Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
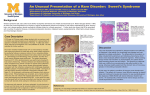
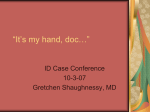
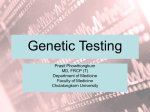
Sweet’s Syndrome Allison Dupont AM Report 1/17/06 Definition Sweet’s syndrome (acute febrile neutrophilic dermatosis) is characterized by: Fever Peripheral neutrophilia Painful red skin papules, nodules and/or plaques Neutrophilic infiltration of skin (particularly the dermis) Clinical Presentation Fever (>38˚C) can be intermittent and may precede skin manifestations by days to weeks. Systemic symptoms may include headache, myalgia, arthralgia, and general malaise. Cutaneous lesions consist of erythematous to violaceous tender papules which may coalesce to form plaques. The plaques are not pruritic. Most often found on the face, neck and upper extremities (especially the dorsum of the hands), but can occur anywhere. Lesions on the lower extremities may resemble erythema nodosum. Clinical Presentation Oral ulcers (more common in patients with Sweet’s syndrome and a hematologic malignancy. Ocular involvement (uncommon in malignancy-associated and drug-induced Sweet’s syndrome). Conjunctivitis, episcleritis Clinical Presentation Involvement of internal organs may occur leading to: Alveolitis Sterile osteomyelitis Involvement of liver, pancreas, and/or kidneys Neurologic and psychiatric changes Laboratory Findings Lab findings are nonspecific. Majority will have peripheral neutrophilia. Other possible lab abnormalities include: Elevated sedimentation rate Elevated C-reactive protein Leukocytosis Consider evaluation of hepatic and renal function. Pathology Sweet’s syndrome characteristically involves dense neutrophilic infiltration of the dermis +/- dermal edema. Neutrophil karyorrhexis is commonly seen. There is no involvement of the vasculature of the skin and no necrosis (in contast to pyoderma gangrenosum). Diagnosis Major Criteria Abrupt onset of painful erythematous plaques or nodules. Histopathologic evidence of a dense dermal neutrophilic infiltrate without vasculitis. Minor Criteria Fever (>38˚C) Association with an underlying hematological/visceral malignancy, inflammatory disease, or pregnancy or preceded by an upper respiratory or GI infection or vaccination. Excellent response to treatment with systemic corticosteroids. Peripheral neutrophilia (>70% neutrophils) Associated Conditions Sweet’s syndrome is associated with an underlying disease or condition in up to 50% of patients. Sweet’s syndrome may be the presenting sign and the underlying disease may not become apparent for several years after Sweet’s syndrome occurs. There is a female predominance except in the case of malignancy-associated Sweet’s syndrome. Associated Conditions 1. Malignancy 2. Approximately 21% of patients with Sweet’s syndrome have a malignancy. 15% hematological (most commonly AML) 6% solid tumors (most commonly carcinomas of the GU tract, GI tract, or breast) Infections Mostly of the upper respiratory or GI tract Streptococcus, mycobacterium, Yersinia, Salmonella, Shigella Associated Conditions 3. Inflammatory bowel disease 4. 5. Sweet’s syndrome may occur alone or in combination with pyoderma gangrenosum. Pregnancy Other conditions with a possible association: -Sarcoidosis -Rheumatoid arthritis -Thyroid disease (Grave’s disease and Hashimoto’s thyroiditis) Drug-induced Sweet’s syndrome Criteria slightly different than classical syndrome. Temporal relationship between drug ingestion/injection and clinical presentation. Resolution of lesions/symptoms after withdrawal of drug or treatment with corticosteroids. Drug-induced Sweet’s syndrome G-CSF is responsible for the majority of cases. Other possible causes: furosemide, lithium, hydralazine, trimethoprimsulfamethoxazole, and oral contraceptives. Pathogenesis Etiology of Sweet’s syndrome is unknown. Presumed to be due to a hypersensitivity reaction to an eliciting antigen which leads to stimulation of cytokine release. Cytokines precipitate neutrophil activation and infiltration. Response to treatment with corticosteroids supports this etiology. Pathogenesis The source of the eliciting antigen may be diverse, including bacterial, viral or tumoral antigens. Treatment Gold standard: Systemic corticosteroids Start at 1 mg/kg/day prednisone with long taper (4-6 weeks) to 10 mg/day. Many patients require several months of 10-30 mg/day to suppress recurrences. Localized Sweet’s syndrome can sometimes be treated with high-potency topical corticosteroids. Treatment Other first-line agents include: 1. Oral potassium iodide -Systemic symptoms resolve in 1-2 days. -Dermatitis resolves in 3-5 days. 2. Colchicine -Systemic symptoms resolve in 2-3 days. -Dermatitis resolves in 2-5 days. Alternative therapies Indomethacin Clofazimine Cyclosporine Dapsone References Burall, Barbara M.D. “Sweet’s syndrome (acute febrile neutrophilic dermatosis)”. Dermatology Online Journal 5(1):8. Cohen, Philip R. MD, Kurzrock, Razelle MD. “Sweet’s syndrome revisited: a review of disease concepts”. International Journal of Dermatology. Volume 42, Issue 10. October 2003. Cohen, Philip R. “Sweet’s syndrome”. Orphanet. October 2003. Federman et al. “Cutaneous manifestations of malignancy”. Postgraduate Medicine Online. January 2005. Joe, Edwin K. MD. “Sweet’s syndrome”. Dermatology Online Journal 9(4):28. Moschella, Samuel L. MD. “Neutrophilic dermatoses”. UpToDate. “Sweet’s Syndrome”. Dermis.net.