Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
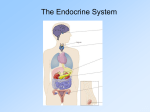
Unit 15: Assisting in Endocrinology Study Guide Answer Keys Vocabulary Review 1. C. Glucagon 8. TSH 2. A. Glycosuria 9. Polyphagia 3. B. Glycogen 10. ADH 4. polydipsia 11. Polyuria 5. ACTH 12. Gluconeogenesis 6. Insulin 13. Growth hormone 7. Ketosis 14. Prolactin Skills and Concepts 1. a. Melatonin: Produced by the pineal gland; helps regulate sleep cycles b. TSH: Produced by the anterior pituitary gland; stimulates the thyroid gland to produce thyroid hormones c. Adrenaline: Produced by the adrenal medulla; activates the response to stress d. Insulin: Produced by the beta cells of the pancreas; helps cells use CHO for energy e. Glucagon: Produced by alpha cells of the pancreas; regulates blood glucose levels 2. An exocrine gland secretes substances through a duct system outward (e.g., sweat glands). An endocrine gland produces chemicals known as hormones and secretes them directly into the bloodstream, where they can be carried to target tissue. 3. Negative feedback is the most common feedback system. An endocrine gland is activated by an imbalance and acts to correct the imbalance by stopping the secretion process. For example, if calcium blood levels fall below normal, the parathyroid glands are stimulated to release parathyroid hormone (PTH). PTH acts to increase blood calcium levels either by stimulating the absorption of calcium from the gut or by demineralizing bone to release stored calcium. This change in the blood calcium level is detected by the parathyroid gland, which then stops production of PTH. 4. a. Thyroid-stimulating hormone (TSH) – stimulates the thyroid gland to produce hormones b. Adrenocorticotropic hormone (ACTH) - stimulates the production and secretion of glucocorticoids c. Prolactin - stimulates the development of the mammary gland d. Growth hormone (GH) - stimulates the growth of the long bones e. Follicle-stimulating hormone (FSH) - stimulates oogenesis and spermatogenesis f. Luteinizing hormone (LH) - promotes ovulation 5. a. Gigantism – Oversecretion of GH in childhood before the epiphyseal plates in the long bones have closed will cause the long bones to grow excessively. Those affected may reach 8 feet or taller. Because GH has a secondary effect on the blood glucose level, these persons may develop DM. b. Acromegaly - If hypersecretion of GH occurs in adulthood, the disorder is called acromegaly. The epiphyseal plates are closed so the long bones cannot grow; a wide range of manifestations can occur because of the growth of excessive connective tissue and overproduction of bone. c. Dwarfism - Hypopituitary dwarfism occurs when the pituitary gland fails to produce normal amounts of GH. The child’s height is impaired, but he or she will have a normal size head and trunk. 1 Unit 15: Assisting in Endocrinology Study Guide Answer Keys 6. a. Diabetes insipidus: Diabetes insipidus develops when ADH is not produced or released in sufficient amounts. ADH increases the permeability of the renal and collecting tubules in the kidneys, permitting fluid to be reabsorbed and causing the urine to become more concentrated. Without the action of ADH, fluid is not reabsorbed from the renal tubules, which causes a large amount of fluid to be excreted in the urine, with the potential onset of dehydration in the patient. b. Addison’s disease: Addison’s disease is a condition of adrenal insufficiency. Symptoms include hypoglycemia, increased pigmentation of the skin, muscle weakness, gastrointestinal disturbances, and fatigue. Cortisol and aldosterone deficiencies lead to retention of potassium and the excretion of water and sodium in the urine. Severe dehydration, low blood volume, low blood pressure, and circulatory shock can occur. Treatment includes replacement of cortisol with the long-term daily administration of glucocorticoids. c. Cushing’s syndrome: Cushing’s syndrome is hypersecretion of the adrenal cortex, causing increased levels of cortisol. Usually a benign pituitary tumor causes the release of excessive amounts of ACTH. Symptoms associated with Cushing’s syndrome may be seen in individuals being treated with corticosteroids for medical reasons. 7. Hypothyroidism: Lower metabolic rate, heat loss, poor mental and physical development, fatigue, weight gain, hair loss, slower pulse rate, lowered body temperature, muscle cramps, menorrhagia, and thick, dry, puffy skin. Hyperthyroidism: Weight loss, tachycardia, palpitations, hypertension, agitation, nervousness, depression, tremor, excessive sweating, goiter, and exophthalmia. 8. Prediabetes is a condition in which an individual has a higher than normal blood glucose level but not high enough for a diagnosis of type 2 diabetes. Two different tests are used to diagnose prediabetes: the fasting plasma glucose test (FPG) and the oral glucose tolerance test (OGTT). A person with prediabetes has a fasting blood glucose level between 100 and 125 mg/dL; individuals with an FPG of 126 mg/dL or higher are diagnosed as diabetic. A patient with prediabetes would have a 2-hour OGTT of 140 to 199 mg/dL; diabetes is diagnosed if the OGTT is 200 mg/dL or higher. 9. DM type 1 usually develops before age 30 and is characterized by a complete absence of insulin production. Patients need daily insulin injections. DM type 2 develops gradually because of an insufficient amount of insulin or resistance at the target cell site or both. 10. Insulin shock occurs if an adult patient’s blood glucose level drops below 46 to 60 mg/dL. In the case of a diabetic coma, the patient is unable to use glucose for energy because insulin either is absent or insufficient, or there is resistance to insulin at the target cell site; as a result, glucose levels build up in the blood, causing loss of consciousness. 11. a. Polyuria (excessive urine production) b. Polydipsia (excessive thirst) c. Polyphagia (increased appetite) 12. Refer to Table 45-1 in the text. 13. Refer to Table 45-2 in the text. 2