diagnosis A sideroblastic process of unknown etiology. Clinical Course Because this patient was not anemic, it was decided not to treat her. Nine years after her original diagnosis, she remains clinically stable. Her hematologic parameters, including the hemoglobin, MCV, and serum ferritin have stayed very close to their initial values. She will continue to be followed by Hematology Clinic. 62 History 17 39 year old female. istory of fibrocystic breast disease. Seen for routine work-up prior to breast biopsy. Physical Exam Moderate splenomegaly. No other organomegaly. CBC RBC 4.28 x 10[12]/L HGB 13.4 g/dL HCT 41.2 % MCV 96.3 fL MCH 31.3 pg MCHC 32.5 g/dL WBC 133.6 x 10[9]/L N seg 56 % N band 15 N meta 13 N myelo 4 N pro 3 L 3 M 4 E 1 B 1 PLT 417 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 63 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: Mature stages and precursors all within normal morphologic limits PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 64 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential (1000 cells): Erythroblasts 9.9% Myeloblasts 1.1 N promyelocytes 1.4 N and precursors 71.7 L 2.0 M 2.8 E and precursors 2.2 B and precursors 8.9 Sections: Markedly hypercellular with increased megakaryocytes. Cytochemistry: Leukocyte alkaline phosphatase [LAP] score: 3 (RI 64-176) Cytogenetics: 46,XX,t(9;22)(q34;q11) [Philadelphia chromosome] seen in all marrow cells analyzed. Question 3 What is the most likely diagnosis? 65 Answer 3 Diagnosis Chronic myeloid leukemia (CML) Clinical Course Following the standard preparatory regimen, the patient received an allogeneic bone marrow transplant. The donor was her HLA-matched brother. Her post-transplant course went well, and 28 days later, her hemoglobin was 11.9 g/dL, WBC 2.0 x 10[9]/L, and PLT 84 x 10[9]/L. Her marrow showed evidence of good engraftment in all three cell lines. Cytogenetics showed 46,XY normal karyotype in all marrow cells analyzed. No 46,XX cells and no cells with a Philadelphia chromosome were seen. This patient continues to be followed in Hematology Clinic. At her last visit, ten years post-transplant, she was still doing well and had no evidence of recurrent disease. Molecular diagnostic studies performed at that time were negative for BCR-abl transcripts. 66 History 18 10 year old female. Seen in Pediatric Neurology for evaluation of difficulty with speech, lack of coordination, and decreased school performance. Parents stated that development had seemed "normal" until kindergarten, when it became evident that she was a "slow learner“ and had difficulty speaking clearly. By second grade, her mental and physical capabilities appeared to be progressively deteriorating, and she could no longer keep up with her peers in a regular classroom. Her special ducation teachers suggested medical evaluation. She had 4 siblings, ages 8 to 19 years, all in good health. Physical Exam Her neurologic exam showed significant abnormalities, including slow, slurred speech, general hypotonia, and difficulty in both fine motor skills and coordination. She also had moderate splenomegaly. 67 CBC (with microscopic differential) RBC 5.57 x 10[12]/L HGB 14.6 g/dL HCT 42.6 % MCV 76.5 fL MCH 26.2 pg MCHC 34.3 g/dL WBC 7.0 x 10[9]/L N 72 % L 23 M 4 E1B0 PLT 108 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 68 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: Rare vacuolated lymphocytes (one shown) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 69 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: Numerous large to medium-sized "foamy" appearing macrophages with relatively small central or eccentric nuclei, and cytoplasm filled with fairly uniform, small clear vacuoles. Granulocyte, erythrocyte, and megakaryocyte maturation within normal limits. Sections: Appear slightly hypocellular Biochemical genetics: Skin fibroblast samples from the patient, her parents, and siblings were analyzed for sphingomyelinase activity: Patient: 36 nmol/mg/hr Mother: 65 Father: 69 Siblings 19 yr: 80 16 yr: 85 13 yr: 69 8 yr: 81 Normal Controls (mean): 83 70 Question 3 What is the most likely diagnosis? 71 Answer 3 Diagnosis Niemann-Pick disease Clinical Course The patient was followed in Pediatric Neurology Clinic. Her condition worsened, and she lost the ability to speak, walk, or care for herself. She was last seen in clinic at age 15. Note: In the most prevalent type of Niemann-Pick disease, deterioration is rapid, and survival beyond early childhood is not common. Because this patient had a more chronic course, and did have some enzyme activity, her disease was classified as a Niemann-Pick variant. 72 History 19 30 year old male who stated he had always been in good health. Several years ago at a routine check-up, he was told that he had a mild form of "anemia." He was recently denied insurance coverage after indicating this condition on an application form. Now seeking clarification of his anemia and its impact on his insurability. Physical Exam Within normal limits: no significant findings. CBC RBC 6.22 x 10[12]/L HGB 12.1 g/dL HCT 38.3 % MCV 61.6 fL MCH 19.5 pg MCHC 31.6 g/dL RDW 15.4 WBC 7.1 x 10[9]/L N 55 % L 33 M 10 E 1 B 1 PLT 204 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 73 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normochromic 1+ target cells basophilic stippling present WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 74 Answer 2 Further Laboratory Studies Hemoglobin electrophoresis: Hemoglobin A 92.7% Hemoglobin A2 6.6% Hemoglobin F 0.7% Question 3 What is the most likely diagnosis? 75 Answer 3 Diagnosis Beta thalassemia trait Clinical Course Appropriate documentation of his condition and his eligibility for insurance coverage was provided to the patient. No further follow-up was necessary. 76 History 20 54 year old female. One year history of fatigue, weight loss, and increasingly severe back pain. Physical Exam She appeared pale, but otherwise her physical exam was within normal limits. CBC RBC 2.85 x 10[12]/L HGB 7.6 g/dL HCT 23.9 % MCV 83.8 fL MCH 26.7 pg MCHC 31.8 g/dL RDW 16.8 WBC 8.4 x 10[9]/L N 60 % L 26 M 12 E 1 B 1 PLT 418 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 77 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic Normochromic with occ. hypochromic cells Moderate rouleaux formation WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 78 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential (1000 cells): Erythroblasts 19.2% Myeloblasts 0.4 N promyelocytes 0.8 N and precursors 45.2 L 9.2 M 3.6 E and precursors 3.2 B and precursors 0.0 Plasma cells 18.4 The plasma cells show variable morphology. Many have a normal appearance, but immature forms with prominent nucleoli are also present. ultinucleated plasma cells and occasional very large forms are noted. Sections: Hypercellular with clusters of plasma cells. Immunohistochemical stains for kappa/lambda light chains show sheets of kappa positive cells and a few widely scattered lambda positive cells. Chemistry: Total protein 11.0 g/dL (RI 5.2-8.3) Serum protein electrophoresis: Albumin 3.2 g/dL (RI 3.0-5.0) Globulins: Alpha1 0.4 (RI 0.1-0.5) Alpha2 1.0 (RI 0.5-1.2) Beta 0.8 (RI 0.5-1.1) Gamma 5.6 (RI 0.6-1.7) Monoclonal protein (5.5 g/dL) seen in gamma fraction. Immunoglobulins, quantitative: IgA 9 mg/dL (RI 85-450) IgG 5800 mg/dL (RI 800-1700) IgM 25 mg/dL (RI 60-370) Radiography: Multiple lytic lesions of the skull, spine, pelvis, and femurs. 79 Question 3 What is the most likely diagnosis? 80 Answer 3 Diagnosis Multiple myeloma (IgG, kappa type) Clinical Course The patient was treated with chemotherapy and radiation therapy. Her bone pain lessened, and her serum protein levels gradually decreased to within normal ranges. After several months, however, she was again experiencing bone pain and abnormal protein levels. She continued to be followed in Hematology Clinic, and at her last visit--four years after the original diagnosis--the disease still appeared to be progressing slowly. 81 History 21 23 year old male admitted to the Emergency Room. Blood samples transported to acute care laboratory for stat analysis. No information on patient's condition or the reason for the ER admission was provided. CBC RBC 5.69 x 10[12]/L HGB 15.5 g/dL HCT 45.0 % MCV 79.9 fL MCH 27.2 pg MCHC 34.4 g/dL WBC 12.4 x 10[9]/L N 70 % L 23 M 7 E 0 B 0 PLT 184 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 82 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normochromic 3+ microspherocytes 3+ small fragments 1+ target cells WBC morphology: Reactive neutrophils with Dohle bodies present PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 83 Answer 2 Further Laboratory Studies Chemistry Serum was grossly hemolysed. Sodium 132 mmol/L (RI 136-146) Potassium 5.0 mmol/L (RI 3.7-5.2) Chloride 101 mmol/L (RI 99-112) Bicarb. 23 mmol/L (RI 22-29) BUN 13 mg/dL (RI 9-23) Creatinine 1.4 mg/dL (RI 0.3-1.0) Urinalysis Urine was grossly red. Blood 3+ Protein 3+ Question 3 What is the most likely diagnosis? 84 Answer 3 Diagnosis Acute hemolysis. Morphology suggests severe burns. Clinical Course The patient had been severely burned in a fire at his residence. He suffered 50% total burns with 35% third degree burns. He was immediately transferred to a specialized burn unit, but did not survive. 85 History 22: 11 year old male. Presented in emergency room with recent onset of easy bruising, bleeding gums, and persistent epistaxis. Previously in excellent health. Mother stated he was "never sick before in his entire life." No history of recent viral infection, and no family history of bleeding disorders. Physical Exam: Bleeding from the left nostril. Numerous petechiae and purpura; mostly on the extremities. No organomegaly. CBC RBC 4.52 x 10[12]/L HGB 13.4 g/dL HCT 37.2 % MCV 82.3 fL MCH 29.6 pg MCHC 35.9 g/dLRDW 12.1 WBC 5.3 x 10[9]/L N 44 % L 39 M 14 E 1B2 PLT <5 x 10[9]/L MPV 10.9 fL Question 1 What morphologic alterations are seen in this blood smear field? 86 Answer 1 Morphologic Alterations: Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Appear increased in size Question 2 What further laboratory studies, if any, are indicated? 87 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: Erythrocyte and granulocyte maturation within normal limits. Megakaryocytes appear normal in number and morphology. Sections: Slightly hypocellular for his age, with abundant megakaryocytes. Coagulation: INR 0.91 (RI 0.85-1.15) PTT 24.8 sec (RI 23-34) TT 15.8 sec (RI 13-18) Question 3 What is the most likely diagnosis? 88 Answer 3 Diagnosis Immune thrombocytopenic purpura (ITP) Clinical Course The patient was given standard therapy for ITP for more than a month, but failed to respond. His platelet counts did not improve and he continued to have severe nosebleeds. Because the patient's ITP was refractory to treatment, it was decided to perform a splenectomy. During the procedure, he received several units of platelets, and tolerated the surgery well. His platelet count gradually recovered; after six months it was 289 x 10[9]/L. He is followed in Hematology Clinic, and continues to do well. 89 History 23: 52 year old female.Seen by her local physician for a minor hand injury, and found to be pancytopenic. Referred to University Hematology Clinic. Physical Exam Essentially normal. No organomegaly. CBC RBC 2.19 x 10[12]/L HGB 7.4 g/dL HCT 21.0 % MCV 96.1 fL MCH 33.6 pg MCHC 35.0 g/dL RDW 17.8 WBC 0.8 x 10[9]/L N seg 42 % N meta 1 L 57 PLT 61 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 90 Answer 1 Morphologic Alterations Results of the blood smear exam were : RBC morphology: Normochromic 1+ polychromasia 2+ anisocytosis Occ teardrop cells and elliptocytes WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 91 Bone marrow biopsy 92 Answer 2 Further Laboratory Studies: Bone marrow biopsy: Aspirate: 34.0% neutrophil promyelocytes. The promyelocytes contain abnormal heavy azurophilic granulation. Auer rods are present, and cells with multiple Auer rods (faggot cells) can be found. Sections: Variable cellularity with both hyper- and hypocellular areas, and a predominance of immature granulocytes. Megakaryocytes appear decreased in number. Cytogenetics: 46,XX,t(15;17)(q22;q11-12) seen in 22 of 24 marrow cells analyzed. Two cells had a normal 46,XX female karyotype. Question 3 What is the most likely diagnosis? 93 Answer 3 Diagnosis Acute promyelocytic leukemia (APL) FAB M3 Clinical Course Chemotherapy was started, and remission was achieved. Subsequent bone marrows showed no leukemic cells, and no evidence of cytogenetic abnormality. The patient remained in clinical remission for almost two years, when abnormal promyelocytes and the 15:17 translocation reappeared in her marrow. She was reinduced successfully, and at that time elected to undergo autologous bone marrow transplantation. The transplant was initially successful. Unfortunately, after about one year she again relapsed. The patient decided against further treatment, and she died two months later. 94 History 24, 8 month old male brought to emergency room. In good health until 24 hours prior to admission, when parents noted fever, progressive lethargy, and dark red urine. Product of normal pregnancy and uncomplicated delivery. Diet had consisted mainly of breast milk and formula, with some fruits and vegetables added recently. Parents were both from Egypt. No known family history of anemia, jaundice, gallstones, or splenectomy. Physical Exam: Lethargic, pale infant with jaundiced skin and scleral icterus. Moderate splenomegaly and hepatomegaly. Temperature of 102°F. CBC: RBC 1.28 x 10[12]/L HGB 4.5 g/dL HCT 11.4 % MCV 89.1 fLMCH 35.2 pg MCHC 39.4 g/dL WBC 27.8 x 10[9]/L N seg 65 % N myelo 1 L 31 M 3 E 0 B 0 NRBC/100 WBC 2 PLT 425 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear 95 field? Answer 1 Morphologic Alterations: Results of the blood smear exam were: RBC morphology: Normochromic 2+ polychromasia 3+ irregularly shaped spherocytes 2+ fragments 1+ echinocytes Many of the spherocytes have a clear "veil" or "blister" of membrane on the edge of the cell. RBC fragments include helmet and "bite" cell forms. WBC morphology: Reactive neutrophils with toxic granulation PLT morphology: Within normal limits . Question 2 What further laboratory studies, if any, are indicated? 96 Answer 2 Further Laboratory Studies Chemistry: Serum was grossly hemolysed. Bilirubin Conj. 1.0 mg/dL (RI 0.0-0.3) Total 6.7 mg/dL (RI 0.0-1.3) Haptoglobin <5 mg/dL (RI 50-150) Urinalysis: Urine was grossly red. Blood 3+ Protein 3+ Biochemical Genetics: RBC enzymes: G6PD 0.8 IU/10[11]RBC equiv. (RI 15.2-23.6) Pyruvate kinase levels within normal limits Question 3 What is the most likely diagnosis? 97 Answer 3 Diagnosis Glucose-6-phosphate dehydrogenase (G6PD) deficiency Clinical Course The patient was admitted and transfused with packed RBCs. On the following day, his hemoglobin was 10.7 g/dL. His condition stabilized and his hematuria cleared. He recovered rapidly. Other laboratory parameters returned to normal levels and there was no further evidence of hemolysis. Note: G6PD is an enzyme that protects erythrocyte hemoglobin from oxidation and subsequent denaturation. Individuals with a deficiency of this enzyme are susceptible to hemolytic episodes following oxidant stress to their red cells. In the Mediterranean type of G6PD deficiency, acute hemolysis can be initiated by the ingestion of fava beans. Questioning of the parents disclosed that one of the vegetables that had been added to the infant's diet—on the day before admission--was fava beans. The patient was discharged, and the parents were provided with a list of foods, medications, and other substances that should be avoided by persons with G6PD deficiency. 98 History 25: 4 year old female with history of frequent upper respiratory infections. Fever and sore throat for several days. Found to have decreased WBC and platelet counts, as well as hepatosplenomegaly. Referred for evaluation of possible malignancy. Physical Exam: Pale child with light blonde "silver streaked" hair, light gray-blue eyes, and photophobia. Her liver and spleen were both palpable approximately 8 cm below the respective costal margins. CBC RBC 3.79 x 10[12]/L HGB 11.2 g/dL HCT 32.4 % MCV 85.5 fL MCH 29.6 pg MCHC 34.6 g/dL RDW 12.0 WBC 2.9 x 10[9]/L N 27 % L 66 M 7 E 0 B 0 PLT 73 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 99 Answer 1 Morphologic Alterations: Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: The neutrophils contain irregularly shaped cytoplasmic granules of variable coloration, including large gray granules. Many of the lymphocytes have a single large azurophilic inclusion. Eosinophil granulation is also abnormal, with very large granules present. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 100 Answer 2 Further Laboratory Studies None. The clinical findings and the blood smear were considered diagnostic. Question 3 What is the most likely diagnosis? 101 Answer 3 Diagnosis Chediak-Higashi Syndrome Clinical Course The patient's respiratory infection resolved. She was evaluated for bone marrow transplantation, and within a few weeks received a transplant from an unrelated donor. Following transplantation, her hematologic parameters recovered and remained stable. Eighteen months later she was experiencing graft-versus host disease and mild hypertension, both of which were being treated. Her local physician assumed subsequent responsibility for her medical care. 102 History 26 47 year old male. For several weeks, he had experienced intermittent fevers, chills, and headaches. These became more frequent and severe, and over the past two weeks he also noted increased fatigue, nausea, and loss of appetite. Significant past medical history: congenital kidney defects and chronic pyelonephritis necessitated a renal transplant 18 years before this admission. Prior to transplantation the patient underwent a bilateral nephrectomy and a splenectomy. Since his successful transplant he had been on longterm immunosuppressive agents, and had enjoyed good health. Physical Exam Pale and tired appearing. Temperature of 102.6°F. Several small ecchymoses, in various stages of healing, on his legs. 103 CBC RBC 2.26 x 10[12]/L HGB 7.1 g/dL HCT 20.7 % MCV 91.6 fL MCH 31.4 pg MCHC 34.3 g/dL RDW 16.2 WBC 1.1 x 10[9]/L N 19 % L 79 M 2 E 0 B 0 PLT 68 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 104 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: 1+ hypochromasia 2+ anisocytosis 1+ target cells occ echinocytes Howell-Jolly bodies present Numerous red cells contain small intraerythrocytic ring forms. A few cells contain more than one ring, and occasional tetrad forms are seen. WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 105 Answer 2 Further Laboratory Studies Coagulation: INR 1.1 (RI 0.85-1.15) PTT 28.1 sec (RI 23-34) TT 16.2 sec (RI 13-18) FDP 27 µg/mL (RI 0-10) Chemistry: BUN 24 mg/dL (RI 9-23) Creatinine 1.2 mg/dL (RI 0.3-1.0) Bilirubin Conj. 0.1 mg/dL (RI 0.0-0.3) Total 1.4 mg/dL (RI 0.0-1.3) Haptoglobin <5 mg/dL (RI 50-150) Urinalysis: Large amount of blood present Question 3 What is the most likely diagnosis? 106 Answer 3 Diagnosis Babesiosis Note: Babesiosis is a tick-borne infection of vertebrates caused by intraerythrocytic sporozoan parasites of the genus Babesia. In the United States, the causative organism in humans is usually Babesia microti. On Wright-Giemsa stained blood smears, Babesia appears as a small ring-shaped form within the infected red cells. Because they multiply intracellularly, two and sometimes four parasites (the characteristic "tetrad" form) may be seen within a single cell. Most people infected with Babesia microti remain asymptomatic, or have only mild clinical manifestations. However, persons who are immunocompromised and/or asplenic are at increased risk for severe disease. This patient had recently spent a weekend in an area known to be endemic for Babesia, and recalled experiencing several tick bites. 107 Clinical Course The patient was immediately started on appropriate treatment for babesiosis, and monitored carefully for signs of increasing hemolysis, DIC and/or renal failure. When his laboratory results indicated that his condition was worsening, he was exchange transfused with several units of packed red cells. His clinical condition and pancytopenia gradually improved, and he was discharged. Antibody titers sent to the CDC had confirmed the diagnosis. Within the next six months, the patient was admitted four more times with recurring babesiosis. His post-transplant regimen and his babesiosis treatment were both adjusted, and eventually the infection was brought under control. 108 History 27: 47 year old male. Seen by his local physician for increased weakness and exercise intolerance. His CBC showed pancytopenia and abnormal "blast-like" cells on the blood smear. He was referred to University Hematology Clinic. Physical Exam: Essentially normal. No organomegaly. CBC RBC 3.75 x 10[12]/L HGB 12.7 g/dL HCT 37.7 % MCV 100.5 fL MCH 33.9 pg MCHC 33.7 g/dL RDW 11.6 WBC 1.2 x 10[9]/L N 1 % L 65 abnormal cells 34 (two shown) NRBC/100 WBC 11 (one shown) PLT 58 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 109 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normochromic 1+ polychromasia 1+ macrocytosis Occ elliptocytes and teardrop cells Most of the NRBCs show dysplastic changes. WBC morphology: The abnormal cells are medium sized blasts with a high N/C ratio. The nuclei are round to oval, with a finely dispersed chromatin and one or more prominent nucleoli. There is a variable amount of basophilic cytoplasm. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 110 Answer 2 Further Laboratory Studies: Bone marrow biopsy: Aspirate differential (1000 cells): Erythroblasts 66.1 % Myeloblasts, type I 29.1 N and precursors 2.0 L 2.4 M 0.0 E and precursors 0.4 B and precursors 0.0 The morphology of the myeloblasts is similar to that described for the peripheral blood. No Auer rods are seen. Dyserythropoiesis is marked, with megaloblastoid changes, prominent cytoplasmic vacuolization, nuclear lobulation and karyorrhexis. Sections: markedly hypercellular. Cytochemistry: PAS (periodic acid-Schiff): Erythroblasts contain blocks of PAS positive material in the cytoplasm. Immunophenotyping: The leukemic cells are positive for: CD45, CD34, CD13, CD33, CD14, and CD36. Cytogenetics: 47,XY,+8 seen in virtually all metaphases examined. 111 Question 3 What is the most likely diagnosis? 112 Answer 3 Diagnosis Erythroleukemia (AML FAB M6) Note: The diagnosis of erythroleukemia includes consideration of clinical findings, morphology, and the following bone marrow differential results: 1] 50% or more of the marrow cells are erythroid precursors. 2] 30% or more of the non-erythroid marrow cells are myeloblasts. This case easily meets these criteria. 113 Clinical Course Chemotherapy was started, and the patient achieved remission within two months. His bone marrow showed no residual leukemic cells and no evidence of trisomy 8 or other cytogenetic abnormalities. Because of the poor prognostic factors associated with his leukemia, he decided to undergo bone marrow transplantation as soon as possible. Fortunately, a sibling was an identical HLA match, and the transplant was performed less than six months after his initial diagnosis. His posttransplant course was complicated by graft-versus-host disease, but it eventually resolved. At his last clinic visit, three years after transplant, he was no longer on immunosuppressive drugs, and continued to do well. 114 History 28 22 year old female. Immigrated to the United States from Vietnam three years prior to admission. Enrolled in the Medical Technology program at the University. She had always been in good health. During an introductory hematology class in which students stain and observe their own blood under the microscope, she suspected that some of her cells were not morphologically normal. She asked a teacher to look at the blood smear with her, and the teacher suggested that a CBC be performed. CBC RBC 5.45 x 10[12]/L HGB 11.6 g/dL HCT 34.0 % MCV 62.5 fL MCH 21.3 pg MCHC 34.2 g/dL WBC 4.0 x 10[9]/L N 55 % L 33 M 9 E 3B0 PLT 243 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 115 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: 2+ target cells 2+ elliptocytes occ teardrops and fragments WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 1 What morphologic alterations are seen in this blood smear field? 116 Question 3 What is the most likely diagnosis? Answer 3 Diagnosis: Alpha thalassemia trait Note: The diagnosis of alpha thalassemia trait is often one of exclusion. However, this young woman's characteristic red cell parameters (borderline HGB level, low MCV, relatively high RBC count), her erythrocyte morphology, her ethnic background, and her lack of clinical symptoms strongly support this diagnosis. Clinical Course No treatment was needed. When asked about her family history, the woman related that she was the youngest of ten living siblings, and her mother had also delivered five stillborn infants. 117 History 29: 48 year old female. Found to have anemia and splenomegaly on routine examination by local physician. Referred to University Hematology Clinic. Physical Exam: Spleen palpable to the level of the umbilicus. Liver palpable 3 cm. below right costal margin. The rest of the exam was within normal limits. CBC RBC 3.85 x 10[12]/L HGB 10.4 g/dL HCT 30.8 % MCV 80.0 fL MCH 27.0 pg MCHC 33.7 g/dL RDW 18.8 WBC 4.7 x 10[9]/L N seg 68 % N meta 4 N myelo 2 L 20 M 5 E 0 B 1 NRBC/100 WBC 5 (shown) PLT 143 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 118 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normochromic 1+ polychromasia 2+ anisocytosis 2+ teardrop cells 2+ elliptocytes WBC morphology: Mature stages and precursors all within normal morphologic limits. PLT morphology: A few large irregularly shaped atypical platelets present. Some have dark granulation, others are hypogranular. Question 2 What further laboratory studies, if any, are indicated? 119 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential (500 cells): Erythroblasts 47.6 Myeloblasts 0.6% N and precursors 39.4 L 8.6 M 2.4 E and precursors 1.0 B and precursors 0.4 Marrow smears are markedly dilute. Neutrophil maturation within normal limits. Immature and mature micromegakaryocytes present. Sections: Markedly hypercellular with increased megakaryocytes. Reticulin-stained sections show moderate to marked reticulin fibrosis. Cytogenetics: 46,XX. No numerical or structural abnormalities found. Question 3 What is the most likely diagnosis? 120 Answer 3 Diagnosis Chronic idiopathic myelofibrosis (IMF) Clinical Course Other than abdominal fullness and mild fatigue, the patient continued to have no symptoms of her disease. The option of a bone marrow transplant was discussed with the patient and her family. Although two of her siblings were HLA identical matches, it was decided not to transplant at that time, but to follow the patient closely and reevaluate transplantation if her condition changed. Two years after diagnosis, her disease was still stable, with virtually no changes in her hematologic parameters or her spleen size. She continues to be followed in clinic. 121 History 30 18 year old male student from Nigeria. Came to the emergency room with symptoms of fever, shaking chills, nausea, and generalized malaise; occurring intermittently over the past five days. Physical Exam: Fever of 103.3°F. Tachycardia with a heart rate of 122. Otherwise within normal limits. CBC (with microscopic differential) RBC 5.85 x 10[12]/L HGB 13.3 g/dL HCT 41.8 % MCV 71.5 fL MCH 22.7 pg MCHC 31.8 g/dL RDW 12.1 WBC 6.2 x 10[9]/L N 89 % L 8 M 2 E 1 B 0 PLT 102 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 122 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normochromic Numerous red cells contain intraerythrocytic organisms. Infected RBCs are enlarged; some are oval shaped, others appear somewhat "fimbriated." Doubly infected cells are present, and several morphologic stages can be found, including ring forms, mature schizonts, and gametocytes. WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits. Question 2 What further laboratory studies, if any, are indicated? 123 Answer 2 Further Laboratory Studies Biochemical Genetics: RBC enzyme: G6PD 11.7 U/g Hgb (RI 4.6-13.5) Question 3 What is the most likely diagnosis? 124 Answer 3 Diagnosis: Malaria Upon further questioning, the patient stated that he had arrived in the United States from Nigeria approximately six months prior to this visit. Shortly after his arrival, he had experienced a similar illness that was diagnosed as malaria. Medication was prescribed, but once he felt better he did not continue to take it. Based on the blood smear morphology, the periodic pattern of his fever and chills, and his travel history, the causative organism was identified as Plasmodium ovale. Clinical Course The patient was hydrated with normal saline, and started on appropriate Treatment for the erythrocytic stages of malaria. Several days later he began a second course of therapy to eliminate the exoerythrocytic (hepatic) forms of the organism. He completed the course of therapy, and on subsequent visits was asymptomatic. Note: On the basis of his low MCV, his relatively high RBC count, and his ethnic background, it is likely that this patient also has alpha thalassemia trait. 125 History 31: 11 year old male. Presented to local physician with worsening abdominal and leg pain, decreasing appetite, and weight loss over the previous three weeks. Physical Exam: Large tender mass palpable on the left side of abdomen. Bilateral inguinal adenopathy. Pain with movement of lower extremities. Abdominal CT scan showed a 6 x 7 cm. retroperitoneal mass. He was referred to University Hospital for evaluation. CBC (with microscopic differential) RBC 4.58 x 10[12]/L HGB 12.4 g/dL HCT 36.6 % MCV 80.0 fL MCH 27.2 pg MCHC 34.0 g/dL RDW 12.8 WBC 7.6 x 10[9]/L N 59 % L 25 M 12 E 4 B 0 Rare abnormal cells on scan (one shown) PLT 172 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 126 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: The abnormal cells are medium sized with rounded to slightly irregular nuclei, condensed chromatin, and one or two distinct nucleoli. There is a moderate amount of deeply basophilic cytoplasm. Some cells contain prominent vacuoles, which at times overlay the nucleus. PLT morphology: Within normal limits 127 Question 2 What further laboratory studies, if any, are indicated? Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate: The differential showed 80.2% abnormal cells similar to those in the blood. Sections: Markedly hypercellular. Immunophenotyping: More than 90% of mononuclear cells in the marrow were a monoclonal population strongly positive for surface IgMkappa light chain and B-cell associated antigens CD19, CD20, and CD24. T-cell associated antigens: negative Myelomonocytic antigens: negative TdT: negative Cytogenetics: 46,XY,t(8;14)(q24;q32) in 20 of 21 marrow metaphases analyzed. Surgical Pathology: Wedge biopsies of the abdominal mass were obtained during an exploratory laparotomy. Because it encased the mesenteric vessels, the mass could not be excised completely. 128 Question 3 What is the most likely diagnosis? Answer 3 Diagnosis Burkitt lymphoma/Burkitt cell leukemia (FAB ALL L3) 129 Clinical Course Chemotherapy was started, and was initially complicated by febrile episodes and severe neutropenia. These problems were resolved, and one month later there was no evidence of Burkitt cells in the blood or bone marrow. The patient's clinical status and laboratory values returned to normal, and he was discharged to the care of the Pediatric Oncology Clinic. At last follow-up, 2 1/2 years after diagnosis, he continued to be in remission. 130 History 32: 82 year old female. Brought to Emergency Room with symptoms of severe frontal headache and associated confusion. Noted to have decreased energy level and a 15 pound weight loss over the previous three months. The patient was initially evaluated for a possible CVA. Neurologic exam and CT scans were negative, but she was found to be pancytopenic. Physical Exam: Pale appearing, but otherwise within normal limits. No organomegaly. CBC (with microscopic differential) RBC 2.05 x 10[12]/L HGB 6.6 g/dL HCT 19.9 % MCV 97.1 fL MCH 32.2 pg MCHC 33.2 g/dL RDW 16.4 WBC 3.5 x 10[9]/L N 48 % L 34 M 15 E 3 B 0 PLT 55 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 131 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normochromic 2+ anisocytosis 2+ oval macrocytes 1+ teardrop cells WBC morphology: Dysgranulopoietic changes, including hyposegmentation, pseudo-Pelger-Huët nuclei, and hypogranularity are seen in some neutrophils (one shown here). PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 132 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential (1000 cells): Erythroblasts 24.6 Myeloblasts 7.0% N and precursors 49.0 L 14.0 M 1.8 E and precursors 1.2 B and precursors 1.4 Plasma cells 1.0 Neutrophil maturation is left shifted. Auer rods are not seen in the myeloblasts. Mild dysgranulopoiesis and dyserythropoiesis are noted. Sections:Hypocellular. Megakaryocytes are decreased in number. Cytogenetics: 46,XX,del(5)(q15q33) in 18 of 20 marrow metaphases analyzed. Chemistry: TSH (thyroid stimulating hormone), vitamin B12, and folic acid levels are all within reference ranges. Question 3 What is the most likely diagnosis? 133 Answer 3 Diagnosis Refractory anemia with excess blasts (RAEB) Clinical Course The patient was transfused with packed RBCs. Her condition improved, and she was admitted to an extended care facility. She required transfusions approximately every two weeks to maintain her hemoglobin. Approximately three months after diagnosis her CBC showed an abrupt rise in the WBC count to 59.4 x 109/L, with 74% myeloperoxidase positive blasts (indicative of evolution to acute myeloid leukemia). She and her family declined further treatment, and she was discharged to be cared for at home. 134 History 33 75 year old male. Symptoms of severe headache and generalized pruritis. Physical Exam Spleen palpable 10 cm. below left costal margin. Liver palpable 3 cm. below right costal margin. The rest of the exam was within normal limits. CBC (with microscopic differential) RBC 7.70 x 10[12]/L HGB 17.3 g/dL HCT 54.3 % MCV 97.1 fL MCH 32.2 pg MCHC 33.2 g/dL RDW 16.4 WBC 18.3 x 10[9]/L N seg 79 % N myelocyte 5 % L 9 M 4 E 0 B 3 PLT 484 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 135 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Essentially normocytic, normochromic WBC morphology: Within normal limits PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 136 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential: Within normal limits Sections: Markedly hypercellular for age. Megakaryocytes normal in morphology and moderately increased in number. Cytogenetics: 46,XY. No numerical or structural chromosome abnormalities detected. Pulmonary function: Oxygen saturation: 97% (RI 94-100) Question 3 What is the most likely diagnosis? 137 Answer 3 Diagnosis Polycythemia vera Clinical Course The patient is being followed by his local physician, and treated with periodic phlebotomy. 138 History 34 53 year old male. Healthy and physically active. Recently noted fatigue and groin soreness. Physical Exam Adenopathy: several small (~1 cm diameter) soft nodes in supraclavicular and axillary areas. Two larger (>2 cm diameter) firm inguinal nodes. No other organomegaly. The rest of the exam was within normal limits. CBC (with microscopic differential) RBC 4.02 x 10[12]/L HGB 13.6 g/dL HCT 38.3 % MCV 95.3 fL MCH 33.8 pg MCHC 35.5 g/dL RDW 12.4 WBC 51.3 x 10[9]/L N 10 % L 89 M 1 PLT 156 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 139 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normocytic, normochromic WBC morphology: Most of the lymphocytes are small and mature appearing with clumped chromatin and a high nuclear to cytoplasmic ratio. Some cells are slightly larger with less clumped chromatin. There are increased numbers of damaged cells. PLT morphology: Within normal limit Question 2 What further laboratory studies, if any, are indicated? 140 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential: 68% lymphocytes morphologically similar to those described in the blood. Sections: Normocellular with a predominantly interstitial infiltrate of small lymphocytes. Occasional focal infiltrates also seen. Immunophenotyping: More than 90% of the lymphoid cells in the marrow are monotypic/monoclonal B lymphocytes. They are weakly reactive for SIg and CIg, showing mu and delta heavy chains and kappa restricted light chains. The cells are strongly reactive for CD5, 19, 20, 22, 23, 24, and HLA-DR; moderately reactive for CD11c, and negative for CD10. Cytogenetics: 46,XY. No numerical or structural chromosome abnormalities detected. Question 3 What is the most likely diagnosis? 141 Answer 3 Diagnosis B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma (B-cell CLL/SLL) Clinical Course The patient was initially followed without therapy. He had no additional symptoms and stable hematologic parameters for about two years. At that time, he developed splenomegaly and his WBC gradually began to increase, eventually reaching >200 x 10[9]/L. Appropriate chemotherapy was initiated, and his WBC dropped to acceptable levels. His spleen size remains constant, and he continues to be followed by Hematology Clinic. 142 History 35 50 year old male. Admitted with symptoms of chest discomfort and shortness of breath. History of splenectomy secondary to trauma 21 years prior to this admission. Physical Exam: Cardiovascular examination was unremarkable, and the electrocardiogram was within normal limits. The liver appeared slightly enlarged. CBC (with microscopic differential) RBC 3.83 x 10[12]/L HGB 12.9 g/dL HCT 36.7 % MCV 95.8 fL MCH 33.7 pg MCHC 35.2 g/dL RDW 19.7 WBC 62.0 x 10[9]/L N seg 14 % N band 11 % N meta 2 % L 8 M 1 E 64 B 0 PLT 429 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 143 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: normochromic 2+ anisocytosis 1+ target cells occ acanthocytes Howell-Jolly bodies present WBC morphology: Many of the eosinophils are hypogranular and show dysplastic changes. PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 144 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential: 42.8% eosinophils and precursors, many of which are hypogranular. Maturation of erythrocytes, neutrophils, and megakaryocytes is within normal limits. Sections: Hypercellular with increased eosinophils. Leukocyte alkaline phosphatase [LAP] score: 89 (RI 64-176) Cytogenetics: 46,XY. No numerical or structural chromosome abnormalities detected. Question 3 What is the most likely diagnosis? 145 Answer 3 Diagnosis Chronic eosinophilic leukemia (hypereosinophilic syndrome Clinical Course Over the next six years, the patient was given several courses of chemotherapy, which were effective for only short periods of time. He developed progressive cardiomyopathy and experienced a cerebrovascular accident. During his final hospital admission, his WBC rose rapidly and he developed bilateral pleural effusions. He deteriorated rapidly, and he and his family elected to forego all but supportive therapy. He died seven years after his original diagnosis. 146 History 36 30 year old male. Symptoms of fatigue, sore throat, and heat intolerance. Stated he had always been mildly anemic, and had one brother with a "blood problem." Physical Exam Spleen and liver slightly palpable. The rest of the exam was within normal limits. CBC (with microscopic differential) RBC 4.21 x 10[12]/L HGB 13.7 g/dL HCT 40.0 % MCV 95.0 fL MCH 32.5 pg MCHC 34.3 g/dL RDW 17.0 WBC 7.0 x 10[9]/L N 51 % L 42 M 3 E 4 B 0 PLT 310 x 10[9]/L Question 1 What morphologic alterations are seen in this blood smear field? 147 Answer 1 Morphologic Alterations Results of the blood smear exam were: RBC morphology: Normochromic with a few hypochromic cells 2+ anisocytosis 2+ teardrop cells 1+ RBC fragments 1+ elliptocytes 1+ target cells Basophilic stippling seen WBC morphology: Within normal limits (one lymphocyte shown here) PLT morphology: Within normal limits Question 2 What further laboratory studies, if any, are indicated? 148 149 Answer 2 Further Laboratory Studies Bone marrow biopsy: Aspirate differential: 36.6% erythroblasts. There is marked dyserythropoiesis with giant erythroblasts, multinucleation, karyorrhexis, and nuclear/cytoplasmic asynchrony. The changes are more pronounced in the later stages (polychromatic and orthochromatic erythroblasts). Several giant anucleate erythrocytes are seen. Maturation of granulocytes and megakaryocytes is within normal limits. Sections: Normocellular with diffusely scattered dyserythropoietic elements. Chemistry: Iron studies, serum lead, folic acid levels, and TSH (thyroid stimulating hormone) were all within reference ranges. Acidified serum test negative Haptoglobin 17 mg/dL (RI 50-150) Question 3 What is the most likely diagnosis? 150 Answer 3 Diagnosis Probable congenital dyserythropoietic anemia (CDA) Clinical Course Because his anemia was mild, it was decided that the patient did not require treatment at the time. He was subsequently lost to follow-up. Note: The congenital dyserythropoietic anemias have traditionally been divided into three types: CDA I, II, and III. However, there is some overlap between types, and it may be difficult to classify individual cases. This patient's disorder most closely resembles CDA III. 151 • Diagnostic Criteria for Chronic Neutrophilic Leukemia • Peripheral blood leukocytosis >25 x 109/L – Segmented neutrophils and bands >80% of leukocytes – Immature granulocytes <10% of leukocytes – Myeloblasts <1% of leukocytes • Hypercellular bone marrow – Increased number and percentage of neutrophilic granulocytes – Nucleated marrow cells with <5% myeloblasts – Normal neutrophilic maturation pattern • Hepatosplenomegaly • No Philadelphia chromosome or bcr/abl fusion gene • No other cause for neutrophilia – No infectious or inflammatory process – No evidence of another myeloproliferative disease – No evidence of a myelodysplastic or myelodysplatic/myeloproliferative disease – No evidence of a tumor or, if present, the myeloid cells must show clonality 152 Diagnostic Criteria Leukemia for Chronic Myelomonocytic Persistent monocytosis (>1 x 109/L) in the peripheral blood No Philadelphia chromosome or bcr/abl fusion gene <20% blasts and promonocytes in the peripheral blood and bone marrow >1 myeloid lineage with dysplasia o if there is no dysplasia the diagnosis of CMML can still be made if the other requirements are satisfied and: o the marrow cells contain an acquired, clonal cytogenetic abnormality, or o persistent monocytosis for 3 months and o exclusion of all other causes of monocytosis 153 • Diagnostic Criteria for Chronic Eosinophilic Leukemia • Persistent eosinophilia >1.5 x 109/L in blood, increased bone marrow eosinophils • >5% but <19% myeloblasts in the bone marrow or >2% in the peripheral blood • Clonality of myeloid cells • No reactive eosinophilia due to allergy, parasitic, infectious, pulmonary, or collagen vascular disease • No reactive eosinophilia due to other malignancies: • T-cell lymphomas • Acute lymphoblastic leukemia/lymphoma • Other myeloproliferative diseases • Acute myeloid leukemia – including inv(16), t(16;16) • Mastocytosis • CML • Myelodysplastic syndrome • Hodgkin's lymphoma • No T-cell population with abnormal cytokine production and aberrant phenotype • CML=Chronic myelogenous leukemia 154 • Diagnostic Criteria for Accelerated and Blast-Phase Chronic Myelogenous LeukemiaAccelerated Phase (Requires one or more of the following criteria):Blast Phase (Requires one or more of the following criteria): • Blasts comprising 10 to 19% of the peripheral blood WBCs and/or of nucleated bone marrow cells • >20% peripheral blood basophils • Persistent thrombocytopenia (<100 x 109/L) unrelated to treatment • Persistent thrombocytosis (>1000 x 109/L) unresponsive to treatment • Increasing splenomegaly or leukocytosis unresponsive to treatment • Cytogenetic evidence of clonal evolution • Blasts composing >20% of peripheral blood WBCs or of nucleated bone marrow cells • Extramedullary blast proliferation • Large foci or clusters of blasts in the bone marrow biopsy 155