Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
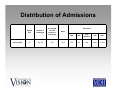
Provider Peer Grouping Monthly Updates May 9, 2011 Katie Burns What is Provider Peer Grouping? • A system for publicly comparing provider performance on cost and quality – …a uniform method of calculating providers' relative cost of care, defined as a measure of health care spending including resource use and unit prices, and relative quality of care… (M.S.§62U.04, Subd. 2) – a combined measure that incorporates both provider risk-adjusted cost of care and quality of care… (M.S.§62U.04, Subd. 3) What Types of Provider Peer Grouping Needs to be Developed? 1. Total Care 2. Care for Specific Conditions The commissioner shall develop a peer grouping system for providers based on a combined measure that incorporates both provider risk-adjusted cost of care and quality of care, and for specific conditions… (M.S.§62U.04, Subd. 3) Hospital Total Care Analysis Attributing Hospital Admissions • The first step in calculating the total care cost measure for each hospital is attribution of inpatient admissions − This serves as the denominator for the cost per admission measure • Generally, attributed admissions consist of all inpatient stays that occur at a hospital over a defined time period Treatment of Readmissions • Hospital stays that occur at the same or another hospital within 30 days after a patient’s discharge are treated differently if the patient is initially admitted due to: – pneumonia – congestive heart failure – heart attack – total knee replacement Treatment of Readmissions • An initial admission related to one of these conditions and procedure is attributed together with the first readmission following it within 30 days of discharge • The combined costs of the initial admission and the first readmission are assigned to the initial hospital Categorizing Admissions • All admissions for each hospital are classified into one of three categories: 1) Initial admission for AMI, CHF, pneumonia, or total knee replacement 2) First readmission within 30 days of discharge from an initial admission 3) Admission for any other condition or procedure that is neither an initial admission for AMI, CHF, pneumonia, or total knee replacement nor a readmission for one of these three conditions or one procedure Hospital Admissions • There were 434,148 admissions in Minnesota during the measurement period Hospital Admissions By Payer Type Distribution of Admissions Sample Size All Hospitals 131 Number of Discharges 434,148 Percentiles Percentage of Total Number of Discharges Mean 100 3,314 10th 25th 50th (Median) 75th 90th 154 310 889 2,893 11,102 Admissions that may Trigger “Readmission” Attribution Principle Diagnosis/Procedure AMI, CHF, pneumonia, or total knee replacement All Admissions AMI CHF Pneumonia Total Knee Replacement Number of Admissions 6,438 10,567 13,380 11,306 41,691 434,148 Percentage of All Admissions 1.5 2.4 3.1 2.6 9.6 100 Summary of Admission Classifications Initial Admissions All Other Admissions AMI CHF Pneumonia Total Attributed Admissions First Readmission Total Admissions 11,213 429,991 4,157 434,148 647 40,555 560 41,115 10,566 389,436 3,597 393,033 Total Knee Replacement All Hospitals Number of Admissions 391,897 5,254 9,259 12,368 CAHs Number of Admissions 35,532 187 1,472 2717 PPS Hospitals Number of Admissions 356,365 5,067 7,787 9,651 Calculating Cost Measures • Two cost measures are calculated – Actual costs (reflect resource use and unit price) – Standardized costs (reflect resource use only) • Cost per admission − Calculated separately for CAH and other hospitals and within payer type Standardized Cost of Admission • Hospital costs are standardized using AllPatient Refined-Diagnosis Related Groups (APR-DRGs) and length of stay • The standardized cost of an admission is the cost per day of stays within a particular DRG at a particular hospital type paid by a particular payer type multiplied by length of stay of that admission Classifying Hospital Stays • Each hospital stay is classified by payer type and hospital type • Each stay is then classified into an APRDRG and one of four severity levels for each APR-DRG – – – – 1: minor 2: moderate 3: major 4: extreme severity of illness or risk of mortality Calculating Actual and Standardized Costs • Standardized cost per day for each stay is calculated as the sum of costs divided by the sum of lengths of stay across all stays within a DRG-severity cell for a hospital type and payer type Progress Update Provider Report Design • Mathematica will interview quality and financial leadership from 12 hospitals in late May – Recruiting for participants to occur shortly • Testing of physician clinic reports will occur in the summer Stakeholder Involvement Stakeholder Involvement: Rapid Response Team • MDH convened this group to provide input on critical issues – – – – – Approach for specific condition analysis Methodology for attributing patients to providers Benchmarking and determination of peer groups Risk adjustment Design and weighting of individual quality measures into composite quality score Stakeholder Involvement: Reliability Workgroup • MDH convened first meeting of this group in December – Explored characteristics of reliable data – Discussed ways of assessing reliability • Next meeting will focus on data and options related to hospital analysis this spring For more information, see www.health.state.mn.us/ healthreform/peer/index.html Next call Monday, June 13, 2011 7:30 am