Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
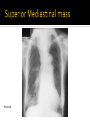
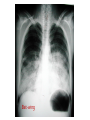
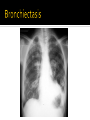
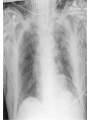
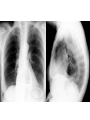
Brandy McKelvy, MD, FCCP Assistant Professor Division of Pulmonary, Critical Care and Sleep Medicine Air Fat least opaque most lucent Black Soft tissue Bone to to to Metal most opaque least lucent White Anatomic Air Fat Water Bone Metal Example Air Mineral oil Water Tums tablets Lead-bottom glass PA & Lateral AP Apical lordotic Lateral decubitus Free flowing pleural effusions Up-right (erect) semi-erect & supine Supine increases medistinal size due to gravity Distribution of pleural fluid KUB vs abdominal series (3 views) Know what you are ordering! Inspiratory/expiratory films Number of ribs visible? ▪ Ideally 8-10 posterior ribs Posterior-Anterior (PA) Standard view & most reliable technique Erect films detect air under the diaphragm Lateral view Done at the same time as the PA film Helps localize infiltrates, identify caridomegaly, effusions & lymphadenopathy Posterior mediastinum and cost-phrenic recesses visible Anterior-posterior (AP) Portable- patient is too ill to go to radiology, usually patient is sitting upright in bed Poorer quality AP films may cause the mediastinum & heart to appear larger ( up to 15% increase in mediastinal structures) Enlargement of the radiographic image of an object relative to its actual size Increased film-subject distance Super-imposition of structures in different planes Resultant image = summation of opacities Two structures of the same radiopacity in contact – their margins cannot be identified Pick one order of operations that you prefer You will not be a professional radiographer but you should always look at your own films Start with: Reading the label on the chest film (what type of film) Reading the label of the film (correct patient) Assessing the quality of the film Identifying the radiographic technique ▪ AP/PA film, exposure, rotation, position (supine, sitting or erect) Poor inspiration “Penetration” High diaphragms, crowded lung markings Disappearing thoracic vertebral details through the heart Rotation Note equal distances from the vertebral spines to the medial ends of the clavicles Under penetrated: you will not be able to see the thoracic vertebrae Over penetration: Lungs are “too black” Unable to see lung markings Check for rotation Does the thoracic spine align in the center of the sternum and between the clavicles? Are the clavicles level? Equal distant from sternum? Was film taken under full inspiration? A good film will show: 10 posterior ribs 6 anterior ribs to qualify When x-ray beams pass through the anterior chest on to the film under the patient, the ribs closer to the film (posterior) are most apparent Gastric bubble should be on the left Aortic knob typically should be on the left Soft tissues- thickness, contours, presence of gas, masses Bones- density, lesions, fractures Lungs- look for abnormal densities, (opacity or luncency) or pneumothorax Pleura- thickening, calcification, effusion, or pneumothorax Trachea- midline, or deviated, wall, lumen diameter Mediastinum- width and contour, discreet masses Heart- size and shape Pulmonary vessels- artery or vein enlargement Hila- position, masses, lymphadenopathy Identify and check positioning of lines, tubes, and other invasive devices Foreign bodies- anything that should not normally be in the chest Boundaries of the film Costophrenic angle Diaphragm Heart Aortic arch Trachea Hilum Main carina Stomach bubble J. Ascending aorta A. B. C. D. E. F. G. H. Costophrenic angle Diaphragm Heart Aortic arch Trachea Hilum Main carina Stomach bubble J. Ascending aorta A. B. C. D. E. F. G. H. 1. Right Atrium 2. R Ventricle 3. Apex of L Ventricle 4. Superior Vena Cava 5. Inferior Vena Cava 6. Tricuspid Valve 7. Pulmonary Valve 8. Pulmonary Trunk 9. Right PA 10. Left PA Cardio/thoracic ratio should be < 50% The hila – the large blood vessels going to and from the lung at the root of each lung where it meets the heart Check for elevation, location, symmetry, lymph nodes, enlarged vessels, masses Increased Pulmonary arterial HTN ▪ Pruning Pulmonary venous HTN ▪ Pulmonary edema ▪ No pruning Decreased Pulmonary embolism Hypovolemia Right side 1. SVC 2. Ascending aorta 3. Right Atrium (RA) Left side 4. LSCA 5. Aortic knob 6. Left PA 7. Left atrium 8. Left ventricle 5. Aortic arch 2. Ascending aorta 9.Right Ventricle 6.Pulmonary trunk 7. Left atrium 8. Left Ventricle Superior Anterior Middle Posterior Anterior mediastinal masses Middle mediastinum Thymoma Thyroid Teratomas “Terrible lymph-nodes”(lymphoma) Lymph nodes Esophagus Aorta Duplication cysts, bronchogenic cysts Hiatal hernia Posterior mediastinum Neurogenic tumors Spinal mass Chest wall masses lymphoma thymoma thryroid Right upper lobe Right middle lobe Left upper lobe Lingula Right lower lobe Left lower lobe Loss of lung volume Anatomy shifts towards atelectasis Linear, smooth, wedge-shaped Apex of opacity starts at hilum Air bronchograms or lack of air Sharp edges Volume loss Normal lung volume No anatomical shift Consolidation/infiltrates Irregular margins Coalesce of infiltrates Air bronchograms Blood, pus, water, protein, tumor all look the same on chest-x-ray Focal vs Diffuse Infiltrates will occupy 1 of 3 spaces: Alveoli ▪ ▪ ▪ ▪ ▪ “Fluffy”, irregular Confluence Air-bronchograms Silhouette sign Acinar nodules Supporting structures ▪ The interstitium or the lymphatics ▪ ▪ ▪ ▪ Reticular i.e. “lacy” infiltrates Nodules Lymphatics spread of tumor Interstitial fibrosis The blood vessels Alveolar-filling, or “airspace” disease: “Pointillist” patterns Air bronchograms RML consolidation Right Upper Lobe Infiltrate Multi-lobar opacities “Always” diffuse Linear Reticular Nodular/miliary Honey -combing Curly B lines – fluid in the intra-lobular septae A. Generalized interstitial thickening = linear (“reticular”) B. Discrete interstitial thickening = nodules C. Interstitial & alveolar filling = silhouette Curly B lines Curly B lines Cardiogenic vs non-cardiogenic pulmonary edema? Bat-wing ARDS Nodules Solitary or multiple Solitary pulmonary nodule Size ▪ 1-2 mm, micronodular (miliary) ▪ 2 mm- 3.0 cm Calcified or non-calcified Margins? Cavitation? Doubling time? How long has it been present? Masses > 3 cm Renal Cell Carcinoma Testicular cancer TB/HIV No walls Emphysema Bullea >1 cm Thin walled Pneumatocels Aircysts (LAM, EG, PLCH) Thick walled Honey combing With Air-fluid levels ▪ Lung abscess, septic emboli, TB, tumors Bronchiectasis Aspergillus cavity Pleural effusions Free flowing Loculated Pleural calcifications Pleural line Pneumothorax? Right hemi-diaphragm always slightly higher than the left Bilateral elevated hemi-diaphragms: Increased intra-abdominal pressure, increased airway pressures Bilateral phrenic nerve palsy Unilateral elevated hemi-diaphragm Unilateral phrenic nerve palsy Volume loss ▪ Atelectasis ▪ Lobectomy Intra-abdominal mass Sub-pulmonic effusion Herniation thru the diaphragm Look under the diaphragm Chest tube port outside chest wall