Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
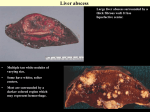
The new england journal of medicine case records of the massachusetts general hospital Founded by Richard C. Cabot Nancy Lee Harris, m.d., Editor William F. McNeely, m.d., Associate Editor Jo-Anne O. Shepard, m.d., Associate Editor Sally H. Ebeling, Assistant Editor Stacey M. Ellender, Assistant Editor Christine C. Peters, Assistant Editor Case 16-2003: A 58-Year-Old Woman with Left-Sided Weakness and a Right Frontal Brain Mass Robert M. Friedlander, M.D., R. Gilberto Gonzalez, M.D., Nadeem A. Afridi, M.D., and Rolf Pfannl, M.D. presentation of case A 58-year-old, right-handed woman was admitted to the hospital because of left hemiparesis. The patient had been well until five days earlier, when a right frontal headache developed, with radiation to the right eye and right ear; suspecting sinusitis, her physician prescribed amoxicillin. Four days before admission, weakness developed in the left arm, and she began to drop items that she was holding in her left hand. During the next three days, the weakness worsened. On the day of admission, she awoke with weakness in the left leg; at one point, she fell from a chair and was unable to rise or walk. She was brought to this hospital, where a right-sided intracranial mass was detected and she was admitted. The patient was married and was employed as an executive. There was a history of similar headaches, without radiation to the eyes or ears, associated with bouts of sinusitis that had been treated with antibiotics; these headaches had usually been accompanied by rhinorrhea, which was absent on this occasion. Her family had noted increasing somnolence during recent days but had observed no confusion or other neurologic symptoms except for the left hemiparesis. She was in excellent health and ordinarily took no medications. She did not smoke and consumed alcohol in moderate amounts. Four dental cavities had been filled during the preceding two weeks. She was allergic to sulfonamide. The temperature was 36.8°C, the pulse 65 beats per minute, and the respiratory rate 16 breaths per minute. The blood pressure was 125/80 mm Hg. On physical examination, the patient appeared well. Findings on a general examination were unremarkable, and no cardiac abnormality was detected. On neurologic examination, the patient was sleepy but alert and oriented, with fluent speech. Both pupils were 3 mm in diameter and constricted to 2 mm on exposure to light; extraocular movements and the visual fields were intact. Weakness in the central area of the left side of the face was noted. Strength was 4/5 in the left deltoid, biceps, triceps, and forearm and hand grip muscles and in the interosseous, iliopsoas, quadriceps, hamstring, soleus, and gastrocnemius muscles and was 5/5 in the same muscles on the right side. There was no pronator drift of the outstretched arms. The sensation of a n engl j med 348;21 www.nejm.org From the Department of Neurosurgery, Brigham and Women’s Hospital (R.M.F.); the Divisions of Neuroradiology (R.G.G.), Cardiology (N.A.A.), and Neuropathology (R.P.), Massachusetts General Hospital; and the Departments of Neurosurgery (R.M.F.), Radiology (R.G.G.), Medicine (N.A.A.), and Pathology (R.P.), Harvard Medical School — all in Boston. N Engl J Med 2003;348:2125-32. Copyright © 2003 Massachusetts Medical Society. may 22, 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2125 The new england journal light touch was preserved. The deep-tendon reflexes were ++ bilaterally, and the plantar responses were flexor. The urine was normal. The hematocrit was 36.2 percent; the white-cell count was 7000 per cubic millimeter, with 82 percent neutrophils, 13 percent lymphocytes, 4 percent monocytes, and 1 percent eosinophils; the platelet count was 308,000 per cubic millimeter, and the mean corpuscular volume 88 µm3; the prothrombin and partial-thromboplastin times were normal. The phosphorus level was 2.1 mg per deciliter (0.68 mmol per liter). The aspartate aminotransferase level was 48 U per liter, and the alanine aminotransferase level 60 U per liter. The levels of urea nitrogen, creatinine, glucose, conjugated and total bilirubin, calcium, magnesium, total protein, albumin, globulin, electrolytes, creatine kinase, creatine kinase isoenzymes, troponin T, and alkaline phosphatase were normal. An electrocardiogram showed a normal rhythm at a rate of 60 beats per minute, with low T waves throughout. Computed tomographic (CT) scanning of the head, performed without intravenous injection of contrast material, revealed a large, complex, predominantly low-attenuation mass in the right frontal lobe, measuring 7.3 cm in the anteroposterior projection and 5.8 cm in the transverse direction; a component located more centrally and measuring 3.5 cm in diameter was observed in the region of the lentiform nucleus and had a level of attenuation similar to that of the brain. There was effacement of the overlying sulci and the temporal horns of the right lateral ventricle and probably some degree of uncal herniation on the right side. A midline shift of 7 to 8 mm to the left was noted; no hydrocephalus, evidence of infarction, intraparenchymal hemorrhage, abnormal collection of extra-axial fluid, or osseous abnormalities were noted. A magnetic resonance imaging (MRI) study of the brain (Fig. 1) disclosed a mass, 3.7 by 2.5 by 2.9 cm, in the right lentiform nucleus; on T2-weighted images the mass was surrounded by an area of hyperintensity, a finding consistent with edema. There was a mass effect, with effacement of right hemispheric sulci, partial effacement of the right lateral ventricle, a midline shift of approximately 8 mm, and slight right-sided uncal herniation. On a diffusion MRI study (Fig. 2), evidence of restricted diffusion was observed centrally in the region of the mass that was hyperintense on diffusion-weighted images and hypointense on apparent-diffusioncoefficient images; no other abnormalities were identified. Chest radiographs showed a probable 2126 n engl j med 348;21 of medicine A B Figure 1. MRI Study of the Brain Showing a Heterogeneous Mass in the Right Frontal Lobe That Compresses the Right Lateral Ventricle. A T2-weighted image without contrast (Panel A) shows a mass (arrow) with high signal intensity centrally, a heterogeneous peripheral ring of signal intensity similar to that of the brain parenchyma, and a surrounding area of bright signal in the white-matter tracts. On the contrast-enhanced T1-weighted image (Panel B), the mass has low signal intensity in the central region, suggesting the presence of fluid, and is surrounded by a ring of enhancement. Beyond the ring of enhancement, a less well-defined area of abnormal low signal extends along the white-matter tracts. www.nejm.org may 22 , 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved. case records of the massachusetts general hospital granuloma, 3 mm in diameter, in the middle zone of the left lung peripherally; the lungs were clear in other respects. The bones appeared osteopenic; the aorta was tortuous and ectatic, and the heart was normal in size and configuration. Several hours after admission, the temperature rose to 38.3°C. Phenytoin and dexamethasone were given intravenously, and the temperature was normal on all subsequent occasions. A diagnostic procedure was performed. A differential diagnosis Dr. Robert M. Friedlander: May we review the radiographs? Dr. R. Gilberto Gonzalez: A CT scan of the head, obtained without the intravenous administration of contrast material, revealed a large, heterogeneous mass in the right frontal lobe. The mass was centrally hypodense. Surrounding this central component was a ring of material that was isodense relative to the brain parenchyma. Beyond this ring was a further area of hypodensity along the white-matter tracts. There was evidence of subfalcine herniation, a midline shift, and compression of the right lateral ventricle. Several hours later, MRI scanning was performed before and after the administration of contrast material. There is a heterogeneous mass in the right frontal lobe. On T2-weighted images (Fig. 1A), the mass has high signal intensity centrally, has a heterogeneous peripheral ring of signal intensity similar to that of the brain parenchyma, and is surrounded by bright signal in the white-matter tracts. There is a mass effect involving compression of the right lateral ventricle. T1-weighted images obtained after the administration of contrast material (Fig. 1B) show that the peripheral ring is enhanced; the central component of the mass and the surrounding white-matter tracts are hypointense on T1weighted images, both with and without the use of contrast. A diffusion MRI study was also performed. The diffusion-weighted image reveals a hyperintense central area (Fig. 2A), which appears hypointense on the apparent-diffusion-coefficient image (Fig. 2B) — a finding indicating restricted diffusion, a characteristic of viscous materials. Surrounding the areas of restricted diffusion are areas of increased signal intensity, consistent with the presence of extracellular edema. Dr. Friedlander: The patient is a 58-year-old wom- n engl j med 348;21 B Figure 2. Diffusion MRI Study of the Brain. The diffusion-weighted image (Panel A) shows an area of hyperintensity corresponding to the central area of the mass (arrow). The apparent-diffusion-coefficient image (Panel B) shows that the central component of the mass has a very low signal (arrow), indicating that the diffusion of water is highly restricted and suggesting the presence of viscous fluid. A surrounding area of high signal suggests edema along the white-matter tracts. www.nejm.org may 22, 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2127 The new england journal of medicine an with a five-day history of headache and progressive left-sided weakness. The patient had previously been healthy, except for occasional bouts of sinusitis that had been treated with antibiotics. Of note, she recently had four dental cavities filled. Imaging performed on admission showed a cystic, ring-enhancing lesion in the right frontal lobe of the brain. Thirty years ago, the diagnostic questions in this case would have been daunting. The patient’s clinical findings would have allowed the location of the lesion to be identified as the right cerebral hemisphere. However, without the assistance of CT or MRI studies, it would have been impossible to be sure whether the patient’s neurologic deficits were due to a lesion that was infectious, neoplastic, vascular, or inflammatory in origin. In this patient, modern imaging studies show a space-occupying, ring-enhancing, cystic lesion surrounded by edema, with no evidence of infarction. From that information alone, we can refine our focus dramatically (Table 1). primary concern, but in this case that information provides only limited guidance in narrowing the list of diagnostic possibilities. From this patient’s history, we learn that her symptoms began five days before admission with a right frontal headache; one day later, progressive weakness of the left arm developed, followed on the day of admission by the onset of weakness of the left leg. These symptoms help to identify the likely site of the lesion as the right cerebral hemisphere, and although in themselves they do not indicate the cause, the course and progressive nature of the symptoms are informative. Symptoms from a vascular event such as an infarction or hemorrhage would be expected to reach their peak in less than five days, and usually within hours. At the other end of the spectrum, patients with primary or secondary cerebral neoplasms tend to present with symptoms of several weeks’ duration, although a much shorter duration is not uncommon. Symptoms associated with brain abscesses have a brief course and progressive nature, as did those seen in this patient.1-5 We also learn that the patient had had bouts of important features sinusitis and in the preceding two weeks had unConsideration of a patient’s history, findings on dergone treatment of dental cavities. Both sinus inphysical examination, and laboratory data are of fections and dental procedures are well-known risk factors for the development of cerebral abscesses. Dental procedures increase the risk of brain abTable 1. Differential Diagnosis of Ring-Enhancing Brain scesses on a continuum ranging from simple cleanLesions. ing, which is associated with the lowest risk, to tooth extraction, which is associated with the highInfections est risk. Some authors believe that although dental Pyogenic brain abscess infections are a risk factor for the development of Toxoplasmosis brain abscesses, dental procedures alone may not Cysticercosis raise the risk of brain abscess at all.6 Other clinical and laboratory data in this case Necrotic fungal infection provide some useful information. The patient was Neoplasms initially afebrile but had a temperature of 38.3°C Primary brain tumors several hours after admission. The elevated temAggressive glial tumors, especially glioblastoma perature strongly suggests the presence of an inmultiforme or anaplastic astrocytoma Primary central nervous system lymphoma fection. The laboratory data show an elevated percentage of neutrophils in the context of a normal Demyelinating diseases white-cell count. It would be interesting to know Vascular lesions this patient’s level of C-reactive protein, since in one Resolving infarction study of patients with cystic ring-enhancing brain Hematoma lesions, this value was elevated in nearly 80 percent of those with a brain abscess and was not elevated Thrombosed giant aneurysm in those with a brain tumor.7 Other The MRI studies in this case provide the most Radiation necrosis specific and objective path to the probable diagnoPostoperative changes sis. Many of the diseases listed in Table 1 may appear on presentation as cystic-appearing lesions 2128 n engl j med 348;21 www.nejm.org may 22 , 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved. case records of the massachusetts general hospital with surrounding ring enhancement. However, the diffusion-weighted images in this case allow us nearly to clinch the diagnosis. A lesion that has a ring of enhancement on contrast-enhanced imaging, a central core of restricted diffusion on diffusion-weighted imaging, and a thin rim of low signal on T2-weighted imaging is essentially diagnostic of a brain abscess. Table 2. Microbiologic Pathogens in Brain Abscesses, According to Major Primary Source of Infection.* Source of Infection Pathogens Paranasal sinuses Streptococcus (especially Streptococcus milleri), haemophilus, bacteroides, fusobacterium Odontogenic sources Streptococcus, bacteroides, prevotella, fusobacterium, haemophilus Otogenic sources Enterobacteriaceae, streptococcus, pseudomonas, bacteroides Lungs Streptococcus, fusobacterium, actinomyces Urinary tract Pseudomonas, enterobacter Penetrating head trauma Staphylococcus aureus, enterobacter, clostridium Neurosurgical procedure Staphylococcus, streptococcus, pseudomonas, enterobacter Endocarditis Viridans streptococcus, S. aureus Congenital cardiac malformations (especially right-to-left shunts) Streptococcus brain abscesses The spectrum of organisms found in brain abscesses reflects the range of underlying primary sources of infection. Approximately 60 percent are multimicrobial.1 A brain abscess can develop as a result of contiguous spread from the sinuses or odontogenic or otic primary sources, as a result of hematogenous spread from distant locations, or after penetration of the brain during surgery or trauma, particularly when bone fragments are retained. In 10 to 60 percent of patients with a brain abscess, no underlying source of infection is found.1,3,5 Table 2 outlines the major primary sources of infection that can lead to the development of a brain abscess. Odontogenic brain abscesses and those arising from the frontal and ethmoid sinuses have a predilection for the frontal lobe. Sphenoid sinusitis and otic infections involve a higher incidence of abscess formation in the temporal lobe than in other lobes.1,3,8 Abscesses that develop owing to hematogenous seeding from distant locations are located in proportion to regional blood flow; therefore, they occur most commonly in the area of the middle cerebral artery1,8 and are more likely to occur as multiple abscesses than as single ones. neoplasms The other major entity to be considered in this case, besides a brain abscess, is a primary or metastatic neoplasm. In particular, aggressive primary brain tumors, such as glioblastoma multiforme or anaplastic astrocytoma, as well as metastases from lung and breast cancer, can present with many of the same imaging characteristics, although a thin rim of low signal on T2-weighted images, which is thought to represent collagen, subtle hemorrhage, or macrophages containing free radicals, is more characteristic of an abscess than of a neoplasm.9,10 Over the past decade, diffusion-weighted imaging has greatly improved our ability to differentiate abscesses from other cystic, ring-enhancing brain lesions. Many recent studies have shown that this method of imaging is sensitive and specific in dif- n engl j med 348;21 * The information is adapted from Calfee and Wispelwey,1 Roos and Tyler,3 and Mathisen and Johnson.5 ferentiating abscesses from neoplasms as a cause of ring-enhancing lesions.11,12 As in this case, the central core of an abscess shows a hyperintense signal on diffusion-weighted images and a hypointense signal on apparent-diffusion-coefficient images, a finding indicating an area of restricted diffusion. Necrotic or cystic brain tumors have central areas of hypointense signal on diffusion-weighted imaging, unless there is a hemorrhagic or proteinaceous component, which may appear as an area of heterogeneous or bright signal. As Dr. Gonzalez mentioned, it appears that the increased viscosity of the fluid in an abscess, along with the hypercellularity of the inflammatory response, contributes to decreased water proton mobility and results in restriction of diffusion.12,13 conclusions The differential diagnosis in this case includes a brain abscess and a cystic neoplasm. The imaging characteristics, particularly the presence of a central core of restricted diffusion within the lesion, point convincingly to a cerebral abscess. Possible sources www.nejm.org may 22, 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2129 The new england journal of infection are suggested by the patient’s several bouts of sinusitis and the recent filling of several dental cavities. Because there is no current evidence of sinusitis, an odontogenic source is more likely. The likely organisms include one or more of the following: streptococcus (Streptococcus milleri being the most common), bacteroides, haemophilus, prevotella, and fusobacterium. The next step in this case should be image-guided, stereotactic needle aspiration of the contents of the lesion. This procedure is both diagnostic and therapeutic. The analysis and culture of the contents would confirm the diagnosis and allow tailoring of the antibiotic regimen. Drainage of the contents would decrease the infectious burden. A Physician: How do you explain the response of the patient’s fever to corticosteroids? Dr. Friedlander: Fever in patients who have brain abscesses often responds to corticosteroids. A Physician: Is the granuloma that appears on the radiograph of the chest relevant to the diagnosis? Dr. Friedlander: I think the granuloma is an incidental finding. Dr. Nancy Lee Harris: Dr. Medlock will describe the clinical thinking and the diagnostic procedure. Dr. Michael D. Medlock (Neurosurgery): We strongly suspected a brain abscess. The patient was taken to the operating room, where a Cosman–Roberts– Wells frame was attached and a contrast-enhanced CT scan was obtained. We targeted points so that we could aspirate the contents of the cyst and obtain a biopsy specimen of the cyst wall. We made a small burr hole, and the computer-guided needle was inserted into the cyst. Approximately 15 ml of fluid with the color and consistency of pus was aspirated and sent to the microbiology laboratory, and a biopsy specimen of the wall was sent for frozensection examination. of medicine pathological discussion Dr. Rolf Pfannl: We received specimens from the right frontal lobe (Fig. 3), including an aggregate of soft tissue (1 cm in diameter) and about 1.5 ml of mucoid material admixed with blood. Examination of a smear and frozen sections revealed acute inflammatory cells, macrophages, and necrotic debris. No tumor cells were found. Histologic sections stained with hematoxylin and eosin consisted predominantly of necrotic tissue with a neutrophilic infiltrate. A few viable fragments of brain contained granulation tissue. There was no evidence of tumor. A Gram’s stain revealed innumerable gram-positive cocci. The findings are those of a brain abscess of bacterial origin. A B clinical diagnosis Brain abscess. dr. robert m. friedlander’s diagnosis Pyogenic brain abscess in the right frontal lobe with an odontogenic source of infection (streptococcus [most likely Streptococcus milleri], haemophilus, bacteroides, prevotella, or fusobacterium). 2130 n engl j med 348;21 Figure 3. Biopsy Specimen of the Mass in the Right Frontal Lobe. Granulation tissue from the edge of the cavity (Panel A) contains proliferating small blood vessels, neutrophils, macrophages, and fibroblasts (hematoxylin and eosin, ¬500). Gram’s staining (Panel B) reveals numerous cocci, both singly and in clusters and short chains (Brown– Hopps stain, ¬624). www.nejm.org may 22 , 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved. case records of the massachusetts general hospital Smears prepared in the microbiology laboratory and subjected to Gram’s staining showed grampositive cocci in pairs and short chains. Cultures of the abscess contents revealed mixed flora, including S. milleri and Haemophilus aphrophilus. S. milleri is a non–group-B, beta-hemolytic organism associated with deep suppurative infections such as brain abscesses.14,15 H. aphrophilus is considered part of the normal oral flora but is occasionally associated with upper and lower respiratory tract infections; it may cause bacteremia, endocarditis, and brain or dental abscesses. The evolution of a cerebral abscess can be roughly divided into four pathologic stages.16,17 On days 1 to 2 after infection, focal suppurative encephalitis or cerebritis occurs, with swelling of endothelial cells and perivascular and parenchymal infiltration by neutrophils. Between days 2 and 7, confluent areas of necrosis develop, with a prominent infiltrate of macrophages, lymphocytes, and plasma cells. Between days 5 and 14, there is early encapsulation, with a granulation-tissue response around the margins, as in this case. After two weeks, encapsulation by a thick, collagenous wall occurs, and the necrotic center is surrounded by granulation tissue and by concentric layers of fibroblasts, reticulin fibers, collagen, and reactive glial cells. Dr. Harris: Dr. Beigel saw the patient after the diagnosis was made and will tell us about subsequent studies and follow-up. Dr. John H. Beigel (Infectious Disease): We were consulted after Gram’s staining had shown grampositive cocci in short chains and pairs. Since there was no evidence on MRI or CT scans of a contiguous focus of infection, we believed that hematogenous spread was likely and that it was probably a streptococcal species. We were concerned about pneumococcus since there were gram-positive cocci in pairs and also about the possible presence of anaerobes, since brain abscesses are often polymicrobial. The patient was initially treated with vancomycin, ceftriaxone, and metronidazole. Because of the presumed hematogenous source, we recommended an echocardiogram to look for endocarditis and a “bubble study” (echocardiography after the injection of agitated saline) to look for a patent foramen ovale. When the culture results showed S. milleri as well as H. aphrophilus, we thought that the most likely source of the infection was bacteremia due to the dental procedures. The antibiotic therapy was changed to ceftriaxone alone, which n engl j med 348;21 was given for six weeks. The patient’s symptoms and neurologic deficit resolved completely. Dr. Nadeem A. Afridi: Cardiac ultrasonography was performed to evaluate the possibility of endocarditis and the possible patent foramen ovale. There were no valvular vegetations. Two echocardiographic techniques are used to assess the presence of an interatrial communication: color Dop- A RA LA B RA LA Figure 4. Cardiac Ultrasonographic Study with Agitated Saline. A mixture of saline and air bubbles is injected intravenously and appears as a bright signal in the right atrium (RA) and ventricle between the first and second heartbeat after injection, as indicated by the bar on the rhythm strip (Panel A). One beat later, between the second and third beats after injection, the air bubbles appear in the left atrium (LA) and ventricle (Panel B), indicating the presence of a right-to-left shunt through a patent foramen ovale. (A video clip of a cardiac ultrasonographic study with agitated saline is available with the full text of this article at http://www.nejm.org.) (Images prepared with the assistance of Dr. Mary Etta King.) www.nejm.org may 22, 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2131 case records of the massachusetts general hospital pler echocardiography, which can detect a left-toright shunt across the septum, and echocardiography with intravenous agitated-saline injection, which can detect a right-to-left shunt. In the latter technique, also known as a bubble study, a small amount of air is mixed with saline and injected intravenously. The tiny air bubbles are seen as bright reflections in the right atrium. If there is an intracardiac shunt, the air bubbles will appear in the left atrium within two, three, or four heartbeats after the injection. Their appearance after five heartbeats can result from normal circulation of the air bubbles through the lung. In this patient, we saw both a leftto-right shunt on the Doppler study and a rightto-left shunt on the study with agitated-saline injection (Fig. 4 and video clip, available with the full text of this article at http://www.nejm.org), both of which are consistent with a diagnosis of patent foramen ovale. Dr. Friedlander: Three important factors contributed to the excellent outcome in this patient, who had a potentially lethal condition. The first was the expeditious and correct diagnosis of a brain abscess. The second was the prompt institution of treatment, with drainage of the abscess and administration of antibiotics. The third was the identification of any abnormalities that would predispose her to future problems, so that prophylaxis might be undertaken with subsequent dental procedures. anatomical diagnosis Brain abscess due to infection with Streptococcus milleri and Haemophilus aphrophilus. Dr. Friedlander is indebted to Jonathan Slotkin, M.D., for assistance in the preparation of the case discussion. references 1. Calfee DP, Wispelwey B. Brain abscess. 8. Infection in Neurosurgery Working Semin Neurol 2000;20:353-60. 2. Seydoux C, Francioli P. Bacterial brain abscesses: factors influencing mortality and sequelae. Clin Infect Dis 1992;15:394-401. 3. Roos KL, Tyler KL. Bacterial meningitis and other suppurative infections. In: Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s principles of internal medicine. 15th ed. Vol. 2. New York: McGraw-Hill, 2001:2462-71. 4. Youmans JR, ed. Neurological surgery: a comprehensive reference guide to the diagnosis and management of neurosurgical problems. 4th ed. Vol. 5. Philadelphia: W.B. Saunders, 1996:3205-13. 5. Mathisen GE, Johnson JP. Brain abscess. Clin Infect Dis 1997;25:763-81. 6. Schuman NJ, Turner JE. Brain abscess and dentistry: a review of the literature. Quintessence Int 1994;25:411-3. 7. Hirschberg H, Bosnes V. C-reactive protein levels in the differential diagnosis of brain abscesses. J Neurosurg 1987;67:35860. Party of the British Society for Antimicrobial Chemotherapy. The rational use of antibiotics in the treatment of brain abscess. Br J Neurosurg 2000;14:525-30. 9. Sze G, Zimmerman RD. The magnetic resonance imaging of infections and inflammatory diseases. Radiol Clin North Am 1988; 26:839-59. 10. Haimes AB, Zimmerman RD, Morgello S, et al. MR imaging of brain abscesses. AJR Am J Roentgenol 1989;152:1073-85. 11. Desprechins B, Stadnik T, Koerts G, Shabana W, Breucq C, Osteaux M. Use of diffusion-weighted MR imaging in differential diagnosis between intracerebral necrotic tumors and cerebral abscesses. AJNR Am J Neuroradiol 1999;20:1252-7. 12. Kim YJ, Chang KH, Song IC, et al. Brain abscess and necrotic or cystic brain tumor: discrimination with signal intensity on diffusion-weighted MR imaging. AJR Am J Roentgenol 1998;171:1487-90. 13. Krabbe K, Gideon P, Wagn P, Hansen U, Thomsen C, Madsen F. MR diffusion imag- ing of human intracranial tumours. Neuroradiology 1997;39:483-9. 14. Tunkel AR, Wispelwey B, Scheld WM. Brain abscess. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. 5th ed. Vol. 1. Philadelphia: Churchill Livingstone, 2000:1016-28. 15. Molina JM, Leport C, Bure A, Wolff M, Michon C, Vilde JL. Clinical and bacterial features of infections caused by Streptococcus milleri. Scand J Infect Dis 1991;23:659-66. 16. Gray F, Alonso J-M. Bacterial infections of the central nervous system. In: Graham DI, Lantos PL, eds. Greenfield’s neuropathology. Vol. 2. London: Arnold, 2002:16770. 17. Brain abscess. In: Ellison D, Love S, Chimelli L, et al. Neuropathology: a reference text of CNS pathology. London: Mosby, 1998:15.6–15.8. Copyright © 2003 Massachusetts Medical Society. 35-millimeter slides for the case records Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a medical teaching exercise or reference material is eligible to receive 35-mm slides, with identifying legends, of the pertinent x-ray films, electrocardiograms, gross specimens, and photomicrographs of each case. The slides are 2 in. by 2 in., for use with a standard 35-mm projector. These slides, which illustrate the current cases in the Journal, are mailed from the Department of Pathology to correspond to the week of publication and may be retained by the subscriber. Each year approximately 250 slides from 40 cases are sent to each subscriber. The cost of the subscription is $450 per year. Application forms for the current subscription year, which began in January, may be obtained from Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974). Slides from individual cases may be obtained at a cost of $35 per case. 2132 n engl j med 348;21 www.nejm.org may 22 , 2003 Downloaded from www.nejm.org on February 23, 2005 . This article is being provided free of charge for use in Cuba. Copyright © 2003 Massachusetts Medical Society. All rights reserved.