Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
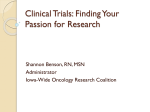
Carcinogenesis vol.24 no.3 pp.605–611, 2003 Regional response leading to tumorigenesis after sulindac in small and large intestine of mice with Apc mutations Kan Yang1,6, Kunhua Fan1, Naoto Kurihara1, Hiroharu Shinozaki1, Basil Rigas2, Leonard Augenlicht3, Levy Kopelovich4, Winfried Edelmann3, Raju Kucherlapati5 and Martin Lipkin1 1Strang 6To whom correspondence should be addressed Email: [email protected] Sulindac and other NSAIDs have been widely studied as potential chemopreventive agents for colon cancer. Shortterm studies have shown adenomatous polyps to regress in patients with familial adenomatous polyposis (FAP). In this study the effect of sulindac on cancer as an endpoint was evaluated in ApcMin mice, a preclinical model of FAP with an Apc mutation in codon 850 that leads to gastrointestinal adenomas and carcinomas. Three groups of mice were studied all of which were fed AIN-76A diet: one group was fed AIN-76A diet alone, a second group received sulindac 200 p.p.m. premixed in the diet and a third group received sulindac 180 p.p.m. added in drinking water. ApcMin mice were killed 9 weeks after feeding was initiated. Mice receiving sulindac developed fewer tumors in the intestine overall; the major decrease in tumor development after sulindac was seen in the small intestine regardless of route of administration. In the large intestine, however, sulindac significantly increased the incidence, multiplicity and volume of tumors in the colon of ApcMin mice, a regional response to sulindac differing from previous reports. Quantitative measurements of apoptosis, Bax and Bcl-xL protein expression in the ApcMin mice revealed the ratio of Bax/Bcl-xL expression and apoptosis increased in the small intestine but decreased in the cecum, consistent with the regional tumorigenesis observed after sulindac. These findings thus suggest involvement of Bax and apoptosis in tumors developing after sulindac treatment in this mouse model. Introduction Several lines of evidence indicate the value of non-steroidal anti-inflammatory drugs (NSAIDs) as potential chemopreventive agents for colorectal cancer. Long-term administration of these compounds roughly halves the incidence of, and mortality from colon cancer in humans (1–3). Sulindac, one of the NSAIDs, is widely used for its anti-inflammatory properties and has been considered a potential chemopreventive agent for treatment of patients with familial adenomatous polyposis Abbreviations: FAP, familial adenomatous polyposis; Apc, adenomatous polyposis coli; ApcMin, ApcMin⫹/–; NSAIDs, non-steriodal anti-inflammatory drugs. © All rights reserved. Oxford University Press 2003 Materials and methods Animals and diets Thirty ApcMin mice (Jackson Laboratories, Harbor, ME), ~4 weeks old, were randomly divided into three groups and fed one of three diets: AIN-76A diet alone, AIN-76A diet with 200 p.p.m. sulindac premixed, and AIN-76A diet with 180 p.p.m. sulindac added to drinking water. The AIN-76A diet provides 3.9 kcal/g and consists of corn oil 5% (12% of calories), calcium 0.52 mg/g (1.3 mg/kcal), phosphorus (as PO4) 0.4 mg/g (1.1 mg/kcal) and vitamin D3 1.0 IU/g (0.26 IU/kcal). ApcMin mice were maintained on their respective AIN-76A or treatment diets for 9 weeks. The duration of treatment was dictated by the lifespan of 4–5 months of the mouse strain (18,19). The average consumption of sulindac was 0.6 mg/day/mouse, an amount equivalent to the dose that inhibits tumor growth reported in ApcMin mice (23). Mice were weighed and feces were tested for gastrointestinal bleeding (hemoccult) at baseline, and weekly thereafter, until animals were killed. Evaluation of tumor development Mice were killed by cervical dislocation, the gastrointestinal tract was removed, opened longitudinally and the contents were washed in cold phosphatebuffered saline (PBS) pH 7.4. The mucosa was flattened on filter paper and fixed in 10% neutral-buffered formalin. Each specimen was examined under a dissecting microscope. Tumors were numbered and their location was recorded. Tumor volume, measured using a grid in the eyepiece of the microscope, was expressed in units of mm3. The flat mucosa of the stomach, duodenum, cecum, proximal and distal colon was processed for further study. Representative tumors from the small intestine and all the tumors in the cecum and colon were sampled and processed. All other internal organs and lymph nodes were examined for tumors. Sections of paraffin-embedded tumor 605 Downloaded from http://carcin.oxfordjournals.org/ at oxford university press on November 23, 2016 Cancer Research Laboratory at The Rockefeller University, 1230 York Avenue, New York, NY 10021, USA, 2American Health Foundation, Valhalla, NY 10595, USA, 3Albert Einstein College of Medicine, Bronx, NY 10461, USA, 4Division of Cancer Prevention, National Cancer Institute, Bethesda, MD 20892, USA and 5Division of Genetics, Brigham and Women Hospital, Boston, MA 02115, USA (FAP) (4–6). In addition to inhibiting aberrant crypt foci in the colon, a precursor of adenoma and cancer (7), sulindac has decreased the number and size of adenomas in humans with FAP (8–15) without having complete regression in all studies (10–12,14,15). In rodents sulindac inhibits colonic carcinogenesis induced by chemical carcinogens (16,17). The establishment of mouse models with targeted Apc gene mutations makes it possible to carry out chemopreventive studies on models of human FAP (18–22). The effects of NSAIDs including sulindac on intestinal tumor development in these mouse models are similar to those of humans, with decreased tumor number and size and without complete disappearance (23–29). Some attention has been given to colorectal cancer developing in patients with FAP after they received sulindac treatment (13,30–33). In view of the emerging role of sulindac and similar pharmaceutical agents as potentially important chemopreventive agents for colon cancer, we carried out a detailed study of the effects of sulindac on tumorigenesis in ApcMin mice, an animal model of human FAP. In this report we provide evidence that, while sulindac did indeed decrease the number and volume of tumors in the small intestine, it simultaneously increased tumor incidence, number and volume in the large intestine. To explore mechanisms that might contribute to this regional response to sulindac, we carried out measurements of apoptosis, and Bax and Bcl-xL in the small intestine, cecum and distal colon. Regional responses of apoptosis, and Bax/Bcl-xL expression after sulindac treatment were demonstrated in the ApcMin mice. K.Yang et al. Table I. Incidence, number and volume of intestinal tumors Group n Overall Small intestine Large intestine A. Incidence AIN-76A Sulindac in AIN-76A Sulindac in drinking water, mice fed AIN-76A 10 10 10 10 (100%) 10 (100%) 10 (100%) 10 (100%) 7 (70%) 10 (100%) 3 (30%) 10 (100%)a 10 (100%)a B. Tumor number per mouse, mean ⫾ SEM AIN-76A Sulindac in AIN-76A Sulindac in drinking water, mice fed AIN-76A 10 10 10 37.1 ⫾ 5.3 5.5 ⫾ 2.4b 14.9 ⫾ 3.9a 36.7 ⫾ 5.3 3.4 ⫾ 2.2b 11.1 ⫾ 3.7a 0.4 ⫾ 0.2 2.1 ⫾ 0.4a 3.8 ⫾ 0.4a C. Tumor volume (mm3), mean ⫾ SEM (median) AIN-76A Sulindac in AIN-76A Sulindac in drinking water, mice fed AIN-76A 10 10 10 43.2 ⫾ 5.1 (42.3) 3.6 ⫾ 0.6 (3.5)b 6.0 ⫾ 1.4 (4.5)b 41.9 ⫾ 5.1 (41.6) 0.6 ⫾ 0.3 (0.02)a 1.7 ⫾ 1.0 (0.6)a 1.3 ⫾ 0.9 (0.0)c 3.0 ⫾ 0.5 (3.0)a,d 4.3 ⫾ 0.7 (3.9)a,d the proteins were made in tumors and corresponding flat mucosa in those regions of the ApcMin mice. Apoptosis Apoptosis originated as a morphological phenomenon, and measurements in the present study were based on morphologic features. Characteristic features required for identification of apoptotic bodies included: a single, condensed small cell with or without cytoplasm (apoptotic body) or a cluster of apoptotic bodies inside another healthy cell (host cell), with or without a halo around the apoptotic body. Measurements were carried out on well-oriented intestinal crypts of flat mucosa. Cells on the mucosal surface of the proximal and distal colon were also included. Twenty-five crypts (50 crypt columns) were scored for each mouse. The apoptotic cells per crypt column were computed. Apoptotic cells in the villi of small intestine were measured separately. The number of apoptotic cells in each villous column was scored. Twenty five villi (50 villous columns) were studied for each mouse. The number of villous columns with apoptotic cells and number of apoptotic cells per villous column were calculated. In tumors, 1000 tumor cells or more were scored for apoptotic bodies. Fig. 1. Tumorigenesis in the gastrointestinal tract of ApcMin mice after sulindac. (A) tumor incidence, (B) tumor multiplicity, (C) tumor volume (*P ⬍ 0.01; **P ⬍ 0.001, sulindac group compared with controls). tissues and 15 serial sections from flat mucosa of each location sampled were examined histologically after staining with hematoxylin and eosin. Diagnoses were based on the WHO classification system (34). To determine the role of apoptosis and related proteins Bax/Bcl-xL in tumor development in both small and large intestine, measurements of apoptosis and 606 Evaluation of Bax and Bcl-xL expression Expression of Bax and Bcl-xL was evaluated on immunohistochemical preparations of tumors taken from small and large intestine and flat mucosa of duodenum, cecum and distal colon of ApcMin mice in sulindac and control groups. The antibodies to Bax (N-20) and Bcl-xL (A-20) were purchased from Santa Cruz Biotechnology (Santa Cruz, CA). Six slides with five serial tissue sections per slide were cut from a paraffin block and labeled. To avoid variation of staining intensity, all tissue-slides were stained at the same time, and all tissue sections were cut by one technologist with the same microtome. Three slides with an odd number (nos 1, 3 and 5) were used for immunohistochemical staining for Bax and Bcl-xL and the first two slides with an even number (nos 2 and 4) were stained for H&E for apoptosis study. On the slides with odd numbers the specific antibody to Bax and Bcl-XL was applied to every other section in each slide. This parallel staining for two different antibodies facilitated the data being more comparable. The last slide (no. 6) was used for negative control on which neither antibody to Bax nor to BclXL was added to tissue sections as immunohistochemical staining. Measurements were carried out with a computer-assisted cell image analyzer (Samba 4000). This system uses a color CCD camera to separate red (R), green (G) and blue (B) colors and convert these colors to digital form. The size of the resulting pixels was 0.25 µm under a magnification of 40⫻. By using a software program, immuno 4.04 per Area Program for cytoplasmic labeling measurement, it was possible to assay the size of positive areas (Labeling Index) and staining intensity (Mean Optical Density) of a given area in an immunohistochemical preparation. Through segregation the assay was confined only to epithelial cells, i.e. in a crypt column of flat mucosa, and to neoplastic glands of a tumor. Ten crypts (20 crypt columns), well oriented, were measured from each intestinal segment of flat mucosa for each mouse. For tumors, 1000 cells from different areas were randomly selected for measurement. Bax and Bcl-XL protein expression was assayed separately in two differently staining tissue sections nearby on one slide for each mouse or tumor. The data were automatically generated with an arbitrary unit (a.u.) including percentage of positive area, staining intensity and overall expression of a combination of Downloaded from http://carcin.oxfordjournals.org/ at oxford university press on November 23, 2016 n, number of mice studied. Comparisons are made to corresponding control (AIN-76A diet, no treatment) using two-tailed Fisher exact probabilities test for tumor incidence; Mann– Whitney and exact binomial calculation for tumor number and volume: aP ⬍ 0.01; bP ⬍ 0.001. Comparisons between tumor volume in the large intestine and small intestine: cP ⬍ 0.001; dP ⬍ 0.01. Sulindac induces colonic tumors Table II. Distribution of tumors found in the large intestine Group Mean number of tumors per mouse Overall AIN-76A Sulindac in AIN-76A Sulindac in drinking water, mice fed AIN-76A 0.4 ⫾ 0.2 2.1 ⫾ 0.4a 3.8 ⫾ 0.4a Right side Left side Subtotal Cecum PC DC 0.3 ⫾ 0.2 1.8 ⫾ 0.3a,b 3.6 ⫾ 0.5a,b 0.2 ⫾ 0.1 1.3 ⫾ 0.2a 3.3 ⫾ 0.4a 0.1 ⫾ 0.1 0.5 ⫾ 0.3 0.3 ⫾ 0.3 0.1 ⫾ 0.1 0.3 ⫾ 0.2 0.2 ⫾ 0.1 aBy Mann-Whitney test or Exact Binomial Calculation: compared with AIN-76A bCompared with the left side of colon of the same diet group: P ⬍ 0.01. for each mouse strain: P ⬍ 0.01. positive area and staining intensity (percentage of positive area⫻staining intensity). The overall expression was used for the comparisons. The ratio of overall expression of Bax and Bcl-xL are reported for each group, i.e. ratio of Bax and Bcl-XL expression ⫽ mean overall expression of Bax/mean overall expression of Bcl-XL. Comparisons of protein expression between treatment and control groups were based on the ratio. intestine tumor volume decreased 99 and 96% in two sulindac groups, respectively, over the controls with P ⬍ 0.01 for both (0.6 and 1.7 versus 41.9 mm3). However, in the large intestine, tumor volume increased 1.3- and 2.3-fold in the sulindactreated groups, P ⬍ 0.01 for both compared with controls (3.0 and 4.3 versus 1.3 mm3). In both sulindac-treated groups, tumor volume was greater in the large intestine than in the small intestine with P ⬍ 0.01 for both, but it was opposite in the control group (Table I and Figure 1C). Distribution and histology of the large intestinal tumors. The large intestinal tumors that were unexpectedly found in the sulindac-treated groups were studied in detail, with respect to their location and their histological features. Location of tumors in the large intestine. The vast majority of large intestinal tumors were located in the right side of the large intestine, especially in the cecum (Table II and Figure 2A). The mean number of large intestinal tumors in the control group was low (0.4). The preponderance of tumors in the right colon increased in the sulindac-treated groups. The number of tumors in the right side increased 5- and 11-fold in both sulindac-treated groups, P ⬍ 0.01 for both compared with controls (1.8 and 3.6 versus 0.3). The tumor number in the right side was significantly higher than in the left side in both sulindac groups, P ⬍ 0.01, but not in the controls (Table II). Thus, the markedly increased tumor incidence in the large intestine was due to tumors developing in the right colon, especially in the cecum. Histological types of tumors in the large intestine. All 60 tumors found in the large intestine from all three groups were evaluated histologically (Table III). Control ApcMin mice had four tumors found in the colon with one invasive carcinoma and three benign tubular adenomas. After sulindac treatment, invasive carcinomas increased ~8- to 10-fold in both groups. Invasion of the submucosa was found in all 20 adenocarcinomas in sulindac-treated groups (Figure 2B). The potentially malignant villous adenoma increased in the proximal colon in one sulindac group, and flat adenomas were greatly increased and mostly seen in the cecum of mice treated with sulindac. These findings demonstrated a complex effect of sulindac on tumorigenesis in this preclinical mouse model: tumors inhibited in the small intestine and tumors increased in the large intestine. Similar effects of sulindac on tumorigenesis were also observed in Apc1638N mice (26), another mouse model of human FAP; the sulindac administration and diets fed were the same as for ApcMin mice, and the feeding duration was 6 months longer than for ApcMin mice because the lifespan is 12–15 months in Apc1638N and 4–5 months in ApcMin mice (26). Mean ⫾ SEM. PC, proximal (upper half) colon; DC distal (lower half) colon. Results All tumors found in the ApcMin mice were in the intestinal tract. There were no tumors in the stomach and none were detected in the lungs, liver, kidneys or lymph nodes of these mice. Tumorigenesis Tumor incidence. We determined the tumor incidence in the small and large intestine as well as the overall tumor incidence, i.e. tumor incidence in a group of mice regardless of anatomical location of the tumor in the intestinal tract (Table I and Figure 1A). In the small intestine the tumor incidence in the group given sulindac premixed in the solid diet decreased 30% compared with the control group (P ⬎ 0.05). However, in the large intestine, the tumor incidence was 2.3-fold increased in both sulindac-treated groups (100 versus 30% with P ⬍ 0.01) compared with controls. The overall tumor incidence was 100% in each of the three groups having tumors (Table I and Figure 1A). Number of intestinal tumors per mouse (multiplicity). The overall number of tumors per mouse decreased 85 and 60% in both sulindac-treated groups compared with controls with P values ⬍0.001 and ⬍0.01, respectively (5.5 and 14.9 versus 37.1) (Table I and Figure 1B). In the small intestine the number of tumors per mouse decreased 90 and 70% in both sulindac groups compared with controls with P values 0.001 and 0.01, respectively (3.4 and 11.1 versus 36.7, representing mean tumor number in mice fed sulindac in solid food and in drinking water versus tumors in control group (same for below if not specified). In the large intestine, however, changes in the tumor number were in the opposite direction from those seen in the small intestine. The tumor number increased 4.3- and 8.5-fold in the two sulindac-treated groups with both P ⬍ 0.01 compared with controls (2.1 and 3.8 versus 0.4). Tumor volume. The overall tumor volume decreased after sulindac treatment in ApcMin mice. The mean overall volume decreased 92 and 86% in the two sulindac groups compared with controls with both P ⬍ 0.001 (3.6 and 6.0 versus 43.2 mm3). Similar to the overall tumor volume, in the small 607 Downloaded from http://carcin.oxfordjournals.org/ at oxford university press on November 23, 2016 Statistical tests Comparisons between the study and control groups were carried out using Fisher exact probabilities, Mann–Whitney test, and binomial calculations. Significant difference was considered as P ⬍ 0.05. K.Yang et al. 608 Discussion This study demonstrated that the chemopreventive agent sulindac, when administered to ApcMin mice, caused decreased number and size of tumors in the small intestine, consistent with reports in the literature (23–25,27,28). The reduction of tumors in the small intestine provided an important internal control to findings observed in the large intestine. An overall Downloaded from http://carcin.oxfordjournals.org/ at oxford university press on November 23, 2016 Fig. 2. Intestinal tumors in sulindac-treated ApcMin mouse. (A) Two gross tumors elevated above the cecal mucosa (arrows), with ulceration in the center (1.75⫻ original magnification). (B) Histological features of an adenocarcinoma of cecum from the same mouse as (A), with irregular neoplastic glands infiltrating in the submucosa of intestinal wall (arrows) with ulceration on the surface. Hematoxylin and eosin, 200⫻ original magnification. (C) Immunohistochemical preparation showing strong Bax expression in an adenoma in the small intestine of a mouse after sulindac treatment, 100⫻ original magnification. Apoptosis Flat mucosa. To evaluate apoptosis during tumor development, apoptotic bodies were counted with criteria noted in the Materials and methods. Findings are presented in Table IV. Apoptosis was counted in the three groups of mice in intestinal crypt epithelial cells of flat mucosa of duodenum, cecum and distal colon. The number of apoptotic cells per crypt column decreased 44% in the cecum (0.34 versus 0.61, P ⬍ 0.001) and 33% in the distal colon (0.14 versus 0.21, P ⬍ 0.01), but did not significantly change in duodenal crypts (0.08 versus 0.10, P ⬎ 0.05) of mice after sulindac treatment. However, in villi of duodenum the number of villous columns with apoptotic cells increased 30% (19.0 versus 14.6, P ⬍ 0.05) and the number of apoptotic cells per villous column increased 40% (0.21 versus 0.15, P ⬍ 0.01) in mice after sulindac. The data thus indicated that in response to sulindac treatment apoptosis differed in flat mucosa of the small and large intestine in ApcMin mice. Tumors. Apoptosis was measured in tumors located in small and large intestine of sulindac-treated and control groups of mice. After sulindac treatment the percentage of apoptotic cells increased 1.4-fold in small intestinal tumors (0.0156 versus 0.0065, P ⬍ 0.001), and decreased 34% in the cecal tumors (0.0100 versus 0.0151, P ⬎ 0.078). The reduction of apoptosis in cecal tumors did not reach statistical significance, which might be due to only two tumors in the control group. Thus, in the cecum of ApcMin mice apoptosis decreased in flat mucosal cells with a trend to decrease in tumor cells, and increased in small intestinal villous epithelial cells and tumor cells during tumorigenesis. Expression of Bax and Bcl-xL Flat mucosa. Quantitative measurements by computer-assisted cell image analysis showed Bax expression increased and BclXL decreased in epithelial cells in the duodenum with the opposite result in the cecum after sulindac treatment. The overall expression of proteins related to apoptosis in epithelial cells, presented as a ratio of Bax to Bcl-xL increased in the small intestine and decreased in the cecum after sulindac. The ratio increased 1.2-fold in the duodenum (1.38 versus 0.62, P ⬍ 0.05) and decreased 55% in the cecum (0.47 versus 1.04, P ⬍ 0.001) after sulindac treatment (Figure 3A). However, no significant difference was seen in the distal colon (0.72 versus 0.59, P ⬎ 0.05) (Figure 3A). Tumors. Similar to the findings of Bax and Bcl-XL expression in flat mucosa of duodenum, Bax expression increased and Bcl-XL decreased in tumors of the small intestine, and the opposite result was observed in the cecal tumors. Figure 2C is representative of the small intestinal tumors showing Bax with strong expression in neoplastic adenoma cells after sulindac treatment. The ratio of Bax to Bcl-xL in tumors increased 3-fold in the small intestine (1.11 versus 0.28, P ⬍ 0.01) and decreased 79% in the cecum (0.87 versus 4.18, P ⬍ 0.05) after sulindac treatment in ApcMin mice (Figure 3B). Sulindac induces colonic tumors Table III. Histologic types of large intestinal tumors Group Number of tumors found in the large intestine AIN-76A Sulindac in AIN-76A Sulindac in drinking water mice fed AIN-76A Total Adenocarcinoma Villous adenoma Flat tubular adenoma Tubular adenoma Micro-adenoma 4 21 35 1 9 11 0 4 0 0 4 22 3 3 1 0 1 1 Table IV. Apoptosis of intestinal epithelial cells in flat mucosa and tumors of ApcMin mice after receiving control AIN-76A diet and AIN-76A with sulindac Control AIN-76A AIN-76A with sulindac 0.08 ⫾ 0.01 0.34 ⫾ 0.01a 0.14 ⫾ 0.01b Percent of villous columns with apoptotic cells Duodenum 14.6 ⫾ 1.1 19.0 ⫾ 1.4c Number of apoptotic cells/villous column Duodenum 0.15 ⫾ 0.01 0.21 ⫾ 0.02b Tumors Percent of apoptotic cells in 1000 tumor cells Small intestine 0.65 ⫾ 0.08 Cecum 1.51 ⫾ 0.79 1.56 ⫾ 0.22a 1.00 ⫾ 0.08d By Mann–Whitney test: compared with corresponding organ with AIN-76A: aP ⬍ 0.001; bP ⬍ 0.01; cP ⬍ 0.05. Compared with tumors of small intestine after sulindac; dP ⫽ 0.078. Mean ⫾ SEM. The number of tumors studied was 17 in control group including 15 in the small intestine and two in the cecum; 27 in the sulindac group including 12 in the small intestine and 15 in the cecum. protective effect of sulindac against tumor development in the intestine as a whole was observed. When sulindac was premixed in AIN-76A diet or supplied in drinking water it decreased the overall tumor number (85 and 60%), and decreased tumor volume (92 and 86%) in the intestine of the ApcMin mice, findings consistent with previous literature. However, unexpectedly sulindac induced tumor formation in the colon, regardless of the route of administration: premixed in a solid control AIN-76A diet, or added to the drinking water. Findings thus showed a complex effect of sulindac in the intestinal tract of mice with this Apc mutation, a chemopreventive effect in the small intestine, but a tumorenhancing effect in the right side of the large intestine. The increase of tumors in the large intestine of ApcMin mice after sulindac was profound, indicated by increased tumor incidence, multiplicity, volume and higher grade of malignancy in the colon, differing from sulindac effects in small intestine. In humans, carcinomas are known to develop in FAP patients maintained on sulindac treatment (13,30–33), appearing endoscopically as flat, ulcerated lesions. By coincidence these findings in ApcMin mice after sulindac are similar; the occurrence of flat adenomas in these mice is of particular interest as they have been found to occur with increased malignant potential in humans with a hereditary predisposition to colon cancer (35–38). To evaluate the comparative tumor response after sulindac treatment in colon and small intestine, the tumor development ratio of treatment group/control group was analyzed. The Fig. 3. Overall expression of proteins Bax and Bcl-xL presented as ratio of Bax/Bcl-xL in duodenum, cecum and distal colon. (A) In flat mucosa. (B) In tumors of small intestine and cecum. (*P ⬍ 0.05, **P ⬍ 0.01, ***P ⬍ 0.001, sulindac group compared with controls.) relative benefit/harm (RB/H) was calculated as: parameter studied in small intestine⫻large intestine in the treatment group/parameter studied in small intestine⫻large intestine in the control group. Treatment was of benefit with RB/H ⬍1, and was harmful with RB/H ⬎1. A 95% confidence interval (95% CI) was also calculated using log transformed means to further evaluate the significance of RB/H. A beneficial effect was suggested in tumor multiplicity after treatment (RB/H ⫽ 0.49) but without statistical significance (95% CI ⫽ 0.091– 2.583). However, a beneficial effect was observed with a reduction of tumor volume after treatment in the group receiving sulindac in AIN-76A (RB/H ⫽ 0.03, 95% CI ⫽ 0.006–0.185). Mice receiving sulindac supplied in drinking water also had a beneficial effect with the tumor volume decreasing, but not tumor number (data not shown). Findings thus indicated a beneficial relative tumor response in colon 609 Downloaded from http://carcin.oxfordjournals.org/ at oxford university press on November 23, 2016 Flat mucosa Number of apoptotic cells/crypt column Duodenum 0.10 ⫾ 0.02 Cecum 0.61 ⫾ 0.04 Distal colon 0.21 ⫾ 0.02 K.Yang et al. Acknowledgements The work was supported by NIH Awards CN65031, R01-CA87559, U01-CA84301 and the Ann E.Woodward Foundation. References 1. Giovannucci,E., Egan,K.M., Hunter,D.J., Stampfer,M.J., Colditz,G.A., Willett,W.C. and Speizer,F.E. (1995) Aspirin and the risk of colorectal cancer in women. N. Engl. J. Med., 333, 609–614. 2. Smalley,W. and DuBois,R.N. (1997) Colorectal cancer and non-steroidal anti-inflammatory drugs. Adv. Pharmacol., 39, 1–20. 3. Williams,C.S., Smalley,W. and DuBois,R.N. (1997) Aspirin use and potential mechanisms for colorectal cancer prevention. J. Clin. Invest., 100, 1325–1329. 4. Waddell,W.R. and Loughry,R.W. (1983) Sulindac for polyposis of the colon. J. Surg. Oncol., 24, 83–87. 610 5. Giardiello,F.M., Offerhaus,G.J. and DuBois,R.N. (1995) The role of nonsteroidal anti-inflammatory drugs in colorectal cancer prevention. Eur. J. Cancer, 31A, 1071–1076. 6. Shiff,S.J. and Rigas,B. (1997) Nonsteroidal anti-inflammatory drugs and colorectal cancer: evolving concepts of their chemopreventive actions. Gastroenterology, 113, 1992–1998. 7. Takayama,T., Latsuki,S., Takahashi,Y., Ohi,M., Nojiri,S., Sakamaki,S., Kato,J., Kogawa,K., Miyake,H. and Niitsu,Y. (1998) Aberrant crypt foci of the colon as precursors of adenoma and cancer. N. Engl. J. Med., 339, 1277–1284. 8. Labayle,D., Fischer,D., Vielh,P., Drouhin,F., Pariente,A., Bories,C., Duhamel,O., Trousset,M. and Attali,P. (1991) Sulindac causes regression of rectal polyps in familial adenomatous polyposis. Gastroenterology, 101, 635–639. 9. Nugent,K.P., Farmer,K.C., Spigelman,A.D., Williams,C.B. and Phillips,R.K. (1993) Randomized controlled trial of the effect of sulindac on duodenal and rectal polyposis and cell proliferation in patients with familial adenomatous polyposis. Br. J. Surg., 80, 1618–1619. 10. Giardiello,F.M., Hamilton,S.R., Krush,A.J., Piantadosi,S., Hylind,L.M., Celano,P., Booler,S.V., Robinson,C.R. and Offerhaus,G.J. (1993) Treatment of colonic and rectal adenomas with sulindac in familial adenomatous polyposis. N. Engl. J. Med., 328, 1313–1316. 11. Giardiello,F.M., Offerhaus,J.A., Tersmette,A.C., Hylind,L.M., Krush,A.J., Brensinger,J.D., Booker,S.V. and Hamilton,S.R. (1996) Sulindac induced regression of colorectal adenomas in familial adenomatous polyposis: evaluation of predictive factors. Gut, 38, 578–581. 12. Winde,G., Schmid,K.W., Schlegel,W., Fischer,R., Osswald,H. and Bunte,H. (1995) Complete reversion and prevention of rectal adenomas in colectomized patients with familial adenomatous polyposis by rectal lowdose sulindac maintenance treatment. Dis. Colon Rectum, 38, 813–830. 13. Cruz-Correa,M., Hylind,L.M., Romans,K.E., Booker,S.V. and Giardiello,F.M. (2002) Long-term treatment with sulindac in familial adenomatous polyposis: a prospective cohort study. Gastroenterology, 122, 641–645. 14. Keller,J.J., Offerhaus,G.J., Polak,M., Goodman,S.N., Zahurak,M.L., Hylind,L.M., Hamilton,S.R. and Giardiello,F.M. (1999) Rectal epithelial apoptosis in familial adenomatous polyposis patients treated with sulindac. Gut, 45, 795–796. 15. Giardiello,F.M., Yang,V.W. and Hylind,L.M. (2002) Primary chemoprevention of familial adenomatous polyposis with sulindac. N. Engl. J. Med., 346, 1054–1059. 16. Rao,C.V., Rivenson,A., Simi,B., Zang,E., Kelloff,G., Steele,V. and Reddy,B.S. (1995) Chemoprevention of colon carcinogenesis by sulindac, a non-steroidal anti-inflammatory agent. Cancer Res., 55, 1464–1472. 17. Reddy,B.S., Kawamori,T., Lubet,R.A., Steele,V.E., Kelloff,G.J. and Rao,C.V. (1999) Chemopreventive efficacy of sulindac sulfone against colon cancer depends on time of administration during carcinogenic process. Cancer Res., 59, 3387–3391. 18. Moser,A.R., Pitot,H.C. and Dove,W.F. (1990) A dominant mutation that predisposes to multiple intestinal neoplasia in the mouse. Science, 247, 322–324. 19. Su,L.K., Kinzler,K.W., Volgelstein,B., Preisinger,A.C., Moser,A.R., Luongo,C., Gould,K.A. and Dove,W.F. (1992) Multiple intestinal neoplasia caused by a mutation in the murine homolog of the APC gene. Science, 256, 668–670. 20. Fodde,R., Edelmann,W., Yang,K. et al. (1994) A targeted chain-termination mutation in the mouse Apc gene results in multiple intestinal tumors. Proc. Natl Acad. Sci. USA, 91, 8969–8973. 21. Yang,K., Edelmann,W., Fan,K., Lau,K., Kolli,B., Fodde,R., Khan,P.M., Kucherlapati,R. and Lipkin,M. (1997) A mouse model of human familial adenomatous polyposis. J. Exp. Zool., 277, 245–254. 22. Oshima,M., Oshima,H., Kitagawa,K., Kobayashi,M., Itakura,C. and Taketo,M. (1995) Loss of Apc heterozygosity and abnormal tissue building in nascent intestinal polyps in mice carrying a truncated Apc gene. Proc. Natl Acad. Sci. USA, 92, 4483–4486. 23. Boolbol,S.K., Dannenberg,A.J., Chadburn,A. et al. (1996) Cyclooxygenase2 overexpression and tumor formation are blocked by sulindac in a murine model of familial adenomatous polyposis. Cancer Res., 56, 2556–2560. 24. Beazer-Barclay,Y., Levy,D.B., Moser,R., Dove,W.F., Hamilton,S.R., Vogelstein,B. and Kinzler,K.W. (1996) Sulindac suppresses tumorigenesis in the Min mouse. Carcinogenesis, 17, 1757–1760. 25. Chiu,C.H., McEntee,M.F. and Whelan,J. (1997) Sulindac causes rapid regression of preexisting tumors in Min/⫹ mice independent of prostaglandin biosynthesis. Cancer Res., 57, 4267–4273. 26. Yang,K., Fan,K., Shinozaki,H., Newmark,H., Edelmann,W., Kucherlapati,R. and Lipkin,L. (1999) Sulindac increases carcinoma Downloaded from http://carcin.oxfordjournals.org/ at oxford university press on November 23, 2016 and small intestine after sulindac treatment with decreased tumor volume. The mechanisms involved in sulindac effects are complex. Pathways of arachidonic acid metabolism, prostaglandin and COX-2 are believed to be involved. Overexpression of COX-2 and PGE2 has been reported in intestinal tumors of humans and ApcMin mice (39–43). Studies show that sulindac sulfide inhibits COX activity, but not the sulfone metabolite (44), and both sulindac sulfide and sulfone are reported to induce apoptosis in different cell types (44–46). Many COX-2independent mechanisms have been investigated which mediate inhibition of tumors with NSAIDs (47–52). Apoptosis induced by NSAIDs is a major mechanism in the inhibition of tumors (53–56). Evidence has indicated that multiple pathways are involved in the control of apoptosis, including death receptors on cellular membranes with apaf1caspases via cytochrome c released from mitochondria (57– 60). BCL-2 family members, Bax, a pro-apoptosis protein, and Bcl-xL, an anti-apoptosis protein, are believed to mediate increased or decreased release of cytochrome c from mitochondria (59). Apoptosis is completely abolished in response to sulindac and other NSAIDs in colonic carcinoma cells with a BAX deficiency, indicating that BAX plays a crucial role in this process (55). Our studies show sulindac significantly increased apoptosis in the small intestine and decreased apoptosis in the cecum in both the flat mucosa and tumors of mice with this Apc mutation. This regional response of apoptosis to sulindac was consistent with the regional tumor response observed, providing evidence of a role for apoptosis in tumorigenesis in this preclinical FAP model; Bax/Bcl-xL expression further revealed a corresponding regional difference after sulindac. Current information on sulindac metabolism in humans and animals (reviewed in refs 56–59) does not indicate a reason for site-specific effects of sulindac in the intestinal tract. These findings are the first report of a procarcinogenic effect of sulindac in the large intestine in a preclinical model of human FAP. Mice with an Mlh1 mutation also show increased tumor development in both the small and large intestine after sulindac treatment (61). Therefore, it would appear advisable to carry out further studies of sulindac and other NASIDs in preclinical models related to colon cancer, to further define regional responses and possible interactions with mutations that might occur. So far there is no systematic follow-up information available regarding patients receiving long-term treatment of sulindac or other NSAIDs, although several individuals have been reported to develop colorectal carcinomas after sulindac treatment. Sulindac induces colonic tumors 46. Chan,T.A., Morin,P.J., Vogelstein,B. and Kinzler,K.W. (1998) Mechanisms underlying nonsteroidal anti-inflammatory drug-mediated apoptosis. Proc. Natl Acad. Sci. USA, 95, 681–686. 47. Schmelz,E.M., Bushnev,A.S., Dillehay,D.L., Sullards,M.C., Liotta,D.C. and Merrill,A.H. Jr (1999) Ceramide-β-D-glucuronide. Synthesis, digestion and suppression of early markers of colon carcinogenesis. Cancer Res., 59, 5768–5772. 48. Patrignani,P., Santini,G., Sciulli,M.G., Marinacci,R., Fusco,O., Spoletini,L., Natolli,C., Procopio,A. and Maclouf,J. (1999) Cyclooxygenaseindependent induction of p21 WAF-1/CIP-1, apoptosis and differentiation by L-745,337 and salicylate in HT-29 colon cancer cells. Adv. Exp. Med. Biol., 469, 555–561. 49. Yang,W.C., Mathew,J., Velcich,A., Edelmann,W., Kucherlapati,R., Lipkin,M., Yang,K. and Augenlicht,L.H. (2001) Targeted inactivation of the p21WAF1/cip1 gene enhances Apc-initiated tumor formation and the tumor-promoting activity of a Western-style diet high-risk diet by altering cell maturation in the intestinal mucosa. Cancer Res., 61, 565–569. 50. McEntee,M.F., Chiu,C.-H. and Whelan,J. (1999) Relationship of betacatenin and Bcl-2 expression to sulindac-induced regression of intestinal tumors in Min mice. Carcinogenesis, 20, 635–640. 51. Lehmann,J.M., Lenhard,J.M., Oliver,B.B., Ringold,G.M. and Kliewer,S.A. (1997) Peroxisome proliferators—activated receptors alpha and gamma are activated by indomethacin and other non-steroidal anti-inflammatory drugs. J. Biol. Chem., 272, 3406–3410. 52. Huang,Y., He,Q., Hillman,M.J., Rong,R. and Sheikh,M.S. (2001) Sulindac sulfide-induced apoptosis involves death receptor 5 and the caspase 8dependent pathway in human colon and prostate cancer cells. Cancer Res., 61, 6918–6924. 53. Elder,D.J., Hague,A., Hicks,D.J. and Paraskeva,C. (1996) Differential growth inhibition by the aspirin metabolite salicylate in human colorectal tumor cell lines: enhanced apoptosis in carcinoma and in vitro-transformed adenoma relative to adenoma cell lines. Cancer Res., 56, 273–276. 54. Piazza,G.A., Rahm,A.K., Finn,T.S., Fryer,B.H., Stoumen,A.L., Pamukcu,R. and Ahnen,D.J. (1997) Apoptosis primarily accounts for the growthinhibitory properties of sulindac metabolites and involves a mechanism that is independent of cyclooxygenase inhibition, cell cycle arrest and p53 induction. Cancer Res., 57, 2452–2459. 55. Zhang,L., Yu,J., Park,B.H., Kinzler,K.W. and Vogelstein,B. (2000) Role of Bax in the Apoptotic response to anticancer agents. Science, 293, 989–992. 56. Shureiqi,I., Chen,D., Lotan,R., Yang,P., Newman,R.A., Fischer,S.M. and Lippman,S.M. (2000) 15-Lipoxygenase-1 mediates nonsteroidal antiinflammatory drug-induced apoptosis independently of cyclooxygenase-2 in colon cancer cells. Cancer Res., 60, 6846–6850. 57. Schulze-osthoff,K., Ferrari,D., Los,M., Wesselborg,S. and Peter,M.E. (1998) Apoptosis signaling by death receptors. Eur. J. Biochem., 254, 439–459. 58. Askkenazi,A. and Dixit,V.M. (1999) Apoptosis control by death and decoy receptors. Curr. Opin. Cell Biol., 11, 255–260. 59. Gross,A., McDonnell,J.M. and Korsmeyer,S.J. (2000) BCL-2 family members and the mitochondria in apoptosis. Genes Dev., 13, 1899–1911. 60. Williams,C.S., Mann,M. and DuBois,R.N. (1999) The role of cyclooxygenases in inflammation, cancer and development. Oncogene, 18, 7908–7915. 61. Yang,K., Fan,K., Lia,M., Edelmann,W., Augenlicht,L.H., Lubet,L., Kopelovich,L., Kucherlapati,R. and Lipkin,M. (2001) Sulindac increases tumor development in the colon of mice with Mlh1⫹/– mutation. Proc. Am. Assoc. Cancer Res., 42, 264. Received June 3, 2002; revised November 26, 2002; accepted December 14, 2002 611 Downloaded from http://carcin.oxfordjournals.org/ at oxford university press on November 23, 2016 development in the colons of mice with Apc mutations. Proc. Am. Cancer Res., 40, 529. 27. Mahmoud,N.N., Bilinski,R.T., Churchill,M.R., Edelmann,W., Kucherlapati,R. and Bertagnolli,M.M. (1999) Genotype-phenotype correlation in murine Apc mutation: differences in enterocyte migration and response to sulindac. Cancer Res., 59, 353–359. 28. Chiu,C.H., McEntee,M.,F. and Whelan,J. (2000) Discordant effect of aspirin and indomethacin on intestinal tumor burden in Apc (Min/⫹) mice. Prostaglandins Leukot. Essent. Fatty Acids, 62, 269–275. 29. Oshima,M., Murai,N., Kargman,S., Arguello,M., Luc,P., Kwong,E., Taketo,M.M. and Evans,J.F. (2001) Chemoprevention of intestinal polyposis in the Apcdelta716 mouse by rofecoxib, a specific cyclooxygenase-2 inhibitor. Cancer Res., 61, 1733–1740. 30. Niv,Y. and Fraser,G.M. (1994) Adenocarcinoma in the rectal segment in familial polyposis coli is not prevented by sulindac therapy. Gastroenterology, 107, 854–857. 31. Lynch,H.T., Thorson,A.G. and Smyrk,T. (1995) Rectal cancer after prolonged sulindac chemoprevention. Cancer, 75, 936–938. 32. Matsuhashi,N., Nakajima,A., Shinohara,K., Oka,T. and Yazaki,Y. (1998) Rectal cancer after sulindac therapy for a sporadic adenomatous colonic polyp. Am. J. Gastroenterol., 93, 2261–2266. 33. Tonelli,F., Valanzano,R., Messerini,L. and Ficari,F. (2000) Long-term treatment with sulindac in familial adenomatous polyposis: is there an actual efficacy in prevention of rectal cancer? J. Surg. Oncol., 74, 15–20. 34. Jass,J.R. and Sobin,L. H. (1989) Histological Typing of Intestinal Tumours, 2nd Edn. World Health Organization, Springer-Verlag, Berlin. 35. Muto,T., Kamiya,J., Sawada,T. et al. (1985) Small ‘flat adenoma’ of the large bowel with special reference to its clinicopathologic features. Dis. Colon Rectum, 28, 847–851. 36. Teixeira,C.R., Tanaka,S., Haruma,K., Yoshihara,M., Sumii,K. and Shimamoto,F. (1996) Flat-elevated colorectal neoplasms exhibit a high malignant potential. Oncology, 53, 89–93. 37. Lynch,H.T., Smyrk,T.C., Lanspa,S.J., Jenkins,J.S., Lynch,P.M., Cavalieri,J. and Lynch,J.F. (1993) Upper gastrointestinal manifestations in families with hereditary flat adenoma syndrome. Cancer, 71, 2709–2714. 38. Cairns,A. and Quirke,P. (1999) Flat adenomas. Br. J. Surg., 86, 1489–1490. 39. Pugh,S. and Thomas,G.A.O. (1994) Patients with adenomatous polyps and carcinomas have increased colonic mucosal prostaglandin E2. Gut, 35, 675–678. 40. Kargman,S.L., O’Neill,G.P., Vickers,P.J., Evans,J.F., Mancini,J.A. and Jothy,S. (1995) Expression of prostaglandin F/H synthase-1 and -2 protein in human colon cancer. Cancer Res., 55, 2556–2559. 41. Williams,C.S., Luongo,C., Radhika,A., Zhang,T., Lamps,L.W., Nanney,L.B., Beauchamp,R.D. and DuBois,R.N. (1996) Elevated cyclooxygenase-2 levels in Min mouse adenomas. Gastroenterology, 111, 1134–1140. 42. Oshima,M., Dinchuk,J.E., Kargman,S.L., Oshima,H., Hancock,B., Kwong,E., Trzaskos,J.M., Evans,J.F. and Taketo,M.M. (1996) Suppression of intestinal polypsis in APCn716 knockout mice by inhibition of cyclooxygenase 2 (COX-2). Cell, 87, 803–809. 43. Hull,M.A., Booth,J.K., Tisbury,A., Scott,N., Bonefer,C., Markham,A.F. and Colettta,P.L. (1999) Cyclooxygenase 2 is up-regulated and localized to macrophages in the intestine of Min mice. Br. J. Cancer, 79, 1399–1405. 44. Lim,J.T., Piazza,G.A., Han,E.K. et al. (1999) Sulindac derivatives inhibit growth and induce apoptosis in human prostate cancer cell lines. Biochem. Pharmacol., 58, 1097–1107. 45. Shiff,A.J., Qiao,L., Tsai,L.-L. and Rigas,B. (1995) Sulindac sulfide, an aspirin-like compound, inhibits proliferation, causes cell cycle quiescence and induces apoptosis in HT-29 colon adenocarcinoma cells. J. Clin. Invest., 96, 491–503.