Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
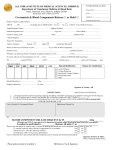
NEW YORK STATE DEPARTMENT OF HEALTH Bureau of Emergency Medical Services Blood and Tissue Resources Program Blood Transfusion Transfer Orders Patient Name (Print) DOB Patient ID Date Transferring Hospital Name Continue PRBC Receiving Hospital Name Other________________________________________ at __________mL/hr Also Administer: # Units PRCBs Other: Special Instructions: Ordering Physician: PRINT NAME SIGNATURE PHONE NUMBER SECTION BELOW TO BE COMPLETED BY AMBULANCE TRANSFUSION SERVICE PERSONNEL Ambulance Service: NYSEMS ID #: Remarks: DOH5210 (4/16) PRINT NAME PRINT NAME PCR #: Rate (mL/hr)