Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
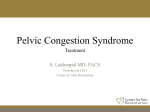
ORIGINAL ARTICLE Splenic Vein–Inferior Mesenteric Vein Anastomosis to Lessen Left-Sided Portal Hypertension After Pancreaticoduodenectomy With Concomitant Vascular Resection Nélio Ferreira, MD; Elie Oussoultzoglou, MD; Pascal Fuchshuber, MD, PhD; Dimitrios Ntourakis, MD; Masato Narita, MD, PhD; Mudassir Rather, MD; Edoardo Rosso, MD; Pietro Addeo, MD; Patrick Pessaux, MD, PhD; Daniel Jaeck, MD, PhD, FRCS; Philippe Bachellier, MD, PhD Hypothesis: A splenic vein (SV)–inferior mesenteric vein (IMV) anastomosis reduces congestion of the stomach and spleen after pancreaticoduodenectomy with resection of the SV–mesenteric vein confluence but carries a risk of left-sided venous hypertension. Design: Comparative retrospective study. Setting: Department of Digestive Surgery and Trans- plantation, University of Strasbourg, Strasbourg, France. Patients: From January 1, 2002, to February 28, 2010, 39 patients underwent pancreaticoduodenectomy with resection of the SV–mesenteric vein confluence for pancreatic adenocarcinoma. All patients had a terminoterminal portalvein–superiormesentericveinanastomosis.TheSVblood flow into the portal vein was preserved in 11 patients by reimplantation of the SV into the portal vein. Sixteen patients underwent surgical reconstruction of the SV-IMV confluence by anastomosis (group 1), and in 12 patients the natural SV-IMV confluence was preserved (group 2). Main Outcome Measures: Preoperative and postoperative spleen volume and platelet count. Author Affiliations: Centre de Chirurgie Viscérale et de Transplantation, Hôpital de Hautepierre, Hôpitaux Universitaires de Strasbourg, Strasbourg, France (Drs Ferreira, Oussoultzoglou, Ntourakis, Narita, Rather, Rosso, Addeo, Pessaux, Jaeck, and Bachellier); and Department of Surgical Oncology, Permanente Medical Group, Walnut Creek, California (Dr Fuchshuber). R Results: Demographic characteristics, preoperative tumor staging, pathological outcome, and postoperative complications were comparable in both groups. There was no difference in platelet count between groups 1 and 2 preoperatively (mean [SD], 293.13 [125.37] vs 241.09 [49.12] ⫻ 103/µL [to convert to ⫻109/L, multiply by 1.0], respectively; P = .21) or postoperatively (mean [SD], 231.75 [156.39] vs 164.31 [76.46]⫻ 103/ µL, respectively; P = .32). Likewise, no difference was found in the spleen volume preoperatively (mean [SD], 258.96 [179.23] vs 237.31 [122.46] mL, respectively; P = .76) and on postoperative day 15 (mean [SD], 279.08 [158.10] vs 299.12 [153.11] mL, respectively; P =.78). Conclusion: Early assessment shows that SV-IMV anas- tomosis is as feasible and as safe as the preservation of a natural SV-IMV confluence in patients undergoing pancreaticoduodenectomy with vascular resection for pancreatic head adenocarcinoma. Arch Surg. 2011;146(12):1375-1381 ADICAL SURGERY REMAINS the only curative treatment of pancreatic cancer.1-3 Portal vein (PV) and superior mesenteric vein (SMV) invasion is often present because of the close relationship between these vessels and the pancreatic head as well as the See Invited Critique at end of article uncinate process.4 For a long time, venous invasion was considered a contraindication to surgery. Recently, however, extensive vascular resection has gained acceptance as it has been shown to improve the rates of R0 resection and surARCH SURG/ VOL 146 (NO. 12), DEC 2011 1375 vival5 without an increase in postoperative morbidity and mortality.6 Resection or division of the splenic vein (SV) has been performed not only in cases of vascular tumor invasion but also to achieve a complete lymph node and neural dissection around the superior mesenteric artery (SMA).7 Potential risks of the procedure include segmental left-sided venous hypertension with resulting splenomegaly, hypertensive gastropathy, esophageal varices, and hemorrhage. When resection of the mesenteric vein–PV confluence or division of the SV is performed during pancreatic head resection, the presence of a natural SV– inferior mesenteric vein (IMV) confluence can preserve the venous drainage of the spleen and the gastric remnant and ob- WWW.ARCHSURG.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/surg/22575/ on 04/28/2017 A PV SV SMV 11 Patients B PV SV IMV SMV tients (4.7%) had partial lateral venorrhaphy and 81 (95.3%) had segmental venous resection, including PV resection in 12 patients, SMV resection in 30 patients, and SV–mesenteric vein confluence resection in 39 patients with direct venovenous anastomosis without interposition. Figure 1 summarizes the vascular reconstruction after resection of the SV–mesenteric vein confluence. Among these 39 patients, 11 received an end-toend anastomosis between the PV and the neoconfluence of the SMV and SV (Figure 1A). These cases were excluded, leaving a study population of 28 patients who underwent end-to-end anastomosis between SMV and PV with either additional endto-end anastomosis between the SV and the IMV (group 1; n=16) (Figure 1B) or preservation of a natural SV-IMV confluence (group 2; n=12) (Figure 1C). The patients’ characteristics, preoperative imaging of venous invasion, preoperative serum tumor markers, preoperative biliary drainage, neoadjuvant treatment, blood transfusion, postoperative mortality and morbidity including patency of the SV-IMV anastomosis, and histological results (venous tumor invasion, specimen margin invasion, TNM classification) were collected from the medical records. 16 Patients (Group 1) SURGICAL TECHNIQUES C PV SV SMV IMV 12 Patients (Group 2) Figure 1. Vascular reconstruction after resection of the splenic vein (SV)–mesenteric vein confluence. Eleven patients received an end-to-end anastomosis between the portal vein (PV) and the neoconfluence of the superior mesenteric vein (SMV) and SV and were excluded from analysis (A); the remaining 28 patients underwent end-to-end anastomosis between the SMV and PV with either additional end-to-end anastomosis between the SV and the inferior mesenteric vein (IMV) (group 1; n=16) (B) or preservation of a natural SV-IMV confluence (group 2; n=12) (C). viates the need for an additional anastomosis between the SV and the PV.7,8 A natural SV-IMV confluence is absent in about 30% of patients as the IMV drains either directly into the SMV or into the SV-SMV confluence.9 In those cases or when a natural SV-IMV confluence cannot be preserved for technical reasons, construction of an SV-IMV anastomosis may be of value to preserve splenic and gastric venous drainage. The aim of this study is to evaluate the feasibility and function of an SV-IMV anastomosis during pancreaticoduodenectomy with SV–mesenteric vein confluence resection. METHODS STUDY POPULATION Between January 1, 2002, and February 28, 2010, a total of 195 patients underwent a curative-intent pancreaticoduodenectomy for pancreatic head adenocarcinoma. Of these, 85 (43.5%) with locally advanced disease had mesenteric vein–PV resection and reconstruction as part of their procedure. Four pa- All patients underwent a standard Whipple pancreaticoduodenectomy without pylorus preservation and extended lymph node dissection including the hepatic hilum, common hepatic artery, celiac trunk, SMA, and para-aortic area above the left renal vein. Intraoperative pathological analysis of the pancreatic margin was obtained in all cases. Technical highlights include the following: (1) early dissection of the origin of the SMA above the left renal vein followed by sectioning of the retroportal pancreatic lamina10 to facilitate venous resection; (2) complete mobilization of the surgical specimen before removing the involved venous segment; and (3) concomitant clamping of the SMA during venous resection to prevent excessive intestinal congestion11 prior to enteric anastomosis. The anastomosis between the SMV and PV was fashioned using a 6-0 nonabsorbable running suture impregnated with a growth factor. To facilitate a tension-free vascular anastomosis without graft interposition, the right colon and the root of the mesentery were completely mobilized.12 End-to-end anastomosis between the SV and IMV was performed using an 8-0 nonabsorbable running suture. If the SV-IMV confluence was preserved, the SV was ligated distally to this confluence (Figure 1C). A 2-layer telescoped pancreaticogastrostomy was routinely used as previously reported.13 The reconstruction was completed by an endto-side choledochojejunostomy and a transmesocolic end-toside gastrojejunostomy. DEFINITION OF POSTOPERATIVE COMPLICATIONS Postoperative complications were given Clavien classifications.14 Pancreatic fistula was defined as a drain output with an amylase content greater than 3 times the serum amylase activity on or after postoperative day 3, according to the International Study Group on Pancreatic Fistula.15 Delayed gastric emptying was defined as the inability to return to a standard diet by the end of the first postoperative week, including prolonged nasogastric intubation, according to the International Study Group of Pancreatic Surgery.16 MAIN OUTCOME MEASURES All patients underwent computed tomography (CT) around postoperative day 15, and the venous anastomosis outflow was ARCH SURG/ VOL 146 (NO. 12), DEC 2011 1376 WWW.ARCHSURG.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/surg/22575/ on 04/28/2017 evaluated. The occurrence of left-sided portal hypertension was evaluated in both groups before and after surgery by assessing the platelet count and spleen volume according to the Cavalieri method.17 In brief, the spleen surface was measured with manual contouring on digitized CT using ImageJ version 1.42q software (National Institutes of Health, Bethesda, Maryland). Final spleen volume was calculated by adding all CT slices showing the spleen.18 STATISTICAL ANALYSIS All values are expressed as mean (standard deviation). Pearson 2 test and independent t test were used appropriately. A difference was considered significant at P⬍.05. Statistical analyses were performed using SPSS for Windows version 10.0 statistical software (SPSS Inc, Chicago, Illinois). RESULTS PATIENTS AND SURGICAL CHARACTERISTICS There were 20 men and 8 women. Their mean (SD) age was 63.2 (8.0) years (range, 43-80 years). The American Society of Anesthesiologists scores were 1 in 9 patients, 2 in 18 patients, and 3 in 1 patient. The mean (SD) body mass index (calculated as weight in kilograms divided by height in meters squared) for all patients was 24.6 (3.5) (range, 16.6-31.9). Twenty-one patients had preoperative weight loss ranging from 1.98 to 15.84 kg (mean [SD], 6.84 [3.56] kg), and 6 patients received preoperative enteral nutritional support with -3 fatty acids, arginine, ribonucleic acid, and soluble fiber (Oral Impact, Nestlé HealthCare Nutrition, Inc, Florham Park, New Jersey). Preoperative biliary drainage was performed in 9 patients who presented with a total serum bilirubin level higher than 11.69 mg/dL (to convert to micromoles per liter, multiply by 17.104). Evaluation of vascular involvement was performed using the Nakao classification,19 with 6 patients showing grade A (normal), 11 patients grade B (unilateral narrowing), 10 patients grade C (bilateral narrowing), and 1 patient grade D (venous obstruction and collateral circulation). The CA 19-9 serum level was elevated in 19 patients, with a mean (SD) level of 772 (1327) kU/L (range, 48-6120 kU/L). Eight patients had gemcitabine hydrochloride–based neoadjuvant chemotherapy with (n=5) or without (n=3) oxaliplatin. Twenty patients received intraoperative red blood cell transfusion (mean [SD], 4.4 [2.8] units transfused). PATHOLOGICAL RESULTS The mean (SD) tumor size was 38.5 (13.6) mm (range, 15-70 mm). Tumor emboli within lymphatic and vascular spaces were encountered in 3 patients, and perineural invasion occurred in 18 patients. The mean (SD) numbers of overall dissected and involved lymph nodes were 35.7 (14.2) (range, 6-74) and 5.7 (10.3) (range, 1-50), respectively. Pathological analysis of the specimen showed that the mesenteric vein–PV wall was involved in 18 patients. The depth of invasion was limited to the adventitia in 4 patients, involved the tunica media in 7, and reached the intima in 7. An R0 resection was achieved in 18 patients (64.2%). Ten patients had microscopic positive margins (R1 resection) including the retroperitoneal margin alone (n = 5), the pancreatic stump alone (n=3), and both the pancreatic stump and either the retroperitoneal margin (n=1) or PV (n=1). According to the American Joint Committee on Cancer staging system, tumor was classified as pT1N0 (stage I) in 2 patients, T3N0 (stage IIA) in 4 patients, T3N1 (stage IIB) in 16 patients, T4N1 (stage III) in 1 patient, and metastatic disease (stage IV) in distant lymph nodes in 5 patients. EARLY POSTOPERATIVE OUTCOME Complications included 1 cardiac complication managed with oral medications (Clavien grade II), 2 pancreatic fistulas treated successfully with octreotide acetate (Clavien grade II), 2 cases of delayed gastric emptying treated with prokinetic drugs (Clavien grade II), 1 case of chylous ascites treated with diuretics (Clavien grade II), 1 SV thrombosis treated with anticoagulation therapy (Clavien grade II), 1 intra-abdominal abscess treated by percutaneous drainage (Clavien grade IIIA), 2 reoperations (Clavien grade IIIB), and 2 in-hospital deaths within 30 days of surgery (Clavien grade V). Both reoperations were because of postoperative hemorrhage: one for active abdominal bleeding from a branch of a midcolonic artery on the second postoperative day and the other for upper gastrointestinal tract bleeding from the pancreatic stump on postoperative day 7. Attempts at endoscopic treatment had failed and the patient required a salvage total pancreatosplenectomy. The first postoperative death was caused by severe sepsis of undetermined origin 15 days after surgery. The second surgical mortality was due to massive intra-abdominal hemorrhage complicating a pancreatic fistula on postoperative day 25. EVALUATION OF LEFT-SIDED VENOUS HYPERTENSION The mean (SD) preoperative and postoperative (day 30) platelet counts were 271.11 (102.24) and 200.13 (126.33) ⫻ 103/µL (to convert to ⫻109/L, multiply by 1.0), respectively. The mean (SD) preoperative and postoperative (day 15) spleen volumes were 249.22 (152.78) and 288.10 (152.09) mL, respectively. COMPARABILITY OF BOTH GROUPS As shown in Table 1, there were no differences between both groups regarding sex, age, American Society of Anesthesiologists classification, body mass index, preoperative weight loss, degree of preoperative venous invasion, level of tumor markers (CA 19-9 level), preoperative biliary drainage, neoadjuvant chemotherapy, and intraoperative blood transfusions. The final pathological examination of the resected specimens in both groups showed no differences regarding tumor size, presence of microvascular emboli and perineural invasion, numbers of dissected and involved lymph nodes, presence and depth of PV invasion, number and site of positive surgical margins, and TNM classification (Table 2 and ARCH SURG/ VOL 146 (NO. 12), DEC 2011 1377 WWW.ARCHSURG.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/surg/22575/ on 04/28/2017 Table 1. Demographic and Surgical Characteristics Characteristic Sex, No. Male Female Age, mean (SD), y ASA score, No. 1 2 3 BMI, mean (SD) Preoperative weight loss, No. Yes No Nakao classification of preoperative venous involvement, No. A B C D Elevated CA 19-9 level, No. Yes No Preoperative biliary drainage, No. Yes No Neoadjuvant chemotherapy, No. Yes No Received blood transfusion, No. Yes No RBC units transfused, mean (SD) Group 1 (n = 16) Group 2 (n = 12) 11 5 63.0 (9.0) 9 3 63.5 (6.9) 4 12 0 24.6 (4.0) 5 6 1 24.5 (2.9) 13 3 8 4 Table 2. Pathological Data P Value Variable .72 Tumor size, mean (SD), mm Microvascular emboli, No. Yes No Perineural invasion, No. Yes No Dissected lymph nodes, mean (SD), No. Involved lymph nodes, mean (SD), No. Portal vein infiltration, No. No Yes Depth of venous wall invasion, No. a Adventitia Tunica media Intima Resection margin, No. R0 R1 Site of positive margin, No. b Pancreas Retroperitoneum Pancreas and retroperitoneum Pancreas and portal vein .94 .27 .96 .38 .82 3 6 6 1 3 5 4 0 9 7 10 2 6 10 3 9 6 10 2 10 11 5 5.0 (2.8) 9 3 3.7 (2.9) .13 .48 .23 .72 Group 1 (n = 16) Group 2 (n = 12) P Value 39.7 (14.0) 37.1 (13.7) .49 .38 1 15 2 10 11 5 38.1 (15.6) 7 5 32.8 (12.4) .97 7.4 (13.3) 3.4 (2.6) .87 5 11 5 7 2 4 5 2 3 2 10 6 8 4 1 4 1 0 2 1 0 1 .57 .57 .75 .82 .27 a Eighteen patients had pathological venous involvement. b Ten patients had positive resection margins. .96 Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); RBC, red blood cell. Table 3). There were no differences in postoperative complications between both groups (Table 4). OCCURRENCE OF LEFT-SIDED PV HYPERTENSION [179.23] vs 279.08 [158.10] mL, respectively; P = .40; group 2: mean [SD], 237.31 [122.46] vs 299.12 [153.11] mL, respectively; P=.16). Furthermore, postoperative CT showed patency of venous reconstruction (Figure 2) in all patients except 1 patient from group 2 who developed SV thrombosis. Nevertheless, the thrombosis was partial, there was no significant change in the spleen size, and later CT showed complete recovery following anticoagulation therapy. COMMENT Between both groups (group 1 vs group 2), there was no difference in the platelet count preoperatively (mean [SD], 293.13 [125.37] vs 241.09 [49.12] ⫻ 103/µL, respectively; P = .21) or postoperatively (mean [SD], 231.75 [156.39] vs 164.31 [76.46]⫻103/µL, respectively; P=.32). Within group 2, the platelet count was significantly lower after surgery compared with the preoperative count (mean [SD], 164.31 [76.46] vs 241.09 [49.12]⫻103/µL, respectively; P=.02). In contrast, there was no difference within group 1 between the preoperative and postoperative platelet counts (mean [SD], 293.13 [125.37] vs 231.75 [156.39]⫻103/µL, P=.32). Between groups 1 and 2, there was also no difference in the preoperative and postoperative splenic volume (before surgery: mean [SD], 258.96 [179.23] vs 237.31 [122.46], respectively; P = .76; postoperative day 15: mean [SD], 279.08 [158.10] vs 299.12 [153.11] mL, respectively; P=.78). Splenic volume showed no difference within each group on preoperative vs postoperative measurement (group 1: mean [SD], 258.96 This comparative retrospective study demonstrated the safety of an SV-IMV anastomosis during pancreaticoduodenectomy with resection of the mesenteric vein–PV confluence. We did not observe additional specific vascularrelated postoperative complications from adding the SV-IMV anastomosis to the procedure. The lack of a significant decrease in platelet count and the lack of a significant increase in spleen volume between both groups before and after surgery suggest a protective function of SV-IMV anastomosis from left-sided portal hypertension. Although a significant difference between preoperative and postoperative platelet counts was seen within group 2, complications due to left-sided portal hypertension did not occur. Pancreaticoduodenectomy has been regarded as the standard operation for pancreatic head carcinoma and can be performed safely with a mortality of 0.7% to 3% and a morbidity of 36% to 41% in high-volume cen- ARCH SURG/ VOL 146 (NO. 12), DEC 2011 1378 WWW.ARCHSURG.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/surg/22575/ on 04/28/2017 Table 3. Tumor TNM Classification According to the American Joint Committee on Cancer Patients, No. TNM Classification Stage Group 1 I IIA IIB III IV 2 1 10 1 2 T1N0 T3N0 T3N1 T4N1 T3N1M1 P Value Group 2 0 3 6 0 3 .32 Table 4. Clavien Classification of Postoperative Complications Patients, No. Clavien Grade II IIIA IIIB IV V Group 1 2 1 1 0 2 Group 2 5 0 1 0 0 P Value .23 PV SV IMV ters.20,21 Radical resection is the single most important factor determining outcome in these patients.2 To achieve R0 resection, resection of the PV and/or SMV is necessary in 10% to 20% of cases and can be done successfully without increase in morbidity and mortality.1,6,22,23 It has been reported that venous resection provides the same overall survival if it is R0 resection.5,13,24,25 Our policy is to perform venous resection in all cases with preoperative or intraoperative suspicion of venous involvement, without dissection along the vein, to avoid tumor dissemination. Suspicion or diagnosis of vascular invasion is currently best assessed by CT.26 In this series, it occurred in 22 patients (78.6%). The degree of venous invasion was evaluated according to the Nakao classification,19 which assesses only the mesenteric-portal axis involvement. However, in our opinion, preoperative angiographic studies should also assess the relationship between the tumor and the SV as well as the anatomical position9 and involvement of the IMV as insufficient venous drainage of the spleen and gastric remnant can be a significant source of postoperative complications after mesenteric vein–PV confluence resection.7,27 For oncological reasons, wide vascular resection of the SV–mesenteric vein confluence including the IMV is often necessary. Division and ligation of the SV carries a theoretical risk of left-sided venous hypertension with congestion of the stomach and spleen. It may induce hypertensive gastropathy with gastric mucosal hemorrhage27 as well as gastric variceal hemorrhage. Moreover, additional ligation of the left gastric vein during lymph node dissection limits the gastric remnant drainage to the short gastric vessels. Therefore, many pancreatic surgeons avoid simple proximal ligation of the SV. If the SV is ligated without reconstruction, the presence of a natural SV-IMV confluence may provide sufficient venous drainage of the spleen and gastric remnant. The SMV Figure 2. Representative postoperative computed tomographic scan of a group 2 patient showing patent splenic vein (SV)–inferior mesenteric vein (IMV) reconstruction. PV indicates portal vein; SMV, superior mesenteric vein. need for SV reconstruction is not universally accepted because the venous drainage of the spleen and stomach may reach the systemic circulation by drainage through esophageal veins.28 If the SV-IMV confluence is absent or impossible to preserve, drainage of the SV may be reestablished by construction of an anastomosis between the SV and IMV to mitigate or completely avoid leftsided portal hypertension. In 1997, Tamura et al8 reported 4 cases of SV-IMV anastomosis or preservation of a natural SV-IMV confluence following pylorus-preserving pancreaticoduodenectomy for pancreatic cancer. Postoperative angiographic studies showed adequate venous drainage from the spleen and stomach into the portal circulation in all cases. In 2005, Misuta et al7 used the same technique in 12 cases. Most patients again demonstrated adequate venous drainage of the spleen and stomach. Reversal of venous flow toward the spleen was seen in only 3 patients (25%), 2 of whom developed splenomegaly and venous dilata- ARCH SURG/ VOL 146 (NO. 12), DEC 2011 1379 WWW.ARCHSURG.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/surg/22575/ on 04/28/2017 tion on postoperative CT imaging. These results raised concerns about the safety of this anastomosis in some patients. However, Misuta and colleagues did not mention the preoperative degree of venous invasion. It is possible that those patients might have already had some degree of left-sided portal hypertension prior to the operation. In the presence of severe preoperative venous stenosis or occlusion due to tumor involvement, established collateral circulation may provide drainage of the spleen and part of the stomach. In such cases, we do not advocate construction of SV-IMV anastomosis. Several methods are available to assess the immediate functionality of an SV-IMV anastomosis. They include clinical observation of the decrease of the gastric congestion and color Doppler ultrasonography7 to demonstrate anastomotic patency and direction of venous blood flow. The low rate of delayed gastric emptying, successfully managed with medication, suggests that there were no additional negative effects on the postoperative gastric motility. Although feasible and reproducible, SV-IMV anastomosis may not be possible in all cases, for example, in the presence of a very short SV stump. In these cases, an interposition graft can be used29 either with an autologous vein (internal jugular, superficial femoral, gonadal, left renal, saphenous) or with prosthetic material. Venous grafts may require a second incision and increase the operative time. Prosthetic material may not be a good option in a contaminated and potentially infected operative field and carries a lower patency rate.11 Distal splenic-renal shunt has also been advocated by some authors.30 If SV-IMV anastomosis is not possible, we try to avoid the use of interposition graft by constructing an anastomosis between the right gastroepiploic vein and the IMV. Before division of the stomach, the right gastroepiploic vein is dissected and divided close to the pylorus along with the greater omentum. This anastomosis, however, is often performed at the end of the operation after completion of the gastroenteric anastomosis to avoid tension or kinking. The decrease in the platelet count in the SV-IMV confluence preservation group suggests the presence of some degree of hypersplenism. The occurrence of 1 case of postoperative SV thrombosis in this group suggests that the confluence was not always functional. We hypothesize venous traumatic injury31 as the possible cause of this complication and stress the importance of careful dissection and meticulous use of vascular surgical techniques. The routine use of concomitant clamping of the SMA during venous resection and reconstruction helps to decrease intestinal complications and reperfusion injury.11 Prolonged venous clamping of the main intestinal venous outflow can cause venous splanchnic stasis and subsequent intestinal ischemia, coagulopathy, and hemodynamic instability after declamping. Arterial clamping prevents intestinal venous congestion and thus facilitates biliary and gastric reconstruction. Finally, the main limitations of this study are the short period of observation and the use of surrogate markers for the development of sinistral portal hypertension including platelet count and splenic volume.32,33 However, invasive measurements of portal pressure are not routinely used in this clinical setting. Among noninvasive methods, both spleen volume and platelet count are currently considered to be accurate predictive markers of portal hypertension and the grade of hepatic sinusoidal injury, especially in patients treated with oxaliplatinbased chemotherapy.34,35 In conclusion, our data suggest that the SV-IMV anastomosis combined with venous resection in pancreaticoduodenectomy for pancreatic adenocarcinoma is feasible, safe, and functional as it promotes venous drainage of the spleen and gastric remnant. Accepted for Publication: July 19, 2011. Correspondence: Philippe Bachellier, MD, PhD, Centre de Chirurgie Viscérale et de Transplantation, Hôpital de Hautepierre, Hôpitaux Universitaires de Strasbourg, Avenue Molière, 67098 Strasbourg CEDEX, France (philippe [email protected]). Author Contributions: Study concept and design: Oussoultzoglou and Fuchshuber. Acquisition of data: Ferreira and Ntourakis. Analysis and interpretation of data: Ferreira, Oussoultzoglou, Fuchshuber, Narita, Rather, Rosso, Addeo, Pessaux, Jaeck, and Bachellier. Drafting of the manuscript: Ferreira, Oussoultzoglou, Ntourakis, and Rather. Critical revision of the manuscript for important intellectual content: Oussoultzoglou, Fuchshuber, Narita, Rosso, Addeo, Pessaux, Jaeck, and Bachellier. Statistical analysis: Oussoultzoglou, Ntourakis, and Narita. Study supervision: Oussoultzoglou, Fuchshuber, Addeo, Jaeck, and Bachellier. Financial Disclosure: None reported. REFERENCES 1. Hartel M, Wente MN, Di Sebastiano P, Friess H, Büchler MW. The role of extended resection in pancreatic adenocarcinoma: is there good evidence-based justification? Pancreatology. 2004;4(6):561-566. 2. Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Büchler MW. Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. Br J Surg. 2004;91(5):586-594. 3. Varadhachary GR, Tamm EP, Abbruzzese JL, et al. Borderline resectable pancreatic cancer: definitions, management, and role of preoperative therapy. Ann Surg Oncol. 2006;13(8):1035-1046. 4. Tseng JF, Tamm EP, Lee JE, Pisters PW, Evans DB. Venous resection in pancreatic cancer surgery. Best Pract Res Clin Gastroenterol. 2006;20(2):349364. 5. Riall TS, Cameron JL, Lillemoe KD, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 3: update on 5-year survival. J Gastrointest Surg. 2005;9(9):1191-1206. 6. Glanemann M, Shi B, Liang F, et al. Surgical strategies for treatment of malignant pancreatic tumors: extended, standard or local surgery? World J Surg Oncol. 2008;6:123-133. 7. Misuta K, Shimada H, Miura Y, et al. The role of splenomesenteric vein anastomosis after division of the splenic vein in pancreatoduodenectomy. J Gastrointest Surg. 2005;9(2):245-253. 8. Tamura K, Sumi S, Koike M, Yano S, Nagami H, Nio Y. A splenic-inferior mesenteric venous anastomosis prevents gastric congestion following pylorus preserving pancreatoduodenectomy with extensive portal vein resection for cancer of the head of the pancreas. Int Surg. 1997;82(2):155-159. 9. Sakaguchi T, Suzuki S, Morita Y, et al. Analysis of anatomic variants of mesenteric veins by 3-dimensional portography using multidetector-row computed tomography. Am J Surg. 2010;200(1):15-22. 10. Pessaux P, Regenet N, Arnaud JP. Resection of the retroportal pancreatic lamina during a cephalic pancreaticoduodenectomy: first dissection of the superior mesenteric artery. Ann Chir. 2003;128(9):633-636. 11. Smoot RL, Christein JD, Farnell MB. Durability of portal venous reconstruction ARCH SURG/ VOL 146 (NO. 12), DEC 2011 1380 WWW.ARCHSURG.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/surg/22575/ on 04/28/2017 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. following resection during pancreaticoduodenectomy. J Gastrointest Surg. 2006; 10(10):1371-1375. Fujisaki S, Tomita R, Fukuzawa M. Utility of mobilization of the right colon and the root of the mesentery for avoiding vein grafting during reconstruction of the portal vein. J Am Coll Surg. 2001;193(5):576-578. Bachellier P, Nakano H, Oussoultzoglou PD, et al. Is pancreaticoduodenectomy with mesentericoportal venous resection safe and worthwhile? Am J Surg. 2001; 182(2):120-129. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-213. Bassi C, Dervenis C, Butturini G, et al; International Study Group on Pancreatic Fistula Definition. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005;138(1):8-13. Wente MN, Bassi C, Dervenis C, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery. 2007;142(5):761-768. Roberts N, Puddephat MJ, McNulty V. The benefit of stereology for quantitative radiology. Br J Radiol. 2000;73(871):679-697. Dello SA, van Dam RM, Slangen JJ, et al. Liver volumetry plug and play: do it yourself with ImageJ. World J Surg. 2007;31(11):2215-2221. Nakao A, Harada A, Nonami T, Kaneko T, Inoue S, Takagi H. Clinical significance of portal invasion by pancreatic head carcinoma. Surgery. 1995;117(1):5055. Reddy SK, Tyler DS, Pappas TN, Clary BM. Extended resection for pancreatic adenocarcinoma. Oncologist. 2007;12(6):654-663. Bahra M, Neumann U. Surgical techniques for resectable pancreatic cancer. Recent Results Cancer Res. 2008;177:29-38. Schäfer M, Müllhaupt B, Clavien PA. Evidence-based pancreatic head resection for pancreatic cancer and chronic pancreatitis. Ann Surg. 2002;236(2):137148. Leach SD, Lee JE, Charnsangavej C, et al. Survival following pancreaticoduodenectomy with resection of the superior mesenteric-portal vein confluence for adenocarcinoma of the pancreatic head. Br J Surg. 1998;85(5):611-617. 24. Nakao A, Takeda S, Sakai M, et al. Extended radical resection vs standard resection for pancreatic cancer: the rationale for extended radical resection. Pancreas. 2004;28(3):289-292. 25. Nakao A, Takeda S, Inoue S, et al. Indications and techniques of extended resection for pancreatic cancer. World J Surg. 2006;30(6):976-984. 26. Vargas R, Nino-Murcia M, Trueblood W, Jeffrey RB Jr. MDCT in pancreatic adenocarcinoma: prediction of vascular invasion and resectability using a multiphasic technique with curved planar reformations. AJR Am J Roentgenol. 2004; 182(2):419-425. 27. Cusack JC Jr, Fuhrman GM, Lee JE, Evans DB. Managing unsuspected tumor invasion of the superior mesenteric-portal venous confluence during pancreaticoduodenectomy. Am J Surg. 1994;168(4):352-354. 28. Fortner JG. Technique of regional subtotal and total pancreatectomy. Am J Surg. 1985;150(5):593-600. 29. Tseng JF, Raut CP, Lee JE, et al. Pancreaticoduodenectomy with vascular resection: margin status and survival duration. J Gastrointest Surg. 2004;8(8): 935-950. 30. Maillard JN, Le Baleur A, Hay JM, Desvignes G, Rodary M. Resections of the portal vein: anatomical basis, clinical results. Chirurgie. 1975;101(11):871876. 31. Carrère N, Sauvanet A, Goere D, et al. Pancreaticoduodenectomy with mesentericoportal vein resection for adenocarcinoma of the pancreatic head. World J Surg. 2006;30(8):1526-1535. 32. Köklü SE, Yüksel OS, Arhan ME, et al. Report of 24 left-sided portal hypertension cases: a single-center prospective cohort study. Dig Dis Sci. 2005;50(5): 976-982. 33. Itzchak Y, Glickman MG. Splenic vein thrombosis in patients with a normal size spleen. Invest Radiol. 1977;12(2):158-163. 34. Dib N, Konate A, Oberti F, Calès P. Non-invasive diagnosis of portal hypertension in cirrhosis: application to the primary prevention of varices. Gastroenterol Clin Biol. 2005;29(10):975-987. 35. Overman MJ, Maru DM, Charnsangavej C, et al. Oxaliplatin-mediated increase in spleen size as a biomarker for the development of hepatic sinusoidal injury. J Clin Oncol. 2010;28(15):2549-2555. INVITED CRITIQUE Safety and Effectiveness of Splenic Vein to Inferior Mesenteric Vein Anastomosis During Pancreaticoduodenectomy R adical resection is currently regarded as the standard operation for pancreatic cancer. Unfortunately, in 10% to 20% of patients, extension beyond the pancreas to involve contiguous major vascular structures limits respectability and possible cure. Extending the scope of the operation to include segments of the PV and/or SMV has proved to be safe, and immediate reconstruction is feasible using well-established vascular surgical techniques. In some instances, resection of the SV–mesenteric vein confluence including the IMV is necessary to achieve an R0 resection. If the SV-IMV confluence remains intact, venous outflow from the spleen is preserved, thereby avoiding the potential development of left-sided portal hypertension and hypertensive gastropathy and/or gastric variceal hemorrhage. Ferreira et al1 have nicely demonstrated that if preservation of the SV-IMV confluence is not possible, direct anastomosis between the remaining SV and IMV segments is both feasible and safe. Furthermore, they have demon- strated short-term anastomotic patency using clinical observation of gastric venous congestion as well as color Doppler ultrasonography. The main limitations of the study are the short observation and the use of surrogate markers (platelet count and spleen volume) to assess gastric venous hypertension. While the validity of these surrogate markers of portal hypertension has been documented in patients with chemotherapy-induced hepatic sinusoidal injury and generalized portal hypertension, it is not clear whether they are equally applicable or reliable in the setting of pure left-sided portal hypertension. Other areas of concern involve the indications for and the success of such extended venous resections. Twothirds of their patients who underwent venous resection had pathological venous involvement, and tumor involved the deeper aspects (tunica media and/or intima) of the vein wall in 60% of these patients. It has been shown elsewhere that deep invasion of the vein wall carries the same dismal prognosis as noncurative resection. More- ARCH SURG/ VOL 146 (NO. 12), DEC 2011 1381 WWW.ARCHSURG.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/surg/22575/ on 04/28/2017