Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
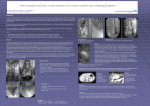
Pelvic Congestion Syndrome Treatment S. Lakhanpal MD, FACS President & CEO Center for Vein Restoration Center for Vein Restoration has forty centers mostly in the Mid-Atlantic and the NE, providing state of the art vascular care in a compassionate and cost efficient manner in the outpatient setting. Center for Vein Restoration Maryland/Virginia/DC Offices FREDRICK OWINGS MILLS CATONSVILLE HERNDON TYSONS CORNER FAIRFAX/FAIROAKS MANASSAS CVR CVM FREDRICKSBURG DC 2- VARNUM ST VIENNA Center for Vein Restoration NY, NJ, CT and PA Offices CT NY NORWALK PA STAMFORD WHITE PLAINS SCARSDALE WOODLAND PARK HACKENSACK MONTCLAIR BRISTOL NORTH BERGEN NJ CVR CVM Center for Vein Restoration Michigan Offices CVR CVM GRAND RAPIDS Treatment • • • Non Interventional – Psychotherapy – Hormonal therapy • Ovarian suppression Interventional Pelvic – TAH-BSO – Ovarian Vein Ligation – Percutaneous embolization – Internal iliac vein varicosity embolization Interventional (extra-pelvic) Perineal varicosities – Sclerotherapy – Phlebectomy Non Surgical Treatment for PVC • • • Primary goal; – Suppress ovarian function – Vasoconstriction of dilated veins. Common treatment drugs; – Progestins, danazol, Gonadotropin releasing hormone receptor agonists, phlebotonics, dihydroergotamine, NSAID’s, phsycotherapy. Medical therapy is not favored for ‘long term’ therapy because of; – Side effects • GnRH agonists (hot flashes, night sweats, vaginal dryness, mood swings). • Progestins (bloating, 5lb weight gain). • Diminishes fertility. • Adjuvant psychotherapy. – Medical therapy is not an unreasonable option for short term therapy to delay any surgical intervention. Interventional Treatments • Open Surgery – For OVR - historical purpose only. – Phlebectomy • Catheter based – Embolizations – Venoplasty – Stenting Surgery open • • • First developed by Rundqvist in the 1980s Technique – “Sympathectomy” incision – Muscle-splitting extraperitoneal approach to the ureter and adjacent ovarian vein. ligated – Suture used for traction to enable multiple ligations that finish ~ 2cm from left renal vein – Unilateral vs bilateral, based on u/s Results (72 patients -33 month f/u) – Pelvic heaviness improved in 70% of patients (in 56% almost complete) 13% little/no improvement – Dyspareunia improved in 84% (50% completed recovery) – Laparoscopic ligation also described Open surgery is now a thing of the past Patients are all treated with endovascular techniques. Catheter based: Documentation of Ovarian Vein Reflux Embolization/ Embolization + Coiling Schematic Representation of the Embolization Treatment of Iliac Vein Obstruction Venoplasty and Venous Stenting • In a clinically symptomatic patient: • Once the obstructive lesion has been identified and the degree of obstruction confirmed by IVUS(see diagnosis of PCS slides), relief of obstruction is carried out by venoplasty and venous stenting. • Currently available stents for such use are the Boston Scientific ‘wall stents’. • Multiple studies have shown the effectiveness of venous stenting in all subsets of patients inclusive of, the elderly, pre and postmenopausal, obese etc. • When placed in patients desirous of a future pregnancy, these venous stents have fared well through a subsequent pregnancy. Venous Interventions – Case Presentation • 71 yr old female • Presented with 8/10 on the pain scare -chronic painful left leg • H/O previous left leg venous ablation with minimal relief • Duplex showed stenosis of LCIV Case Study Case Study Case Study Venous Interventio – Case presentation • 34 yrs old female, severe(7/10) chronic pain in right leg with swelling , • Duplex Compression of LEIV and reflux Case Study Case Study Pregnancy After Ilio-caval Stenting • • • • • • • • • • • • • • J Vasc Surg. 2009 Aug;50(2):355-9. doi: 10.1016/j.jvs.2009.01.034. Management of pregnancy in women with previous left ilio-caval stenting. Hartung O1, Barthelemy P, Arnoux D, Boufi M, Alimi YS. Author information 1Service de Chirurgie Vasculaire, Centre Hospitalier Universitaire Nord, Marseille, France. [email protected] Abstract BACKGROUND: Ilio-caval stenting now represents the first line treatment for disabling obstructive ilio-caval lesions. Most patients are young women of child-bearing age. We herein report our experience of pregnancy in women who have a history of iliocaval stenting. MATERIALS AND METHODS: From November 1995 to April 2008, 119 patients had ilio-caval stenting for obstructive venous disease in our department. Of these, 62 women were able to become pregnant. When pregnancy occurred, they received preventive treatment with low molecular weight heparin (LMWH) from the 3rd month of pregnancy to 1 month after delivery and had to wear elastic stockings. Patients also had to sleep on their right side if possible. They were followed during the pregnancy by duplex scanning at 3, 6, and 8 months, and then 1 month after delivery. RESULTS: Eight pregnancies occurred in 6 patients (mean age 26.5 years) who had a patent self-expanding stent (1 patient had 3 pregnancies). They had stenting for May-Thurner disease in 3 patients, for post-deep venous thrombosis (DVT) left common iliac vein occlusion in 1 patient, and during venous thrombectomy in 2 patients. All stents were self-expanding metallic stents located on the left common iliac vein. One patient had unrelated spontaneous abortion after 2 months of pregnancy. No DVT or symptomatic pulmonary embolism occurred during pregnancy, delivery, or during the postpartum period. Four patients needed cesarean delivery and none had hemorrhagic complications. None of the patients had adverse effects from the treatment. Duplex scan showed compression of the stent(s) at 8 months in 4 patients with inflow obstruction in 3 patients. Postpartum duplex-scan showed no remaining stenosis in all patients. No stents had structural damage. CONCLUSION: Ilio-caval stent compression can occur during pregnancy but does not lead to structural damage to the self-expanding stents. Despite this, no cases of DVT occurred with preventive LMWH treatment Pre Procedural Care • Timing of the procedure in relation to menstrual or pain cycle is unimportant. • The patient should be restricted to clear fluids after midnight for a morning appointment, and clear fluids after breakfast for an afternoon appointment. Post Procedural Care - 1 • • • • • • Patients are instructed to avoid heavy lifting or exertion more intense than walking for 3 to 7 days post discharge. Anti-inflammatory medications are used to control post-procedural pain; oral narcotics are rarely required. The first menstrual period after embolization is often unusually heavy. Patients should be warned and reassured that this is almost invariably transient. Patients should be re-evaluated at 3 months for clinical response, at which time a trans-vaginal ultrasound to assess ovarian vein or pelvic vein reflux can be performed, providing an objective treatment assessment. Ovarian hormone levels following the procedure have been shown not to be affected. Physchological counselling must continue Post Procedural Care -2 • • Patients may describe persistent symptoms at 3months. If the presentation was chronic pelvic pain, careful questioning may reveal that symptoms have improved but have not completely resolved. It is important to temper patient expectations as many patients will have less frequent, less severe pain rather than complete symptom eradication as their ultimate outcome. Improvement of chronic pelvic pain may be delayed for more than 6 months post treatment, particularly when severe at presentation. If the patient has persistent, unimproved pain at 6 months, repeat venography may be indicated to evaluate for a recanalized ovarian vein, a missed cause for reflux, continued filling of pelvic varicosities, or an undiagnosed outflow obstruction. Consideration should be given to the addition of other treatments such as physical therapy, neurostimulation, or trigger point injections. If the presentation was vulvar or lower extremity varicosities, most often there will be minimal change at follow-up. The principle role of ovarian vein embolization is elimination of the highest point of reflux. Ablation or resection of vulvoperineal or leg varicosities that have not resolved can be performed with lesser chance of recurrence. Post Procedural Care - Non Saphenous Varicosities and PCS • Regression of lower extremity varicosities does not necessarily correlate with relief from other symptoms associated with PCS. • Disappearance of lower extremity varicosities does correlate with relief from other symptoms associated with PCS. Creton D, Hennequin L, Kohler F, Allaert FA. Embolisation of symptomatic pelvic veins in women presenting with non-saphenous varicose veins of pelvic origindthree-year follow-up. Eur J Vasc Endovasc Surg 2007;34:112-7. Meneses L, Fava M, Diaz P, Andia M, Tejos C, Irarrazabal P, et al. Embolization of incompetent pelvic veins for the treatment of recurrent varicose veins in lower limbs and pelvic congestion syndrome. Cardiovasc Intervent Radiol 2013;36:128-32. AVF Practice Guidelines 1. PCS should NOT be a diagnosis of exclusion, but suspected by typical symptoms and a past history of vulvar veins in pregnancy 2. Visible perineal varices confirm at least a component of PCS 3. U/S confirms the presence, and in skilled hands can determine the cause, of pelvic varices. 4. Selective venography confirms the cause and anatomical features, to then proceed to endovenous ablative treatment by coils with or without sclerotherapy 5. Both surgical and endovenous ablation of ovarian vein reflux are equally effective 6. Coil treatment has greater patient acceptance, but long-term results, particularly possible recanalization, are unknown. Conclusions • PCS represents a significant source of chronic pelvic pain and productivity loss • A clinical diagnosis - Keep a high index of suspicion – Chronic pain induces psychological changes. We need to be sensitive and supportive – Multidisciplinary approach • OBGYN • Interventional team • Good relief with endovascular techniques – Patient expectations to be Conclusions • Venous outflow obstruction plays an important role in the clinical expression of chronic venous disease. • Compression of the left iliac vein at the arterial crossover point may be present in 1/3rd of the general population without any venous symptoms. • The combination of reflux and obstruction gives the highest levels of venous hypertension and the most severe symptoms compared with either alone. • Chronic obstruction of the iliac vein results in severe symptoms because of poor compensation by collateral formation. Conclusions • Percutaneous endovenous stenting has emerged during the last decade as the method of choice to treat venous outflow obstruction due to chronic venous disease. • Stents have also been placed to relieve obstruction revealed after removal of acute iliofemoral thrombus. • Stenting of the venous outflow obstruction of the lower extremities can be performed with low risk, long-term high patency rate, and a low rate of in-stent restenosis. • Intravascular Ultrasound (IVUS) is critical in determining lesion presence, severity, and balloon/stenting sizing. Please refer back to the complete presentation on Pelvic Congestion Syndrome. Thank You