Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
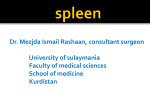
All you need to know about splenic arterial embolisation (or almost) Poster No.: C-1875 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: A. Zugazaga, P. Bermúdez, A. Darnell, A. Alguersuari, D. Rodriguez, A. Torremadé, J. Branera, J. R. Fortuño; Sabadell/ES Keywords: Spleen, Embolization, Interventional radiology DOI: 10.1594/ecr2010/C-1875 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 34 Learning objectives • To review the anatomy of the splenic artery and the spectrum of indications for splenic artery embolization. • To describe the different techniques for splenic artery embolization and possible complications. Background Splenic artery embolization is becoming increasingly common in interventional radiology. It is performed to treat different emergent or chronic diseases, including abdominal trauma, hypersplenism, splenic arterial aneurysm and pseudoaneurysm. The limitations of each possible management approach have yet to be clearly defined. We will try to shed some light on the situation. Splenic vascular anatomy Figure 1, 2 & 3 The spleen plays an important role in the immune system, defending against microorganisms that enter the circulation. Thus, avoiding splenectomy can help preserve immune function. The splenic artery supplies the spleen and distal portions of the stomach and pancreas. It courses along the superior edge of the pancreas in close relation to the splenic vein. Near the splenic hilum, the artery usually divides into superior and inferior branches, and each branch further divides into various intrasplenic branches. Page 2 of 34 The inferior polar artery usually gives rise to the left gastroepiploic artery. Numerous short gastric branches arise from the terminal splenic or left gastroepiploic artery to supply the gastric cardia and fundus. The splenic artery has many branches that supply the pancreatic body and tail. The first large branch is the dorsal pancreatic artery, which arises from the proximal splenic artery, and the second large branch is the greater pancreatic artery (or arteria pancreatica magna), which arises from the middle segment of the splenic artery. When embolization is planned, visualization of the pancreatic arteries and gastric branches is essential to reduce the risk of their unintended embolization. Images for this section: Page 3 of 34 Fig. 1 Page 4 of 34 Fig. 2 Page 5 of 34 Fig. 3 Page 6 of 34 Imaging findings OR Procedure details Our experience Between January 2001 and July 2009, we treated 15 patients (10 men and 5 women; mean age=58 years, range 33-80) , by splenic artery embolization. All patients had undergone abdominal CT prior to the procedure. The different diagnoses were: posttraumatic splenic injuries in 7 patients, splenic artery pseudoaneurysm due to pancreatitis in 3, hypersplenism in 3, and aneurysms in 2. Materials used for embolization included gelatin sponge pledgets, polyvinyl alcohol particles, and coils. We treated 7 patients using only coils, 2 using PVA particles and coils in combination, 6 using coils and sponge pledgets in combination. We used proximal embolization in most patients. The procedure was effective in 13 of 15 patients. Major complications were 1 abscess and 1 pancreatic fistula. The abscess occurred after coil and sponge pledgets embolization of a pseudoaneurysm secondary to chronic pancreatitis, and it was treated by percutaneous drainage. The pancreatic fistula was a postoperative complication in a patient with hypersplenism who was first treated with proximal splenic artery embolization with coils and particles. The fistula resolved with conservative management. Next we will examine the different scenarios where splenic artery embolization plays an important role. 1. Trauma The spleen is the most frequently injured solid organ in blunt abdominal trauma in both adults and children. Other less common causes of splenic injuries include penetrating abdominal trauma, iatrogenic injury (surgery, endoscopy or biopsy), and spontaneous rupture. Surgery was long the only possible management in patients with traumatic injuries. The increased susceptibility of patients to infections after splenectomy led to the development spleen-conserving procedures. This trend is based on experiences in pediatric patients, where the nonoperative management (NOM) of splenic injuries has gained wide acceptance. When successful, NOM enables spleen immune function to be preserved Page 7 of 34 and avoids the morbidity associated with nontherapeutic laparotomy (theoretical potential of decreasing hospital length of stay and blood transfusion requirements). As a result, in most trauma centers, NOM is now the treatment of choice in hemodynamically stable patients. Failure rates of NOM in most current studies range from 3% to 18%. Splenic artery embolization (SAE) has played an increasingly important role in this nonoperative approach, leading to decreased failure rates of NOM. • Diagnosis The accurate diagnosis of splenic injury is of the utmost importance in the evaluation of trauma patients. Multidetector computed tomography (MDCT) allows accurate identification and characterization of splenic injuries. Hemodynamically unstable patients are not suitable candidates for CT and are typically evaluated with diagnostic peritoneal lavage (DPL) or ultrasound focused abdominal sonography in trauma (FAST) to detect hemoperitoneum and enable prompt treatment. However, in hemodynamically stable patients, MDCT has become the gold standard for the diagnosis of splenic injuries after trauma. CT has an accuracy exceeding 95% in the detection of splenic injuries when meticulous CT technique is used. Artifacts from patients' arms, external wires, or nasogastric tubes should be minimized. The administration of intravenous contrast is mandatory for the correct evaluation of the spleen and the rest of the abdomen. Contrast material is routinely administered intravenously with a power injector, images are obtained 60 to 70 seconds after the start of the injection to obtain a portal phase. Arterial phase images or delayed images obtained about 2 to 3 minutes after contrast injection can be useful to demonstrate an increased volume of extravasation of contrast material. Assessment of splenic injury should include evaluation for hematoma, laceration, vascular injuries, and active hemorrhage. Splenic hematomas are seen as low-density collections of blood, iso/hypodense relative to spleen in contrast-enhanced CT images. Hematomas can be intraparenchymal, subcapsular, or perisplenic. On CT lacerations appear as low-attenuation lines that extend partially or completely across the spleen; lacerations can be single, multiple, or stellate. Splenic fractures are defined as lacerations that extend completely across the spleen, commonly involving the hilum. Vascular pedicle injuries usually result in significant hemorrhage and cardiovascular instability, and patients are not referred for CT evaluation. The CT appearance of these Page 8 of 34 lesions is nonenhancement of the lower pole of the spleen with preservation of upper pole perfusion through the short gastric arteries. Active hemorrhage appears as areas of irregular extravasated contrast that can be distinguished from blood by its density (> 100 HU). Table - American Association for the Surgery of Trauma. Splenic Injury Scale. Figure 1&2 Grade Lesion Injury Description I Hematoma Subcapsular, nonexpanding, surface area Laceration <10% of Capsular tear, nonbleeding parenchymal depth < 1 cm II Hematoma Laceration Subcapsular, nonexpanding, 10%-50% of surface area; Intraparenchymal, nonexpanding, <5 cm in diameter Capsular tear, active bleeding; 1 cm -3 cm parenchymal depth that does not involve a trabecular vessel III Hematoma Laceration Subcapsular, >50% of surface area or expanding; Ruptured hematoma bleeding; subcapsular with active Intraparenchymal hematoma >5 cm expanding or Page 9 of 34 Parenchymal depth >3 cm or involving trabecular vessels IV Hematoma Laceration Ruptured intraparenchymal hematoma with active bleeding Laceration involving segmental or hilar vessel producing major devascularization (>25% of spleen) V Laceration Completely spleen shattered Vascular Hilar vascular injury that devascularizes spleen Splenic pseudoaneurysms are a rare but life-threatening complication of splenic injury after blunt abdominal trauma and are defined as well-defined focal contrast blush. Pseudoaneurysms are differentiated from contrast extravasation because they appear isodense to the adjacent vascular structures on delayed images, while contrast extravasation shows no change in density. • Indications of SAE The use of endovascular therapy for controlling hemorrhage from the damaged spleen was first reported in 1981. The classic indications for SAE include lesions involving a high risk of secondary rupture of the spleen, such as splenic trauma with contrast extravasation or pseudoaneurysm on CT scan. Although more liberal indications have been described, the routine use of SAE is questioned by other authors. The addition of SAE to NOM has proven feasible, safe, and effective in increasing rates of splenic salvage. The procedure is particularly beneficial in severe splenic injuries that previously required laparotomy and were more likely to lead to the failure of NOM. The following algorithm is currently recommended by the American Association for the Surgery of Trauma (AAST): Figure 3 on page 19 In summary, angiography is indicated in hemodynamically stable patients with grade III-V splenic lesions on CT and/or active contrast extravasation and/or splenic vascular injury Page 10 of 34 on CT. Of course, the final decision and the success of the treatment will depend on good teamwork between surgeons and radiologists. • Technique The success rate of splenic embolization ranges from 75% to 100%. Two primary techniques of splenic artery embolization have been described: 1. Proximal 2. Super selective distal embolization. In proximal embolization, the splenic artery is selectively catheterized; the tip of the catheter must be placed beyond the origin of the dorsal pancreatic artery. Then, embolic coils (the size of which is very important) are placed to occlude blood flow. The surgical equivalent of this procedure is splenic artery ligation. Proximal embolization performed exclusively with coils decreases the volume of splenic arterial blood flow and thereby produces relative hypotension in the splenic bed, which allows the spleen to repair itself without infarction. By reducing splenic blood flow and arterial pressure, bleeding ceases and the collateral supply from the left gastric artery, short gastric branches, dorsal pancreatic artery, and pancreatic or duodenal arcades, as well as omental gastroepiploic collaterals, will provide an alternative blood flow maintaining the viability of the spleen. The endpoint of embolization is still controversial, but it is clear that the objective of embolization is to reduce the pressure in the splenic parenchyma to decrease its risk of bleeding and help the spleen heal and reconstitute the blood supply through collateral vessels. In super selective distal embolization, a microcatheter is advanced as close as possible to the site or sites of vascular injury. Then, embolic agents are used with or without small coils. This achieves hemostasis in the injured spleen while preserving perfusion to the remaining. However, subsequent bleeding may occur because some vascular injuries may initially go unnoticed due to vasospasm. Reportedly, approximately 70% of pseudoaneurysms are missed on initial CT examination and discovered on follow-up CT. Moreover, there is some evidence suggesting that distal embolization may be associated with more frequent splenic infarcts. For all these reasons, proximal embolization is the technique of choice for the management of blunt splenic injuries. At angiography, frank extravasation is rare, and abrupt vessel truncation, arteriovenous fistula, or pseudoaneurysm are more common findings. Page 11 of 34 Here there some examples: Figure 4 on page 20, Figure 5 on page 21, Figure 6 on page 22 2. Hypersplenism Splenectomy or transcatheter ablation of splenic parenchyma are often performed for the management of hypersplenism, a pathologic condition that is characterized by increased pooling or destruction of the corpuscular elements of the blood by the spleen. It may be seen in many disorders, including cirrhosis with portal hypertension, hematological abnormalities, and diffuse splenic infiltration from primary malignancies such as leukemia and lymphoma. Signs of hypersplenism include splenomegaly, thrombocytopenia, leukopenia, and anemia. Total splenectomy may be an effective treatment for hypersplenism, but it impairs the body's ability to produce antibodies against encapsulated microorganisms and predisposes patients to sepsis. After splenectomy, the treated condition may recur, with the possible result that a second surgery or additional transfusion will be needed. Furthermore, patients who have comorbid conditions and severe cytopenia are not considered candidates for surgery. However, the removal of functional splenic tissue may improve hematological abnormalities related to bone marrow suppression from systemic chemotherapeutic and immunosuppressive agents, so that optimal doses of such medications can be maintained. In 1973, Madison reported the initial clinical experience with splenic arterial embolization. • Indications: 1. Preoperative 2. Definitive treatment 1. Although proximal arterial occlusion is ineffective for the management of hypersplenism, it is useful as a preoperative technique for reducing intraoperative blood loss in patients undergoing open or laparoscopic splenectomy. Moreover, in laparoscopic Page 12 of 34 splenectomy, splenic artery embolization can lead to a reduction in splenic size, which may help improve the surgical view and intraoperative exposure. Presently, laparoscopic splenectomy is the treatment of choice in the surgical management of splenomegaly. Many reports suggest the clinical benefit of preoperative splenic artery embolization, especially in patients with severe splenomegaly (larger than 20 cm). The most widely accepted technique in these cases is proximal embolization (the same as described above for traumatic lesions). 2. Splenic arterial embolization has also been advocated for the intentional infarction of splenic tissue to reduce its consumptive activity. Initial experiences with this modality of treatment led to severe complications of complete splenic infarction, preventing its acceptance as a viable treatment option. However, many authors recommend incomplete or partial splenic arterial embolization, in which a portion of the splenic parenchyma is left viable, to preserve the spleen's immunologic function. Partial splenic arterial embolization was first considered a viable option when initial attempts to treat hypersplenism with proximal splenic arterial occlusion were unsuccessful. Treatment failures were attributed to abundant collateral circulation (especially through short gastric and gastroepiploic arteries) that re-entered around the occluded segment of the splenic artery reestablishing the splenic blood supply. Partial splenic embolization may be performed with one of two methods: In the first approach, a few distal branches of the splenic artery are selectively catheterized and embolized to achieve complete stasis in these branches while several other branches are left untreated. Parenchymal phase angiograms may be used to estimate the volume of the remaining viable splenic tissue. Additional branches then may be catheterized, and embolization may be repeated, until the desired effect is achieved. In the second approach, nonselective partial embolization, the working catheter tip is positioned more proximally in the main splenic artery but beyond the origin of the major pancreatic branches. Embolic particles are injected until the parenchymal blush is reduced. We can use different embolic agents, most frequently gelfoam pledgets and PVA particles. The Spigos technique to minimize complications includes 1. Aseptic technique 2. Antibiotic coverage 3. Avoidance of excessive infarction of splenic mass. Hematological response and the severity of complications correlate with the amount of infarcted splenic tissue. Most interventionalists aim to achieve infarction in 60% to 70% of the plenic mass. Page 13 of 34 4. Effective postembolization analgesia Here is an example: Figure 7 on page 23 3. Portal hypertension Endoscopic obliteration of gastroesophageal varices and creation of a transjugular intrahepatic portosystemic shunt are the two most common options used to manage variceal hemorrhage in cirrhotic patients with portal hypertension. Open or laparoscopic splenectomy has been proposed, but it has not gained wide acceptance because of the high risk of complications. Partial splenic embolization appears to be efficacious in reducing episodes of variceal bleeding, improving hematologic parameters, enhancing hepatic protein synthesis, and reducing the severity of hepatic encephalopathy. The reduction of splenic volume results in a decrease in venous drainage and, thus, in a reduction in portal venous flow and pressure. Associated morbidity and mortality appear to be acceptable. Embolization may be performed alone or in combination with other therapeutic interventions, such as endoscopic ligation. The literature, however, is limited. Given the potential benefits of partial splenic embolization, further investigation is warranted to allow evidence-based evaluation of its use. We do not have any experience in splenic artery embolization to treat portal hypertension. 4. Splenic artery aneurysm The splenic artery is the most frequent site of visceral arterial aneurysms with a prevalence of 0.8%. Most of them are small (<2 cm), saccular, and located in the intermediate or distal segment of the splenic artery. They are multiple in 20% of cases. Most splenic artery aneurysms are detected incidentally during diagnostic imaging performed for other indications. Rupture is rare but associated with a high mortality rate. Page 14 of 34 • Indications for treatment Cases with specific symptoms (e.g., back or epigastric or left upper quadrant pain), female sex and childbearing age, planned liver transplantation, portal hypertension, and aneurysms with a diameter of greater than 2.5 cm should be treated. Various therapeutic options are available to treat splenic artery aneurysms. Traditional surgical management is the recommended repair in low-risk patients with asymptomatic aneurysms greater than 20 mm in diameter or with rapidly growing aneurysms. During the past decade, endovascular techniques have been advocated as an alternative to treat these aneurysms. Percutaneous interventional techniques are associated with lower morbidity and mortality compared to surgical modalities. • Technique Packing of the aneurysmal sac with embolic agents (most commonly with coils, but also with detachable balloons and inert particles) and exclusion of the aneurysmal neck with the "sandwich" method are the recommended techniques for treating splenic artery aneurysms. Precise selection of the occlusion site is necessary to preserve collateral blood flow to the spleen via the gastric, omental, and pancreatic vessels. The "remodeling" technique used to treat intracranial aneurysms has also been used for widenecked aneurysms. Success rates of embolization are between 80% and 90%. Stent-graft placement to exclude the aneurysm and preserve blood flow through the splenic artery has also been reported. Percutaneous needle puncture of the aneurysm and administration of thrombin into the aneurysm may be another therapeutic option when embolization is not possible or has failed. Imaging follow-up (Doppler ultrasonography or CT, which is more sensitive) is recommended to determine whether the aneurysm is completely occluded. Here is an example: Figure 8 on page 24 5. Splenic artery pseudoaneurysm Chronic pancreatitis causes vascular complications, including pseudoaneurysms of the peripancreatic arteries. Splenic artery pseudoaneurysms are the most common visceral artery pseudoaneurysms. They have been reported to develop in about 10% of cases Page 15 of 34 of pancreatitis. Splenic pseudoaneurysms appear to develop as a consequence of inflammatory processes adjacent to the splenic artery, particularly acute and chronic pancreatitis with associated pseudocysts. Proteolytic pancreatic enzymes may digest the arterial wall and cause pseudoaneurysms. They are often asymptomatic. Complications include rupture with retroperitoneal or intraperitoneal hemorrhage. They can rarely rupture into the gastrointestinal tract. The clinical presentation of pseudoaneurysm rupture includes acute abdominal pain, hematemesis, and melena. When such symptoms are present in a patient with pancreatitis, a vascular complication should be suspected and a prompt diagnosis is essential because treatment is mandatory. Color duplex sonography and especially contrast-enhanced MDCT are essential for the detection of vascular complications. Although surgical treatment traditionally played the major role, recent advances in interventional radiology have made arterial embolization well suited for treating splenic artery pseudoaneurysms. Identification of the bleeding vessel during surgery is problematic due to peripancreatic inflammation, necrosis, and friability, which can make it impossible to control bleeding. • Technique Several techniques (mostly the same as in splenic artery aneurysms) have been described for the interventional radiology treatment of splenic pseudoaneurysms. Although theoretically all modalities could be effective, the great fragility of the pseudoaneurysmatic wall contraindicates most of them. Therefore, embolization of both distal and proximal vessels (the "sandwich technique" Figure 9 on page 25) is generally believed to be the best procedure. Coils, which achieve permanent embolization without increasing the intravascular pressure, are the most common embolic materials in the treatment of pseudoaneurysms. In this context, temporary occlusion of the splenic artery using a balloon catheter can be useful for controlling splenic arterial flow and preventing distal coil migration. A gelatin sponge is also an option. However, because it might induce rupture by increasing intravascular pressure during infusion, it must be applied in specific situations: (1) in combination with coils, where it would function as an adjuvant to stimulate thrombus formation by increasing blood flow stagnation; (2) to embolize small vessels in which deployment of coils is difficult; and (3) when treating multiple bleeding sites. Here is another example: Figure 10 on page 26 Complications of embolization Page 16 of 34 The use of total splenic infarction has been limited because of the high incidence and severity of complications such as splenic abscess (Figure 10 on page 26), splenic rupture, bacteremia, splenic vein thrombosis, and unremitting bronchopneumonia. Unlike in other organ systems, the presence of air in the spleen does not always indicate abscess formation. Splenic abscesses occur in a small percentage of patients and may be successfully managed percutaneously or intraoperatively. Salvage rates are similar whether embolization is performed in an arterial segment distal or proximal to the origin of the splenic artery. Several mechanisms may cause complications after complete splenic infarction: induced immunosuppression, anaerobic bacterial growth in the hypoxic tissue, percutaneous introduction of exogenous bacteria, and retrograde transport of enteric pathogens via reversed portal flow. Like complete splenic ablation, partial splenic arterial embolization and proximal embolization (for splenic artery aneurysm) may entail complications and adverse effects, but these procedures are better tolerated than complete splenic ablation. In addition, patients may develop pleural effusions that require thoracentesis; paralytic ileus; pancreatitis (likely a result of nontarget embolization of the dorsal pancreatic or greater pancreatic artery); or postembolization syndrome, which consists of fever, leukocytosis, and abdominal pain. In general, major complications are rare and it is difficult to quantify them because of the inhomogeneous data from the different series. Splenic function after embolization has not been thoroughly evaluated. Several small studies have demonstrated preserved splenic function after surgical splenic artery ligation based on pathological findings. Thus, as proximal embolization mimics surgical splenic artery ligation, it is reasonable to theorize that it also preserves splenic function. Although there are some encouraging findings, large prospective studies are needed. Page 17 of 34 Images for this section: Fig. 1: A: splenic laceration (grade II), B: subcapsular and perisplenic hematoma (grade III), C: splenic fracture (grade IV) Page 18 of 34 Fig. 2: D: shattered spleen (grade V) with post-traumatic pseudoaneurysm, E: splenic laceration with perisplenic hematoma and active bleeding (grade IV) Page 19 of 34 Fig. 3: Algorithm of the AAST Page 20 of 34 Fig. 4: A 36-year-old man injured in a head-on automobile accident. A: CT shows laceration (grade IV) with perisplenic hematoma and active bleeding (arrow), B: DSA shows an extensive hypovascular lesion, C: proximal embolization with coils to reduce the pressure, D: CT postembolization shows a normal sized-spleen with small hypoattenuating areas that correspond to infarcts. No surgery was needed in this patient. Page 21 of 34 Fig. 5: A 41-year-old man involved in a bicycle accident. A: CT shows a splenic laceration (grade II) with perisplenic hematoma, B: CT two days after A shows the formation of a posttraumatic pseudoaneurysm (arrow). Note that the hyperenhancing nodular image seen in the arterial phase disappears in the portal phase, C: DSA with multiple nodular images secondary to pseudoaneurysms, D: proximal embolization of the splenic artery, E: CT postembolization shows resolution of the pseudoaneurysms and a residual splenic hematoma. No surgical measures were taken in this patient Page 22 of 34 Fig. 6: A 64-year-old woman involved in an automobile accident. A: CT shows splenic lacerations (grade III) and hyperenhancing nodular images that correspond to pseudoaneurysms (arrow), B: DSA shows multiple pseudoaneurysms (note that no active extravasation is visualized), C: proximal embolization of the splenic artery. No surgical measures were taken in this patient Page 23 of 34 Fig. 7: A 57-year-old man with lymphoproliferative disease and splenomegaly. A: CT shows a giant splenomegaly, with peripheral triangular, hypoattenuating images that correspond to infarcted areas (arrow), B: DSA shows the same as the CT, C: proximal embolization D: macroscopic specimen. Embolization was performed before splenectomy to reduce the risk of bleeding Page 24 of 34 Fig. 8: An asymptomatic 71-year-old woman with an incidentally found splenic artery aneurysm. US (A) and MR angiogram (B) show a splenic artery aneurysm, C: DSA confirms MR findings, D: DSA post-coling the aneurysm, E: Postembolization CT shows a splenic infarct. Page 25 of 34 Fig. 9: "Sandwich technique" Page 26 of 34 Fig. 10: A 59-year-old man with chronic pancreatitis. Pseudoaneurysm formation after a relapse of acute disease. A: CT shows a hypodense collection in the pancreatic tail associated with splenic infarction, B: CT one week after A shows a hyperattenuating nodular image inside the collection that was due to the formation of a splenic pseudoaneurysm (red arrow), C: DSA shows a pseudoaneurysm, D: embolization by packing 2 coils to sandwich the pseudoaneurysm, E: CT after embolization, shows an splenic abscess due to splenic necrosis that was managed with percutaneous drainage. Page 27 of 34 Conclusion • Splenic arterial embolization may be used to treat a wide range of pathologic entities, so interventional radiologists require a thorough knowledge of the common indications, techniques, and complications. • We also believe that specific interdisciplinary protocols for each condition are mandatory. Personal Information # # A. Zugazaga , P. Bermúdez*, A. Darnell**, A. Alguersuari*, D. Rodriguez , A. # Torremadé , J. Branera*, J. R. Fortuño* # Radiology Resident * Vascular and Interventional Radiology Staff ** Abdominal Radiology Staff UDIAT-CD, Institut Universitari Parc Taulí - UAB Parc Taulí, 1 Page 28 of 34 08208 Sabadell SPAIN [email protected] [email protected] Images for this section: Page 29 of 34 Fig. 1 Page 30 of 34 References Haller JJ, et al. Nonoperative management of solid organ injuries in children: is it safe? Ann Surg 1994; 210:625-628. Raikhlin A, et al. Imaging and transcatheter arterial embolization for traumatic splenic injuries: review of the literature. J can chir, 2008 (51); 6: 466-472. Anderson S, et al. Blunt Splenic Trauma: Delayed-Phase CT for Differentiation of Active Hemorrhage from Contained Vascular Injury in Patients1. Radiology 2007; 243 (1): 88-95. Naoum JJ, et al. Concomitant intraoperative splenic artery embolization and laparoscopic splenectomy versus laparoscopic splenectomy: comparison of treatment outcome. The American Journal of Surgery 2007; 193, 713-718 Piffaretti G, et al. Splenic artery aneurysms: postembolization syndrome and surgical complications. American Journal of Surgery. 2007; 193, 166-170 Iwama Y, et. al. Transcatheter Embolization of Splenic Artery Pseudo-Aneurysm Rupturing into Colon After Post-Operative Pancreatitis. Cardiovasc Intervent Radiol (2006) 29:133-136 Guan YS, et al. Polyvinyl alcohol and gelatin sponge particle embolization of splenic artery pseudoaneurysm complicating chronic alcoholic pancreatitis. World J Gastroenterol 2005; 11(17):2684-2686 Kokonis KG. Partial splenic embolization in the treatment of patients with portal hypertension: a review of the english language literature. J Vasc Interven Radiol 2007 Apr;18(4):463-81. Romano M et al. Partial splenic embolization in patients with idiopathic portal hypertension. Eur J Radiol 2004 Mar;49(3):268-73 Velmahos GC, et al. Nonoperative management of splenic injuries: have we gone too far? Arch Surg 2000;135:674-679. Page 31 of 34 Splenic Arterial Interventions: Anatomy, Indications, Technical Considerations and Potential Complications David C. Madoff, MD et al. RadioGraphics 2005; 25:S191-211 Wahl WL, et al. Blunt splenic injury: operation versus angiographic embolization. Surgery 2004;136:891-899. Haan JM, et al. Splenic embolization revisited: a multicenter review. J Trauma 2004; 56:542-547. Poulin EC, et al. Splenic artery embolization before laparoscopic splenectomy: an update. Surg Endosc 1998;12:870-875. Images for this section: Page 32 of 34 Fig. 1 Page 33 of 34 Page 34 of 34