Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
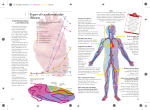
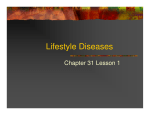
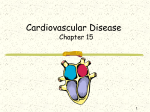
Cost-Effectiveness Analysis of Hypertension Guidelines in South Africa Absolute Risk Versus Blood Pressure Level Thomas A. Gaziano, MD, MSc; Krisela Steyn, MSc, NED, MD; David J. Cohen, MD, MSc; Milton C. Weinstein, PhD; Lionel H. Opie, MD, DPhil, FRCP Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Background—Hypertension is responsible for more deaths worldwide than any other cardiovascular risk factor. Guidelines based on blood pressure level for initiation of treatment of hypertension may be too costly compared with an approach based on absolute cardiovascular disease (CVD) risk, especially in developing countries. Methods and Results—Using a Markov CVD model, we compared 6 strategies for initiation of drug treatment—2 different blood pressure levels (160/95 and 140/90 mm Hg) and 4 different levels of absolute CVD risk over 10 years (40%, 30%, 20%, and 15%)—with one of no treatment. We modeled a hypothetical cohort of all adults without CVD in South Africa, a multiethnic developing country, over 10 years. The incremental cost-effectiveness ratios for treating those with 10-year absolute risk for CVD ⬎40%, 30%, 20%, and 15% were $700, $1600, $4900, and $11 000 per quality-adjusted life-year gained, respectively. Strategies based on a target blood pressure level were both more expensive and less effective than treatment decisions based on the strategy that used absolute CVD risk of ⬎15%. Sensitivity analysis of cost of treatments, prevalence estimates of risk factors, and benefits expected from treatment did not change the ranking of the strategies. Conclusions—In South Africa, current guidelines based on blood pressure levels are both more expensive and less effective than guidelines based on absolute risk of cardiovascular disease. The use of quantitative risk-based guidelines for treatment of hypertension could free up major resources for other pressing needs, especially in developing countries. (Circulation. 2005;112:3569-3576.) Key Words: cost-benefit analysis 䡲 hypertension 䡲 prevention 䡲 stroke 䡲 cardiovascular diseases D The other method is the blood pressure level approach, which uses different cutpoints in blood pressure level to define hypertension and recommend treatment. This approach is exemplified by the American Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VII).5 Among those without CVD, these blood pressure level– based guidelines are primarily focused on arbitrary blood pressure levels above which hypertension is diagnosed, with only a minor modification if diabetes mellitus is present. Although the blood pressure guidelines recommend the ascertainment of other risk factors, the decision to initiate drug treatment does not take into account this additional information, with the exception of diabetes mellitus and chronic renal disease. The blood pressure level–approach based on a single cutoff point does not differentiate risk based on age, actual level of espite advances in treatment, cardiovascular disease (CVD) is expected to be the leading cause of death and disability worldwide by 2020.1 Among risk factors for CVD, hypertension is responsible for more deaths worldwide than any other, including cholesterol, tobacco, body mass index, and physical activity.2 Hence, the social and economic demands of adequately treating hypertension are of considerable magnitude and complexity. Internationally, there are 2 approaches to the primary prevention of CVD expressed through hypertension guidelines. One approach is based on absolute risk and has been adopted by the British Hypertension Society3 and New Zealand.4 In this strategy, the absolute CVD risk is estimated on the basis of the number and severity of all major risk factors. Treatment decisions are then based on the choice of a level of risk above which it is reasonable to attempt to lower blood pressure with medications. Received January 12, 2005; revision received May 19, 2005; accepted July 18, 2005. From Cardiovascular Medicine (T.A.G.) and the Division of Social Medicine and Health Inequalities (T.A.G., M.C.W.), Brigham & Women’s Hospital, Harvard Medical School, Boston, Mass; Chronic Diseases of Lifestyle Unit of the Medical Research Council (K.S.), Cape Town, South Africa; Cardiology Division (D.J.C.), Beth Israel Deaconess Medical Center, Boston, Mass; Hatter Institute (L.H.O.), Department of Medicine and Cape Heart Centre, Faculty of Health Sciences, University of Cape Town, South Africa; and Department of Health Policy and Management (M.C.W.), Harvard School of Public Health, Boston, Mass. Guest Editor for this article was Clyde W. Yancy, MD. Reprint requests to Thomas A. Gaziano, MD, Cardiovascular Medicine, Brigham & Women’s Hospital, 75 Francis St, Boston, MA 02115. E-mail [email protected] © 2005 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/CIRCULATIONAHA.105.535922 3569 3570 Circulation December 6, 2005 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 cholesterol, smoking, or the number of other risk factors present. Consequently, this method does not allow for precise assessment of a patient’s true CVD risk. For example, the predicted 10-year CVD risk for a patient with a systolic blood pressure of 130/90 mm Hg and more than 1 risk factor can range from 5% to 50%. Likewise, a patient with systolic blood pressure of 170 mm Hg and no other risk factors can have a 10-year risk of ⬍5% years depending on age. Thus, at one extreme, some high-risk patients are undertreated, and at the other extreme, many patients at relatively low risk are treated with very little absolute benefit. An analysis in Great Britain6 revealed that the methods of JNC VI and the World Health Organization/International Society Hypertension (WHO/ISH) for screening those with more than a 20% 10-year-risk of CVD, compared with the Framingham risk equation, had sensitivities of 80% to 90% but specificities of 10% (JNC VI) and 50% (WHO/ISH) and thus failed to differentiate those between high and low risk. The health and economic implications of this poor specificity were evaluated in the WHO CHOICE (World Health Organization Choosing Interventions that are Cost-Effective)7 program. It showed that the strategy of treating those at high absolute risk in various regions of the world was cheaper and saved more lives than one based on target levels of individual risk factors. However, the model is limited by its use of regional rather than national epidemiology and cost estimates. These limitations are particularly important because the distribution of hypertension differs by geography and ethnicity,8 as much as does the extent of economic development in different countries. Recently, the South African Hypertension Society adopted and revised its new guidelines9,10 based on the JNC VI11 and VII5 guidelines. Furthermore, South Africa has conducted one of the first demographic health surveys in sub-Saharan Africa to estimate the prevalence of hypertension and other CVD risk factors.12 We therefore believed that this developing country with a multiethnic population provided a unique and timely opportunity to conduct a cost-effectiveness analysis comparing the 2 approaches in a country with a growing burden of CVD and in which epidemiological and cost data were available to help inform the potential consequences of the various guideline choices for hypertension. Methods Guidelines Compared We conducted a cost-effectiveness analysis of blood pressure level– and absolute risk– based hypertension guidelines in persons without known CVD or target-organ disease. The strategies compared included 2 different strategies based on blood pressure levels and 4 different strategies based on the absolute level of cardiovascular risk, as well as a comparison strategy of no antihypertension prescription therapy, for a total of 7 different strategies. The first blood pressure level strategy was the 1995 South African Hypertension Society guidelines.13 These guidelines recommended initiation of drug treatment for all those who have a blood pressure greater than 160/ 95 mm Hg or those with a blood pressure greater than 140/90 mm Hg and diabetes mellitus. The second blood pressure level strategy was equivalent to the current guidelines that were adopted by the South African Hypertension Society in 2001.9 According to the current South African guidelines, drug treatment is initiated for those who have a blood pressure greater than 140/90 mm Hg alone or 130/ 85 mm Hg with diabetes mellitus after lifestyle changes failed to reduce the above levels. Under the 4 strategies based on absolute risk for CVD strategies, if an individual has an absolute risk of CVD over the next 10 years of more than 15% (or 20%, 30%, or 40%, depending on the specific strategy), then antihypertensive therapy is initiated. Finally, we considered a “no-intervention” strategy in which patients would not receive any pharmacological primary prevention treatment for hypertension. We assumed for all strategies that once an individual developed CVD, he or she would be treated according to the standard of care currently in practice. Treatment guidelines in all 7 strategies were applied to a simulated population of all South African adults from the age of 35 to 75 years who were free of CVD, defined as angina, myocardial infarction, sudden death, or stroke. South Africa CVD Risk Stratification The population was stratified into 288 cohorts representing each of the possible combinations of the 6 characteristics: sex, age, systolic blood pressure, smoking, diabetes mellitus, and cholesterol. Age was stratified into 4 deciles (35 to 44, 45 to 54, 55 to 64, and 65 to 74 years) according to the 1996 census.14 There was further stratification by systolic blood pressure into 3 groups: ⬍140 mm Hg, 140 to 59 mm Hg, and ⱖ160 mm Hg. Further dichotomization was done for smoking and diabetes mellitus.15–17 Finally, the strata were divided according to 3 levels of total cholesterol: ⬍5.18 mmol/L (200 mg/dL), 5.18 to 7.25 mmol/L (200 to 280 mg/dL), and ⱖ7.25 mmol/L (280 mg/dL).18,19 The proportion in each stratum of the cohort reflected the results of the 1998 South African Demographic and Health Survey12 for age, sex, smoking status, and blood pressure. The distributions of cholesterol and diabetes mellitus were stratified with mean values according to sex, because few data exist to determine their relationship to the other risk factors. Markov CVD Model No cohort data exist in South Africa that show the effects of the risk factors for CVD, nor are there any randomized control trial data on the benefit of treatment for hypertension. There have been no trials that compared the different hypertension guidelines. Even if these trial data did exist, they likely would not be for the length of time we chose to evaluate, and we therefore chose to model CVD. We used Markov modeling, which allowed us to predict disease events over a given length of time for a particular cohort and adjust risks as the population aged. The simulation began with a population free of CVD. Baseline assumptions for the CVD model (simplified representation in Figure 1) and their sources are listed in Table 1. If under the specific set of guidelines, the conditions for initiation of hypertensive drug treatment were met, the cohort entered into the treatment arm; otherwise, the simulated cohort entered the no-treatment arm. For absolute risk groups, a 10-year risk of CVD was calculated that was based on the Framingham risk function.20 Each year, the cohort faced a probability of dying of a noncardiac cause on the basis of South African life tables,21 developing coronary heart disease, having a stroke, or surviving free of CVD. The risks for an event— either coronary heart disease or stroke—were based on separate Framingham risk functions for each event.20,22 Separate short-term and annual survival probabilities were defined for each cohort group based on age and sex for each coronary heart disease outcome and for stroke. Finally, the probabilities of being admitted to a hospital and having angiography, revascularization, or CABG were estimated for each scenario in South Africa. Data on actual rates do not exist, but we assumed rates equal to one tenth the US rates in 1999 and varied these rates in sensitivity analyses. At the end of each year, the cohort was then redistributed to 1 of 8 health states, depending on the events of the previous year. The 8 states were disease-free (no CVD event or death of other causes), postarrest, post–myocardial infarction without CABG, post–myocardial infarction with CABG, postangina without CABG, postangina with CABG, postcerebrovascular accident (CVA), and dead (non– CVD-related and CVD-related death). For those in the disease-free state, the risk factors remained the same with the exception of age, Gaziano et al CEA of Hypertension Guidelines in South Africa 3571 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Figure 1. Schematic of CVD model. The full model represented by this simplified version has 62 possible clinical pathways. All members of the cohort begin free of CVD disease. In the initial year, each member of the cohort has a certain probability based on treatment status risk factors of moving along 1 of 4 pathways: remaining disease free, dying of non-CVD causes, or developing fatal or nonfatal coronary heart disease or stroke. In the subsequent years, those with prior CVD follow a separate pathway with adjusted risks for recurrence of CVD or death based on age and prior event. All risks are updated annually based on age. Costs are captured along the way for treatment of hypertension and CVD events. CHD indicates coronary heart disease; CVA, cerebrovascular accident; Rx, treatment; and MI, myocardial infarction. which was updated annually. For those with prior CVD, their risk was based on their CVD history. Total life-years and quality-adjusted life-years (QALYs) were accumulated for the cohort over the 10 years for each guideline. QALYs were obtained with the weighted disease state values from the disability weights of the WHO Global Burden of Disease project.23 All analyses were performed with DATA by TreeAge Software Incorporated. Treatment Assumptions Treatment was assumed to lead to a 10-mm Hg reduction in systolic blood pressure on the basis of the meta-analyses by MacMahon et al24 and Collins et al.25 It was assumed that all individuals would receive the same reduction in blood pressure from the medications given the work in the meta-analysis by MacMahon et al.24 On the basis of these meta-analyses, we estimated that a 10-mm Hg reduction in systolic blood pressure would result in a 40% relative risk reduction for stroke and a 14% relative risk reduction for coronary heart disease events.24,25 Costs Only the costs related to treatment of hypertension, CVD events, and their sequelae were included in the model. Screening costs included the cost of obtaining risk factor information. Because both of the blood pressure level– based guidelines required ascertainment of these values, the cost of screening was the same across all strategies except the no-intervention strategy. Productivity costs due to work loss and costs of care giving and travel time were not included in the analysis. The proportions of patients who received each antihypertensive drug and the average number of medications prescribed per person were obtained from the South African Demographic Health Survey.12 The costs of treatment for hypertension included the number of clinic visits required for each of the guidelines. Medication costs reflected wholesale prices and administration costs.26 The cost per visit was according to the South African “scale of benefits.”27 These are the levels that are reimbursed by third-party payers and are considerably less than the charges recommended by the South African Medical Association.27 Treatment costs for the morbid sequelae of hypertension—angina, myocardial infarction, cardiac arrest, and stroke—are not directly itemized for each diagnosis in South Africa; however, the mean cost per CVD admission has been estimated in South Africa.28 Relative weights for the costs of individual diagnoses were estimated from US data.29 These relative differences were applied to the average South African CVD admission cost to determine an estimate for each specific CVD admission. Costs of coronary angiography, percutaneous coronary interventions, and CABG surgery were according to the South African Medical Association scale of benefits and included both hospital and physician costs. Economic Analysis and Discounting All costs are reported in 2001 US dollars. To convert costs from the South African rand to the US dollar, costs were first converted using the mean exchange rate for the year in which each of the South African costs were reported. Then, the costs were adjusted to 2001 US dollars using the inflation rate for South Africa over those years up to 2001. Both future costs and benefits were discounted at 3% per year, consistent with current guidelines. Effects were measured in years of life and QALYs gained. Strategies that had higher costs and fewer QALYs than at least 1 other strategy, ie, that were dominated, were eliminated from further consideration. Incremental costeffectiveness ratios were calculated for each of the nondominated programs. Sensitivity Analyses Univariate sensitivity analyses were conducted on the costs of hypertension treatment, the costs per hospital diagnosis, the proportion of the population that undergoes CABG or angiography, the proportion of the population being treated for hypertension, the prevalence of hypercholesterolemia, the relative risk reduction from treatment, and the discount rate. We also performed a probabilistic multivariate sensitivity analysis with Monte Carlo simulation30 in which we simultaneously varied all of the values listed above. For this analysis, the costs and discount rate followed a uniform distribution over the ranges listed in Table 1, whereas the remaining variables followed a log-normal distribution. New values from within each of the probability distributions were randomly selected during each of 1000 iterations, and the quality-adjusted life expectancy and lifetime cost for each of the strategies were calculated. Model Validation We compared projected annual mortality rates from the model for ischemic heart disease (death due to angina, myocardial infarction, or cardiac arrest) and stroke with the mortality rates recorded in South Africa. We also compared the total direct costs of CVD predicted by our model with a previously published estimate. Results Model Validation Table 2 compares the projections of costs, morbidity, and mortality from our model with the estimates from the avail- 3572 Circulation December 6, 2005 TABLE 1. Estimated Base-Case Values and Assumptions for Model Input Parameters Parameter Value Range for Sensitivity Analyses Epidemiology and treatment Hypertension and smoking prevalence10 Age, sex, and race differences Risk functions 10-Year cardiovascular disease risk7 Framingham risk function 7 10-Year coronary heart disease risk Framingham risk function 10-Year stroke risk20 Framingham risk function Noncardiovascular mortality19 Table Proportion of eligible people receiving antihypertensive treatment10 44% 32%–56% Treatment effects BP reduction24 10 mm Hg systolic 24,25 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 CHD risk reduction 14% 14%–25% Stroke reduction24,25 40% 10%–50% $86 $ 43–$192 Costs 10,21–25 Hypertension treatment CVD events Average cost of CVD admission $5636 $3150–$12 600 CHD ⬍30-day survival $3166 $1500–$6000 CHD ⬎30-day survival $4402 $2000–$8000 Stroke $8633 $4000–$17 000 CABG $11 431 $5500–$22 000 Catheter-based revascularization $4737 $2400–$9500 Post-CHD with CABG, 1st year $1300 $ 650–$2600 Post-CHD with CABG, subsequent years $600 $ 300–$1200 Post-CHD without CABG, 1st year $1500 $ 750–$3000 Post-CHD without CABG, subsequent years $840 $ 420–$1700 3% 0%–7% Annual treatment costs 24 Discount rate BP indicates blood pressure; CHD, coronary heart disease. able literature on South Africa. In general, the model was able to accurately project the number of deaths due to ischemic heart disease and stroke, the incidence of stroke, and the overall direct cost of CVD. Our model predicted that 12% of annual deaths for adults aged 35 to 74 years would be due to ischemic heart disease and 14% would be due to stroke. Published data on annual death rates due to ischemic heart disease range from 5% to 13%, and annual death rates from stroke range from 8% to 16% after adjustment for the more than 20% of deaths that were unregistered or ill defined.31–33 Our model projected that the annual incidence of stroke was 323 per 100 000 persons. There are no published incidence rates for stroke for the population as a whole, but Rosman34 found that the range was from 100 per 100 000 for those 20 years and older to 500 per 100 000 for those aged 55 years and older. Our model results are well within these figures. With regard to costs, our model also projected direct annual CVD costs of US $690 million in 1991 costs. Pestana28 found that direct CVD costs were estimated between US $620 and $810 million in 1991. TABLE 2. Cost-Effectiveness Model Predicted and Actual Outcomes Outcome Model Prediction Published Reports, Range Annual death rate due to IHD, % 12 5–13 Annual death rate due to stroke, % 14 8–16 Stroke rate, per 100 000 323 100–500 Annual direct cost of CVD, $US millions 690 620–810 IHD indicates ischemic heart disease. Table 3 displays the costs, life-years, QALYs, and incremental cost-effectiveness ratios for the 6 strategies of hypertension treatment compared with no pharmacological treatment as a baseline. The 4 “absolute risk” strategies had incremental cost-effectiveness ratios ranging from $700 per QALY gained to $11 000 per QALY gained, depending on the risk threshold for initiating treatment. The strategy of initiating antihypertensive therapy for those individuals with a predicted 10-year CVD risk ⬎40% had an incremental costeffectiveness ratio of $700 per QALY gained compared with Gaziano et al CEA of Hypertension Guidelines in South Africa 3573 TABLE 3. Costs, Effects, and Incremental Cost-Effectiveness Ratios of Guidelines for Hypertension Management Over 10 Years in 10 Million Adults Cost, $US Millions Incremental Cost,† $US Millions Effect, QALYs (Millions) 䡠䡠䡠 8 78.185 78.173 Incremental Effect,† QALYs Incremental C/E Ratio† $/QALY $/LYS* 䡠䡠䡠 12 000 䡠䡠䡠 700 䡠䡠䡠 900 No treatment 5820 Absolute risk CVD ⬎40% 5828 Absolute risk CVD ⬎30% 5874 46 78.214 29 000 1600 2100 Absolute risk CVD ⬎20% 6110 236 78.262 48 000 4900 6700 Absolute risk CVD ⬎15% 6351 241 78.284 22 000 11 000 18 000 1995 South African guidelines (target level 160/95 mm Hg) 6418 67 78.260 ⫺24 000 Dominated‡ Dominated Current guidelines (target level 140/90 mm Hg) 6735 317§ 78.279 ⫺5000 Dominated Dominated Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 LYS indicates life-years saved. *Total and incremental life-years not shown. †Each strategy’s cost and effect are compared with the preceding less costly one. ‡A dominated strategy is one that is both more expensive and less effective than the preceding strategy to which it is compared. §Compared with absolute risk CVD ⬎15%, because the 1995 guidelines are dominated by the absolute risk CVD ⬎15% strategy. no treatment. The absolute risk of CVD ⬎30%, absolute risk of CVD ⬎20%, and absolute risk of CVD ⬎15% strategies had cost-effectiveness ratios of $1600, $4900, and $11 000 per QALY, respectively, each being compared with the next less inclusive treatment criterion. On the other hand, the 1995 South African guidelines and the 2001 South African Guidelines strategies were both more costly and resulted in fewer gains in quality-adjusted life expectancy than the absolute risk of CVD ⬎15% strategy and were thus dominated by the less costly absolute risk treatment strategies in the costeffectiveness analysis. The overall rankings were unchanged when outcomes were assessed in terms of years of life gained. Sensitivity Analyses Although there were some changes in the absolute values for the incremental cost-effectiveness ratios over the range of values tested, the only univariate sensitivity analysis that altered the rank order of health benefits or costs of the drug treatment strategies was the annual cost of hypertension treatment (Figure 2). We varied the annual cost of hypertension from $43 to $192 to reflect a range from one half to 2 times our baseline assumption of $86. We found a threshold point of $53 below which the absolute risk of CVD ⬎40% strategy cost less and increased the number of life-years gained compared with the “no-treatment” strategy. In this high-risk population, the number needed to treat to prevent 1 event was low enough that below $53 per year of treatment, the reduction in costs from preventing events was greater than the cost of treating those who would not have an event over the 10 years. Above $53 per year of antihypertensive therapy, the ranking of the strategies was the same as in the base case, Figure 2. Sensitivity analysis on cost of hypertension treatment. One-way sensitivity analysis showing the impact of varying the costs of hypertension treatment on the incremental costeffectiveness ratios of the guidelines that were compared in this study. The 1996 South African guidelines and the JNC VI guidelines are excluded because they were dominated strategies. AR indicates 10-year absolute risk for CVD event. 3574 Circulation December 6, 2005 Figure 3. Sensitivity analysis on relative risk reduction of coronary heart disease. One-way sensitivity analysis showing the impact of varying the relative risk reduction of treatment of hypertension compared with nontreatment on the incremental cost-effectiveness ratios of the guidelines compared. The 1996 South African guidelines and the JNC VI guidelines are excluded because they were dominated strategies. AR indicates 10-year absolute risk for CVD event. Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 with no treatment having the lowest costs and benefits and the 4 absolute risk strategies each with successive incremental cost-effectiveness ratios. Furthermore, the incremental ratios were quite sensitive to the increasing cost of hypertension treatment. For example, the incremental cost-effectiveness ratio for the absolute risk of CVD ⬎30% strategy ranged from $300 to nearly $5000/QALY when the annual cost of antihypertensive therapy was increased from $43 to $186. Figure 3 displays that when the relative risk reduction of coronary heart disease from hypertensive therapy was assessed over the range from 15% to 25%, the incremental cost-effectiveness ratio increased inversely with the amount of benefit of treatment. At an assumed reduction in coronary heart disease events of 25% with treatment, the absolute risk of CVD ⬎40% strategy had an incremental cost-effectiveness ratio of $400/QALY, but with an assumed risk reduction of 15%, the ratio was $900/QALY. Plausible variations in each of the other remaining variables listed in Table 1 did not change the rank ordering of the strategies, and the costeffectiveness ratios never varied by more than 50% from the base case. Furthermore, under the full range tested for each variable in the univariate sensitivity analyses, the 1995 South African guidelines and the JNC-VI– based guidelines remained dominated by the absolute risk threshold treatment strategies. The probabilistic multivariate sensitivity analysis using the 6 above-mentioned variables revealed little variation from the base case and no change in the order of the strategies with any of the iterations. For example, the mean incremental ratio when we compared absolute risk of 30% versus 40% was $1600/QALY, with 95% of the values within $200 of that figure. The range was similar for each of the other comparisons having nondominated strategies, with 95% of the values of incremental ratios varying by less than $200/QALY from the base-case results. Discussion On the basis of the results of our population-based simulation model, we conclude that for the current South African population, hypertension guidelines based on an absolute risk for cardiovascular disease are both more effective at saving lives and less costly than those based predominantly on a blood pressure level. This approach is even more attractive if the cost of treatment could be reduced. We modeled the cost of hypertension treatment based on the current mix of medications used in South Africa. If the use of thiazides replaces the more expensive calcium channel blockers or ACE inhibitors, then the cost-effectiveness ratios for primary prevention will be further reduced, and the absolute risk strategies will be even more attractive, if not economically dominant, compared with no treatment. Furthermore, the conventional blood pressure– based guidelines remained more costly and less effective with each univariate and multivariate sensitivity analysis. We recognize that our model is based on limited cost data, which is a significant problem throughout the developing world. However, given that we applied the same costs of treatment to all the intervention strategies, the result seen in the sensitivity analysis still showed that the blood pressure level guidelines were always dominated throughout the assessed ranges of costs. Certainly, the costs of interventions could be much lower if generic medications were used instead of the current pattern of use of both patented and generic drugs in South Africa. Thus, our estimates are likely conservative. The choice of which absolute risk threshold might be appropriate for South Africa can be guided by either a comparison with what the country is currently doing or by some other international standard. On the basis of our model, switching from its current guidelines to one of treating those with an absolute risk of CVD of ⬎15% could save the South African society up to US $500 million over 10 years without any decrement in the QALYs achieved under its current guidelines. Alternatively, the Commission on Macroeconomics and Health recommended choosing interventions that were less than 3 times the gross domestic product (GDP) per capita. This figure would be $9000/QALY if we used the Gaziano et al Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 GDP figure ($3000/capita) from 2002 and would be consistent with the decision to treat all those at absolute risk of CVD ⬎20%. However, under this criterion, the absolute risk of 15% strategy would also be acceptable if a greater proportion of generic medications, such as hydrochlorothiazide, were used. The use of absolute risk– based guidelines is relatively new; however, guidelines that are based on absolute cardiovascular risk are more sensitive at predicting those at highest risk. They have been shown in a model of coronary heart disease in New Zealand to predict fewer cardiovascular events than those based on a blood pressure level when applied to people with the same risk factors.35 The present findings are consistent with the WHO CHOICE by Murray et al7: The absolute risk approach also had lower costeffectiveness ratios than the target-level approach. The present study extends their findings in 3 distinct ways. First, we looked at a specific country with more detailed epidemiological and cost data. This allows an individual country like South Africa to shift resources based on its specific health needs and budgetary limitations. It allows a direct comparison of the 2 possible approaches under consideration and evaluation of what a change from its current approach to a new one might entail. Second, our model included inpatient costs of CVD events. Given that these events are responsible for a significant proportion of costs related to a blood pressure and CVD prevention program, our costs more likely reflect actual costs associated with the intervention. Finally, given that we had specific country information, we were able to validate our model. Recent recommendations with regard to guidelines suggest that they should be simple and easy for various types of clinicians to follow.7 The exact risk of developing CVD can be calculated with risk calculators found on a variety of Internet Web sites. All that is needed is the specific risk factor profile for the individual being evaluated, information that is identical to what is needed to use the JNC VI guidelines. Additionally, a recent study in a busy primary care setting in the United Kingdom found that use of a chart based on absolute risk calculations was well-liked, easy to use, and resulted in a clinically significant reduction in blood pressure compared with usual care.36 One limitation is that the absolute risk approach uses the Framingham function, which is based on a predominantly US white population. However, it has been shown to be equally predictive among white and black men and women in the United States.37 Furthermore, the case-control INTERHEART38 study confirmed that similar risk factors accounted for the majority of myocardial infarction regardless of region. Also, although many of our assumptions about risk assessment and treatment effects were based on Western data, the model is validated well within the range of limited estimates published on South Africa. Nonetheless, a cohort study examining the CVD risk function in South Africans would allow for refinement of our model and is an obvious area for future exploration. Further generalization of our results to other developing countries should take into account the fact that the risk score may overestimate or underestimate disease, CEA of Hypertension Guidelines in South Africa 3575 which would increase or decrease the incremental costeffectiveness ratios, respectively. Acknowledgments The first author would like to express gratitude to Eugene Braunwald of Harvard Medical School for inspiration and his encouragement to pursue this project at the Cape Heart Centre of the University of Cape Town in South Africa as a Lancet International Fellow. Further acknowledgement goes to Cynthia Young, research assistant, for help in preparation of this manuscript. The authors report no conflicts of interest. References 1. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990 –2020: Global Burden of Disease Study. Lancet. 1997; 349:1498 –1504. 2. Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ, Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360: 1347–1360. 3. Williams B, Poulter NR, Brown MJ, Davis M, McInnes GT, Potter JF, Sever PS, Thom SM, British Hypertension Society. Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society, 2004-BHS IV. J Hum Hypertens. 2004;18: 139 –185. 4. National Health Committee. Guidelines for the Management of Mildly Raised Blood Pressure in New Zealand. Wellington, New Zealand: Ministry of Health; 1995. 5. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JLJ, Jones DW, Materson BJ, Oparil S, Wright JTJ, Roccella EJ. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560 –2572. 6. Yikona JI, Wallis EJ, Ramsay LE, Jackson PR. Coronary and cardiovascular risk estimation in uncomplicated mild hypertension: a comparison of risk assessment methods. J Hypertens. 2002;20:2173–2182. 7. Murray CJ, Lauer JA, Hutubessy RC, Niessen L, Tomijima N, Rodgers A, Lawes CM, Evans DB. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: a global and regional analysis on reduction of cardiovascular-disease risk. Lancet. 2003;361: 717–725. 8. Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases, part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation. 2001;104:2746 –2753. 9. South African Hypertension Society Executive Committee. Hypertension clinical guideline 2000. S Afr Med J. 2001;91:163–172. 10. Milne FJ, Pinkney-Atkinson VJ. Hypertension guideline 2003 update. S Afr Med J. 2004;94:209 –216,218,220 –225. 11. The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med. 1997;157:2413–2446. 12. Steyn K, Gaziano TA, Bradshaw D, Laubscher R, Fourie J, South African Demographic and Health Coordinating Team. Hypertension in South African adults: results from the Demographic and Health Survey, 1998. J Hypertens. 2001;19:1717–1725. 13. Hypertension Society of Southern Africa. Guidelines for the management of hypertension at primary health care level. S Afr Med J. 1995;85: 1321–1325. 14. Report of the Census Evaluation Task Team of the Statistics Council on the Final Post-Enumeration Survey Adjusted Count of the 1996 Population Census. Pretoria, South Africa; Statistics South Africa; 1996. 15. Seedat YK, Mayet FG, Khan S, Somers SR, Joubert G. Risk factors for coronary heart disease in the Indians of Durban. S Afr Med J. 1990;78: 447– 454. 16. Levitt NS, Katzenellenbogen JM, Bradshaw D, Hoffman MN, Bonnici F. The prevalence and identification of risk factors for NIDDM in urban Africans in Cape Town, South Africa. Diabetes Care. 1993;16:601– 607. 17. Levitt NS, Steyn K, Lambert EV, Reagon G, Lombard CJ, Fourie JM, Rossouw K, Hoffman M. Modifiable risk factors for type 2 diabetes mellitus in a peri-urban community in South Africa. Diabet Med. 1999; 16:946 –950. 3576 Circulation December 6, 2005 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 18. Steyn K, Jooste PL, Langenhoven ML, Benade AJ, Rossouw JE, Steyn M, Jordaan PC, Parry CD. Coronary risk factors in the coloured population of the Cape Peninsula. S Afr Med J. 1985;67:619 – 625. 19. Rossouw JE, Jooste PL, Chalton DO, Jordaan ER, Langenhoven ML, Jordaan PC, Steyn M, Swanepoel AS, Rossouw LJ. Community-based intervention: the Coronary Risk Factor Study (CORIS). Int J Epidemiol. 1993;22:428 – 438. 20. Anderson KM, Odell PM, Wilson PW, Kannel WB. Cardiovascular disease risk profiles. Am Heart J. 1991;121:293–298. 21. Dorrington R, Bradshaw D, Wegner T. Estimates of the level and shape of mortality rates in South Africa around 1985 and 1990 derived by applying indirect demographic techniques to report deaths. In: CERSA Technical Report. Cape Town, South Africa: Medical Research Council; 1999. 22. Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: a risk profile from the Framingham Study. Stroke. 1991;22: 312–318. 23. Murray CJ, Lopez AD. The Global Burden of Disease: a Comprehensive Assessment of Mortality and Disability From Diseases, Injuries and Risk Factors in 1990 and Projected to 2020. Cambridge, Mass: Harvard University; 1996. 24. MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, Abbott R, Godwin J, Dyer A, Stamler J. Blood pressure, stroke, and coronary heart disease, part 1: prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet. 1990;335:765–774. 25. Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, Godwin J, Qizilbash N, Taylor JO, Hennekens CH. Blood pressure, stroke, and coronary heart disease, part 2: short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990;335:827– 838. 26. Edwards PR, Lunt DW, Fehrsen GS, Lombard CJ, Steyn K. Improving cost-effectiveness of hypertension management at a community health centre. S Afr Med J. 1998;88:549 –554. 27. South African Medical Association. Guide to Fees for Medical Services 2000. Cape Town, South Africa: Health & Medical Publishing, Inscape Press; 1999. 28. Pestana JA, Steyn K, Leiman A, Hartzenberg GM. The direct and indirect costs of cardiovascular disease in South Africa in 1991. S Afr Med J. 1996;86:679 – 684. 29. Gold MR, Siegel JE, Russell LB, Weinstein MC, eds. Cost-Effectiveness in Health and Medicine. New York, NY: Oxford University Press; 1996. 30. Doubilet P, McNeil BJ, Weinstein MC. The decision concerning coronary angiography in patients with chest pain: a cost-effectiveness analysis. Med Decis Making. 1985;5:293–309. 31. Bradshaw D, Botha H, Joubert G, Pretorius J, van Wyk R, Yach D. Review of South African Mortality 1984. Parow, South Africa: Medical Research Council; 1987. 32. Bradshaw D, Dorrington RE, Sitas F. The level of mortality in South Africa in 1985: what does it tell us about health? S Afr Med J. 1992;82: 237–240. 33. Central Statistical Service. South Africa Life Tables 1984 –1986. Pretoria, South Africa: Government Printer; 1987. 34. Rosman KD. The epidemiology of stroke in an urban black population. Stroke. 1986;17:667– 669. 35. Baker S, Priest P, Jackson R. Using thresholds based on risk of cardiovascular disease to target treatment for hypertension: modelling events averted and number treated. BMJ. 2000;320:680 – 685. 36. Montgomery AA, Fahey T, Peters TJ, MacIntosh C, Sharp DJ. Evaluation of computer based clinical decision support system and risk chart for management of hypertension in primary care: randomised controlled trial. BMJ. 2000;320:686 – 690. 37. D’Agostino RB Sr, Grundy S, Sullivan LM, Wilson P, CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA. 2001;286:180 –187. 38. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L, Interheart Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364:937–952. Cost-Effectiveness Analysis of Hypertension Guidelines in South Africa: Absolute Risk Versus Blood Pressure Level Thomas A. Gaziano, Krisela Steyn, David J. Cohen, Milton C. Weinstein and Lionel H. Opie Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Circulation. 2005;112:3569-3576 doi: 10.1161/CIRCULATIONAHA.105.535922 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2005 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/112/23/3569 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/