Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cross-species transmission wikipedia , lookup
Hepatitis C wikipedia , lookup
Bovine spongiform encephalopathy wikipedia , lookup
Oesophagostomum wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Onchocerciasis wikipedia , lookup
Meningococcal disease wikipedia , lookup
Chagas disease wikipedia , lookup
West Nile fever wikipedia , lookup
Schistosomiasis wikipedia , lookup
Brucellosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Bioterrorism wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Ebola virus disease wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Henipavirus wikipedia , lookup
Leptospirosis wikipedia , lookup
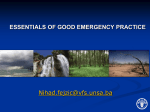
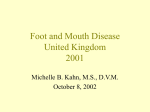
PERSPECTIVES 33. Costerton, J. W., Lewandowski, Z., Caldwell, D. E., Korber, D. R. & Lappin-Scott, H. M. Microbial biofilms. Annu. Rev. Microbiol. 49, 711–745 (1995). 34. Hall-Stoodley, L., Stoodley, P. & Costerton, J. W. Bacterial biofilms: from the natural environment to infectious diseases. Nature Rev. Microbiol. 2, 95–108 (2004). 35. Williams, H. N., Kelley, J. I., Baer, M. L. & Turng, B.-F. The association of bdellovibrios with surfaces in the aquatic environment. Can. J. Microbiol. 41, 1142–1147 (1995). 36. Koval, S. F. & Bayer, M. E. Bacterial capsules: no barrier against Bdellovibrio. Microbiology 143, 749–753 (1997). 37. Koval, S. F. & Hynes, S. H. Effect of paracrystalline protein surface layers on predation by Bdellovibrio bacteriovorus. J. Bacteriol. 173, 2244–2249 (1991). 38. Westergaard, J. M. & Kramer, T. T. Bdellovibrio and the intestinal flora of vertebrates. Appl. Environ. Microbiol. 34, 506–511 (1977). 39. Lenz, R. & Hespell, R. B. Attempts to grow bdellovibrios surgically injected into animal cells. Arch. Microbiol. 119, 245–248 (1978). 40. Scherff, R. H. Control of bacterial blight of soybean by Bdellovibrio bacteriovorus. Phytopathology 63, 400–402 (1973). 41. Varon, M. & Shilo, M. Attachment of Bdellovibrio bacteriovorus to cell-wall mutants of Salmonella spp. and Escherichia coli. J. Bacteriol. 97, 977–979 (1969). 42. Varon, M. Selection of predation-resistant bacteria in continuous culture. Nature 277, 386–388 (1979). 43. Alexander, M. Why microbial predators and parasites do not eliminate their prey and hosts. Annu. Rev. Microbiol. 35, 113–133 (1981). 44. Shemesh, Y. & Jurkevitch, E. Plastic phenotypic resistance to predation by Bdellovibrio and like organisms in bacterial prey. 6, 12–18 (2004). 45. Huang, S. S., Labus, B. J., Samuel, M. C., Wan, D. T. & Reingold, A. L. Antibiotic resistance patterns of bacterial isolates from blood in San Francisco County, California, 1996–1999. Emerg. Infect. Dis. 8, 195–201 (2002). 46. Schwudke, D. et al. The obligate predatory Bdellovibrio bacteriovorus possesses a neutral lipid A containing α-D-mannoses that replace phosphate residues: similarities and differences between the lipid As and the lipopolysaccharides of the wild-type strain B. bacteriovorus HD100 and its host-independent derivative HI100. J. Biol. Chem. 278, 27502–27512 (2003). 47. Wilkinson, M. H. F. Predation in the presence of decoys: an inhibitory factor on pathogen control of bacteriophages or bdellovibrios in dense and diverse ecosystems. J. Theor. Biol. 208, 27–36 (2001). 48. Stolp, H. & Petzold, H. Untersuchungen uber einen obligat parasitischen Mikroorganismus mit lytischer aktivitat fur pseudomonas bakterien. Phytopathogishe Zeithschrift 45, 364–390 (1962). 49. Stolp, H. & Starr, M. P. Bdellovibrio bacteriovorus gen. Et sp. N., a predatory, ectoparasitic, and bacteriolytic microorganism. Antonie Van Leeuwenhoek 29, 217–248 (1963). Acknowledgements The authors would like to thank R. Chaudhuri of Colibase, University of Birmingham, UK, for assistance with genome analysis. Their work is funded by the Wellcome Trust. Competing interests statement The authors declare that they have no competing financial interests Online links DATABASES The following terms in this article are linked online to: Entrez: http://www.ncbi.nlm.nih.gov/Entrez/ Bdellovibrio bacteriovorus HD100 | Buchnera aphidicola | CAE77837 | CAE78299 | CAE78505 | CAE78865 | CAE78875 | CAE79180 | CAE79394 | CAE79452 | CAE79454 | CAE80233 | CAE80242 | CAE80483 | CAE80640 | CAE81224 | RadA | RecA | RecG FURTHER INFORMATION B. bacteriovorus strain W: http://www.micro-gen.ouhsc.edu/b_bacter/b_bacter_home.htm Bacteriovorax marinus strain J: http://www.sanger.ac.uk/Projects/B_marinus/ Bdellovibrio genome project: http://www.eb.tuebingen.mpg.de/schuster/research_bd.htm/ R. Elizabeth Sockett’s laboratory: http://www.nottingham.ac.uk/biology/contact/academics/ sockett/research.phtml Access to this links box is available online. NATURE REVIEWS | MICROBIOLOGY OPINION The UK foot-and-mouth disease outbreak — the aftermath Daniel T. Haydon, Rowland R. Kao and R. Paul Kitching The 2001 epidemic of foot-and-mouth disease in the United Kingdom triggered a livestock culling campaign that involved the slaughter of more than 6.5 million animals. Three years later, management of the epidemic remains controversial. Some believe that untried control methods based on unvalidated models replaced well-established policy, motivating an unnecessary slaughter. Others hold that rigorous quantitative approaches provided the basis for new incisive policies that significantly curtailed the epidemic. Now, new and more flexible control policies have been adopted throughout Europe. For these policies to receive the full confidence of scientists, veterinarians and the general public, it is necessary that we improve both our understanding of where, how and why control measures initially failed in 2001 and how new policies should be implemented. Foot-and-mouth disease (FMD) is a highly infectious viral disease of cloven-hoofed animals. Its main epidemiological features are described in BOX 1. The Office Internationale des Epizooties (OIE) recognizes countries (or regulated regions within countries) to be in one of three disease states: FMD free without vaccination; FMD free with vaccination; and FMD present with or without vaccination. Countries move through these stages, typically accessing wider and more profitable export markets as the level of disease control is progressively improved. Countries with endemic FMD generally start with extensive vaccination programmes, which, in combination with movement regulations and other sanitary measures, reduce the incidence of new infections, ultimately to zero, after which time the use of vaccination can be stopped altogether. Such programmes are costly, can take many years to succeed and often experience substantial setbacks1. Consequently, the development of alternative regulatory practices that recognize regional disease-free status as not necessary for safe trade of some livestock commodities should be strongly encouraged2. Over the past five decades most European countries have used vaccination programmes, but in 1992 the widespread use of vaccination in the European Union (EU) was banned for reasons we describe below. Since then, with the exception of occasional outbreaks, the EU has moved to a disease-free unvaccinated state. In the United Kingdom vaccination has never been used, and in a fully susceptible host population control has always been undertaken using ‘traditional methods’3. Historical perspectives on control Traditional control of FMD involves the imposition of regional movement bans, the disinfection of infected properties and rapid slaughter of all animals on premises that are identified as being infected (IPs), as having had ‘dangerous contact’ with an IP (DCs) or as being particularly infectious if, and at risk of being, infected. For decades most FMD outbreaks have been well controlled by traditional methods. For example, the Northumberland Report4 refers to 180 primary outbreaks of FMD in the United Kingdom between 1954 and 1967, all of which were contained using traditional methods: 169 resulted in no more than 20 further cases (FIG. 1a), and only four epidemics generated more than 50 cases — one of these is the 1967 outbreak that resulted in more than 2,000 cases. The 2001 UK outbreak was different to previous outbreaks in many respects, foremost of which was that in the early stages of the epidemic the authorities were unable to apply traditional control methods to a high standard in all areas5,6. For the first time mathematically based computer models were used in the management of an outbreak. In contrast to empirically derived ‘tried and tested’ FMD control policies that have been in use over the past several decades, the results of this modelling indicated that the epidemic would be controlled more effectively if widespread culling of apparently uninfected herds, and, in particular, culling based purely on geographical proximity was adopted. These observations beg two questions. First, why did the models produce such a contrasting FMD control VOLUME 2 | AUGUST 2004 | 6 7 5 PERSPECTIVES policy to that apparently endorsed by the historical record? Second, what would have happened in 2001 if traditional methods had been efficiently applied from the outset? Surprisingly, these are questions that have received little attention in the literature. A good understanding of where, how and why traditional methods failed is vital if the correct lessons are to be learned from this epidemic. It is particularly important that these issues are subject to scrutiny because the new UK Department for Environment, Food and Rural Affairs (DEFRA) contingency plan for FMD outbreaks is a particularly flexible one that will require the authorities to choose from a range of control measures that include culling of both IP and DC animals, pre-emptive FIREBREAK CULLING, and emergency 7 VACCINATION TO KILL and VACCINATION TO LIVE . A summary comparison of the outbreaks of 1967 and 2001 is thought-provoking. In 1967, estimates of the number of IPs that were infected directly from primary cases vary from 38 to 59 (REFS 8,9), and all were contained in a relatively small area. In 2001, disease entered the United Kingdom in early February and by the time disease was confirmed on 20 February, at least 30 premises10,11, and possibly as many as 79 (REF. 12), were infected. Unlike in 1967, the result was widespread outbreaks from Dumfries and Galloway in the north, to Devon in the south, as well as overseas to Northern Ireland, France and the Netherlands. Late on the evening of 23 February a national movement ban was imposed. Following this, most spread was ‘local’, that is, limited to within 3 km of an IP10,13. Both the 1967 and 2001 epidemics were characterized by lengthy final phases. In 1967 the epidemic lasted 212 days and caused outbreaks on 2,364 different premises4. In 2001 the epidemic lasted 214 days and resulted in the identification of infection and culling of herds on 2,026 premises6. Glossary FIREBREAK CULLING The culling of animals for the purpose of preventing spread of infection beyond an area, even though the animals are not believed to have been exposed to infection. VACCINATION TO KILL Or suppressive vaccination. A vaccination policy adopted within the protection zone that anticipates that vaccinated individuals will be destroyed as soon as circumstances allow. VACCINATION TO LIVE Or protective vaccination. A vaccination policy that anticipates that vaccinated individuals will not be prematurely slaughtered, and will enter the food chain as normal. 676 | AUGUST 2004 | VOLUME 2 Box 1 | Foot-and-mouth disease — the basics Foot-and-mouth disease (FMD) is a disease of cloven-hoofed animals such as cattle, pigs, sheep and goats. The pathology of FMD includes fever, vesicles in the mouth, feet and udders, loss of milk production in adult animals and death in young animals. Infected cattle, sheep and goats can become carriers of FMD that are persistently infected (and occasionally infectious) for up to 3.5 years depending on the host species37. FMD virus is an RNA virus of the family Picornaviridae (genus Aphthoviridae). It has seven distinct serotypes, between which there is no immunological cross-reactivity. The FMD virus genome contains 8,400 nucleotides and 12 genes, four of which encode capsid proteins. FMD virus genomes are diverse: capsid genes of the same serotype can differ by more than 30% of nucleotides and distant subtypes within the same serotype may only elicit weak cross-reactivity, so the choice of (inactivated) vaccine strains must be carefully matched to outbreak strains against which protection is sought. The virus can evolve rapidly (for example, 1.5% of capsid gene nucleotides can change per year, or at an estimated fixation rate of one nucleotide in these genes over the course of an individual infection42), but the Pan-Asia strain has shown remarkable genetic stability over several years. The virus is released in all secretions and excretions of an infected animal, especially in their breath and secretions that are associated with ruptured vesicles. Transmission of FMD virus can take place mechanically by people who have handled infected animals, on straw or hay that is contaminated by infected animals, on farm vehicles or milk tankers carrying infected milk, or even on the surgical equipment of veterinary surgeons. FMD virus can also spread as an aerosol — the 1981 outbreak on the Isle of Wight, UK, was caused by virus from an outbreak in pigs in Brittany, a distance of more than 250 km43; however, over land, spread of the virus rarely exceeds 10 km44. One of the most intriguing aspects of the epidemiology of FMD is the seemingly high variability in the transmissibility of the virus. It is thought to have one of the lowest infectious doses of any virus45 has enormous potential for infectiousness within herds46 and, under the right conditions, a remarkable capacity to spread by aerosol over considerable distances8,43. Oddly however, under other conditions, FMD virus seems to be less infectious — for example, there is some evidence that FMD virus cannot be maintained over long time periods in sheep populations47 and when the Pan-Asia virus spread to the Netherlands, studies showed that it failed to spread between calves that were in direct contact with each other48. More than half (98) of the 180 primary cases reported in the United Kingdom between 1954 and 1967 failed to infect any other premises and in the 2001 epidemic the first case — a large pig farm left infectious for at least 2 weeks during meteorological conditions favourable to transmission28 — is thought only to have infected 1–10 neighbouring farms before it was finally culled27. Despite these similarities, some important differences must be recognized when comparing the two epidemics. In 1967 slaughter was mostly confined to animals from IPs, whereas in 2001 animals were culled on a further 8,131 premises that were close to, or in some other way associated with, IPs 6. In 1967, approximately 442,000 animals were slaughtered to control the epidemic, whereas in 2001 at least 4 million animals were slaughtered for the purposes of disease control, with at least a further 2.5 million animals destroyed in ‘welfare culls’6. Nationally, prior to the 2001 epidemic, total numbers of the two most important host species for the FMD virus (cattle and pigs) were 8% less than 1967 figures. The average dairy herd size had doubled since 1967 (REF. 5), but the effects of fewer larger herds on disease control are unclear (although obviously the number of individuals culled per IP must increase). In addition, sheep numbers had increased by 46% and the physical movement of infected sheep was responsible for much of the early dissemination of infection in 2001 (REF. 14) — sheep were present on 80% of all IPs, including 15% that were solely sheep farms. By contrast, the 1967 epidemic was mostly restricted to cattle. Diagnosis in sheep is much more difficult, which probably led to delays in the identification of IPs in 2001. However, sheep are less infectious than both pigs and cattle15. The modern livestock industry involves the movement of many more animals than in 1967, but the epidemiological significance of this diminishes after the imposition of movement bans. The effects of these changes on the efficacy of traditional measures in controlling FMD outbreaks remain largely unexplored. The extent to which pathogens are infectious prior to the onset of discernable pathology is obviously an important determinant of the extent to which epidemics can be efficiently controlled16. The FMD virus is genetically diverse and it is plausible that differences in both the transmissibility and the route of transmission might exist between strains, which could alter the effectiveness of www.nature.com/reviews/micro PERSPECTIVES a Sizes of FMDV outbreak b Time to slaughter for 1967 and 2001 epidemics 70 50 Number of secondary outbreaks 0 1–5 6–10 11–20 21–50 >50 50 (67) Percentage of IPs Number of primary outbreaks 40 2001 Reporting to slaughter 2001 Confirmation to slaughter 1967 Confirmation to slaughter 60 30 (243) 20 (61) 40 30 20 10 10 (2,364) 0 0 54 55 56 57 58 59 60 61 62 63 64 65 66 67 19 19 19 19 19 19 19 19 19 19 19 19 19 19 Year 0 1 2 3 4 5 6 7 8 9 10 11 Interval (Days) Figure 1 | Past performance and implementation of traditional methods. a | Primary outbreaks of FMD from 1954 to 1967, together with the number of associated secondary outbreaks4. Primary outbreaks are those that cannot be linked with any known source in Great Britain and are therefore attributed to FMD introduction from abroad. Secondary outbreaks are all those that arose by the spread of infection from primary outbreaks. Numbers in brackets refer to the actual number of outbreaks for those epidemics with more than 50 secondary cases. b | Comparison of the time between reporting or confirmation of FMD and slaughter of animals, for the epidemics in 1967 and 2001. Time intervals refer to the difference between the dates of reporting/confirmation and slaughter from 25 October onward for 1967 (REF. 4) and IPs with confirmation dates on or after 24 February for 2001. This figure was constructed using the most recent DEFRA data. IP, infected premises. Although successful control can be considered to be the prevention of endemic disease, the aims of a successful control strategy may have changed since traditional methods were last tested. Control strategies might seek to minimize various quantities, such as total animal loss, duration of the epidemic (which is currently the main objective in England and Wales)7, regional spread, financial loss (to several economic sectors) or animal suffering. Moreover, a small outbreak that is under control, and therefore in decline, is likely to be viewed as acceptable, but when the number of extant IPs is high, a substantial and potentially unacceptable number of new cases can still arise from an epidemic that is — technically — considered to be under control and might therefore necessitate further control measures18. Historically, traditional methods that have been viewed as successful because FMD has not become endemic in the UK might now be rejected on the grounds that they might be unable to contain FMD outbreaks under climatic conditions that are favourable to viral transmission and in areas of high livestock density. However, controversy persists because assembling evidence that alternative methods of control might work any better is not straightforward. The models — strengths, weaknesses a traditional control policy. However, experimental evidence for increased transmissibility of the Pan-Asia FMD virus strain that was responsible for the 2001 outbreak is statistically weak17. What we do know is that, for some reason, there was little aerosol spread during the 2001 outbreak and this should have made the outbreak easier, and not more difficult, to contain. Between 1967 and 2001, the capacity of the State Veterinary Services (SVS) in the United Kingdom had been greatly reduced. The number of SVS field staff was reduced from about 600 in 1967, to 220 in 2001 (REF. 6), and by 2001 few investigators had any practical experience of dealing with FMD. The scale of the outbreak prior to the imposition of movement controls stretched the SVS beyond their capacity to implement a functional traditional response. Between implementation of a national movement ban and adoption of a contiguous premises (CP) cull (in which animals on neighbouring premises to an IP were culled), traditional control methods were implemented to a standard far below that of the 1967 outbreak. Fewer than 10% of IPs were subject to culling on the day disease was reported, and only 35% were subject to culling by the following day (FIG. 1b). Although the number of reported IPs was increasing NATURE REVIEWS | MICROBIOLOGY exponentially, only 0.8 DCs were identified per IP5. This response was inadequate — the success of traditional methods depends on having the necessary resources to identify and cull IPs and DCs as early as possible. Controlling transmission Traditional control measures, directed at culling animals from IPs and DCs within 24 hours of reporting disease, were attempted up to 23 March, after which additional measures were introduced that included: slaughter on suspicion of infection; culling of pigs, sheep and goats on premises within 3 km of an IP in both Dumfries and Galloway and in Cumbria; and culling all premises contiguous to an IP within 48 hours. This last measure became known as the ‘24/48’ IP/CP cull policy and would prove highly controversial. There are instructive regional variations in the extent to which this policy was implemented; it seemed to be somewhat discretionary in Scotland, and may not have been “more than 50% implemented” elsewhere6. Indeed, although the CP cull is in principle easy to define, what is truly ‘contiguous’ is subject to interpretation, and the most appropriate definition is contingent on the assumed mode of disease transmission. There is one other difference between the management of the control strategy in 2001 to that of previous outbreaks. Soon after the discovery of the first case of FMD in 2001, members of the ‘FMD Science Group’ oversaw the construction and analysis of three independently developed epidemiological models of FMD spread. These models, which were based on computer simulation and mathematical techniques, were fitted to data as they were collated over the course of the epidemic and used to predict the future course of the epidemic under several control scenarios13,19–21. Although some very good quantitative epidemiologists were present in the United Kingdom in 1967, there is no record of any of them advising the FMD control policy at that time. The new and important role for quantitative modelling in real-time disease-control management reflects technological developments (such as powerful computers and spatial data), the maturing of quantitative epidemiology as an academic discipline and unusually direct communication between leading epidemiologists and senior government scientific advisors6. More importantly, it reflects a growing awareness of the need for rigorous data analysis, which was highlighted by the experience with BSE in the United Kingdom22. VOLUME 2 | AUGUST 2004 | 6 7 7 PERSPECTIVES The models are compared in detail elsewhere23. As they adopted different approaches yet still obtained similar important results24, it has been argued that the conclusions derived from them are likely to be robust. However, this confidence should not be exaggerated because all the models share certain fundamental similarities. One is that they assumed that the location of the farming premises as recorded in the agricultural census of 2000 was an appropriate surrogate for the location of livestock. Discrepancies between the location of livestock and the location according to the census were well known, and would limit the spatial resolution at which these models could determine local culling strategies. For example, the value of quantitative comparisons amongst a 3 km, 2 km, 1.5 km or CP cull would have been unclear21. Another similarity is that they were all parameterized using the same epidemiological data (provided by DEFRA), and it was assumed that these data were sufficiently accurate to allow detailed, predictive mathematical modelling at a level adequate to advise policy. Although models are valuable because they allow the objective exploration of data, all models must inevitably make assumptions and it is part of the modelling process to explore, question and review the consequences of these assumptions in an attempt to improve understanding of model behaviour and acquire greater and more widespread confidence in their predictions. We believe there are a number of points arising from the use of the outbreak data that require further examination in the published literature. First, contact-tracing data indicated that premises were infectious as early as 3.5 days after the estimated date of infection, with a constant probability of transmission until all the animals were slaughtered13,21. Unless transmission to an IP has occurred by animal movement, IPs would not always be expected to be infectious so quickly, and infectiousness might be expected to increase over time as the number of infected animals in the herd increases. The high estimated levels of infectiousness soon after the date of infection could be due to consistent error in identification of the source IP or in estimation of the date of contact with the infection. The date of contact is estimated by the date of the earliest known contact with an IP or by the age of lesions; however, in pigs and cattle older lesions have an error estimate of ± 3 days25. Although other factors, such as increased biosecurity on uninfected farms close to IPs might reduce the effects of rising infectivity over time, the models could be sensitive to changes in the infectiousness profile, and overestimation of the 678 | AUGUST 2004 | VOLUME 2 early infectiousness of IPs would lead to models exaggerating the importance of CP culling. The sensitivity of the models to this assumption remains unclear. Second, the relationship between the probability of transmission and the distance to an IP (known as the ‘transmission kernel’) is based directly on the contact-tracing data13. Although the data represents the best estimate of ‘who infected whom’, underlying biases in these estimates are mostly unexplored in the literature. Simulations of the epidemic in Cumbria overestimate the number of IPs close to locations at which the epidemic originated26. This might have been the result of excessive wave-like progression of the simulated epidemics, caused by an overestimation of the importance of local spread, and could lead to an exaggerated estimate of the value of CP culling. Third, it is assumed that identification of the disease on farms was accurate. Detailed analysis of the proportion of IPs that were confirmed as infected by laboratory tests is yet to be published, but given the difficulty of diagnosing disease in sheep, it is anticipated to be substantially less than 100% — for example, in 1967, fewer than 20% of doubtful cases were subsequently found to be infected4. Subsequent analysis12 has revealed that the role of animal movement in the early spread of infection might have been underestimated, leading to a potential overestimation of the number of premises that were infected after the movement ban was imposed. Both sources of error could cause the models to overestimate the control effort that was required13. Fourth, although it is well known that after movement restrictions were imposed in late February the transmission kernel changed to reflect much higher levels of local transmission21, a constant transmission kernel was assumed in all models thereafter. The transmission kernel only describes the effect of distance on infectious contact without distinguishing amongst airborne, animal contact or mechanical transmission. Early on in the course of the epidemic, aerosol transmission may have been important27, but environmental conditions28 and the lack of transmission to pigs reduced its later impact10. Anecdotally, the proportion of infectious contacts that were assigned to animal movements or human activity increased over the time course of the epidemic29. Transmission is assumed to be independent of the control policy but changing the control policy might affect logistics, farmer compliance or the implementation of biosecurity. Ferguson et al.20 have suggested that significant increases in the transmission rate might have occurred towards the end of the epidemic. Although difficult to prove, the extensive movements of people, animals and vehicles owing to the intensive slaughter policy could have exacerbated transmission. Finally, the models assume that the linear distance between farms was the main determinant of transmission risk. If two farms have the same composition and are equidistant from an IP, then the models assume that they are equally likely to become infected, and so a purely spatially motivated policy like the CP cull is favoured. However, if one is more likely to become infected than the other (for example, if two farms are connected by a wellused road), then identifying the high-risk property becomes more worthwhile. This is the question that lies at the core of the controversy over the control policy — what is the effectiveness of a DC cull compared with a CP cull? Although the models predict that, as implemented, the cull was superior to the other options considered, a comparison with a well-managed traditional policy is yet to be published13,20. More recent analyses indicate that even very precise DC culling would only have been valuable if the time between disease diagnosis and slaughter could have been reduced26, and that the overall number of premises subject to culling may be fairly insensitive to overculling at the local level18. This indicates that the superior performance of the CP cull in reducing the epidemic duration might be more important than any apparent over-culling. However, a better understanding of the risk factors that are associated with transmission of infection is critical for a comprehensive evaluation of the benefits of DC culling30. The main factor responsible for the end of the epidemic probably varied regionally, but there is evidence that factors other than the change in control policy could have been the most important (BOX 2). Whatever future analyses may tell us, unprecedented numbers of animals were slaughtered in a new and untested control procedure, largely formulated and justified with the use of necessarily hastily developed computer models. Given uncertainties in the data and the reliance of these models on assumptions that are necessarily crude and also difficult to verify, it is difficult to make the argument that mathematical models showed that implementation of widespread and intensive culling was the only tenable option. Models did show clearly, and at a relatively early stage, that a traditional policy, as previously implemented, was not sufficient to prevent the development of a very large epidemic. However, the main arguments in favour of a CP cull are simpler decision-making and ease www.nature.com/reviews/micro PERSPECTIVES Box 2 | Reduction of disease transmission IP Incidence 04 /0 5 27 /0 4 20 /0 4 13 /0 4 06 /0 4 30 /0 3 23 /0 3 16 /0 3 09 /0 3 02 /0 3 Date b 10 9 8 7 6 5 4 3 2 1 27 /0 4 20 /0 4 13 /0 4 06 /0 4 0 30 /0 3 Reduction in the infectious period 0 23 /0 3 Movement restrictions and biosecurity both contribute to a reduction in the rate at which disease is transmitted. 5 16 /0 3 Reduction in the transmission rate 10 09 /0 3 In the case of the 2001 epidemic, fortuitous weather conditions might have limited aerosol transmission28. 15 02 /0 3 Environmental factors 20 23 /0 2 If the pool of susceptible premises becomes sufficiently small the disease will die out. As the range of FMD transmission is limited, the reduction in the number of susceptible premises in the vicinity of IPs may also cause the disease to die out locally. Any culling of premises that are not infected (whether as part of a dangerous contact (DC), contiguous premises (CP) or other cull) will contribute to the depletion of the susceptible population with CP culling likely to contribute most to local depletion. Movement restrictions decrease the effective range of FMD transmission21, making local depletion effects more important. 30 25 IP Incidence Depletion of the susceptible population a 23 /0 2 In the 2001 epidemic several factors might have contributed to reducing transmission. These can be categorized by the nature of their effects, with some factors having multiple effects. Date All culling that removes infected premises (including IP, DC and CP culling strategies) contributes to a reduction in the infectious period. The rationale behind the CP cull is that the increased probability of culling uninfected premises is compensated for by a reduction in the infectious period of those CPs that are infected but have not yet been identified. When a combination of these factors results in a reduction of the average number of new infections caused by an IP to below one, the epidemic is classed as being under control49, although there might be many more infection events before the epidemic is over. What caused the 2001 epidemic to end? This is likely to have varied between regions. Reducing the period of time before an animal is slaughtered and increasing detection rates no doubt contributed to the decline of the epidemic, and the revised policy measures were designed to facilitate this. However, reconstructions of the epidemic indicate that the rate at which new infections were arising peaked between 19 March and 21 March11, and the number of reported cases peaked on 26 March — before these new policy measures were implemented13,23. Therefore, the switch to more stringent control procedures could not have been responsible for this initial reduction. Population depletion may have had a greater effect. In Cumbria (figure part a) the epidemic (shown in red) is compared to an average of 100 simulated epidemics using the algorithm of Kao26 (shown in green) and with modified simulations with the same parameters but double the number of premises and double the area (shown in blue). This analysis addresses what could have happened if Cumbria covered an area twice as large. The divergence of the two curves in late March suggests that the main cause of the downturn was geographical isolation — the epidemic simply ran out of room. Thus, in Cumbria, although the revised control policies are likely to have contributed to the decline of the epidemic18,26, the epidemic was arguably never under control, except in the sense that movement restrictions and biosecurity prevented the transmission of disease to new areas while the epidemic burned itself out. In Devon (figure part b), the epidemic (shown in red) is compared to the average of 100 simulations recreating the actual culling policy in Devon (shown in green) and a policy in which culling is restricted to animals on IPs only (shown in blue). The incidence in the two simulations declines at similar points. This corroborates a previous result50, which indicated that IP culling alone might have been sufficient to bring the disease under control. Although requiring more rigorous investigation, this was likely to have been true in other affected regions in the UK where infection was less widespread. of management, together with the benefit that, in a time of great chaos and uncertainty, a clearly defined policy with simple goals can be of both logistical and political value. Looking to the future The direct and indirect economic tolls of the 2001 epidemic are estimated to have been at least UK £3 billion and UK £5 billion, NATURE REVIEWS | MICROBIOLOGY respectively31,32. This, together with widespread public disquiet at the visible slaughter of at least 6.5 million animals, has prompted a major revision of outbreak contingency planning. Many excellent recommendations have been made by commissioned reports5,6,33 and have been incorporated into future contingency plans7. An obvious recommendation is the imposition of an automatic nationwide movement ban on all livestock immediately after confirmation of the first case. In 2001, such action could have halved the size of the epidemic11. More radical is the recommendation that emergency vaccination “should now be considered as part of the control strategy from the start of any outbreak”5. This recommendation arises partly from the positive outcomes of vaccination campaigns VOLUME 2 | AUGUST 2004 | 6 7 9 PERSPECTIVES carried out in Uruguay34 and experience in the Netherlands35 in 2001. Culling of animals on IPs will continue to remain part of any control programme, and therefore any outbreak will always involve slaughter regardless of whether emergency vaccination is implemented. Nevertheless, the recommendation to vaccinate is welcome provided several important difficulties are overcome. Vaccinated animals will always require time to acquire protective immunity, although this time can be substantially reduced by the use of high-potency vaccines36. Furthermore, vaccination might not always prevent infection or the establishment of a long-term asymptomatic but potentially infectious carrier state in cattle and sheep37 (although recent results seem to also confirm the effectiveness of high-potency vaccines in inhibiting the carrier state38). For this reason, OIE regulations had required a delay of 1–2 years before countries that had an FMD outbreak, and which had used emergency vaccination, could reapply for full disease-free status (in contrast to just 3 months if culling alone was used). This delay has recently been reduced to 6 months provided adequate numbers of vaccinated animals are subject to a test for antibodies to viral non-structural proteins (NSPs) that can, in principle, distinguish between animals that have been vaccinated and those that are, or have been, infected. However, there are some problems with this approach— for example, it is doubtful that putative carrier animals always produce detectable quantities of antibody to NSPs39 and the development of more sensitive tests will require the use of more highly purified and expensive vaccines. Policy on emergency ‘vaccination-to-live’ is now included in the EU directive 2003/85/EC (Article 61)40, which also requires member states to “make all arrangements necessary for emergency vaccination” on confirmation of the first identified case of disease (Article 14.3). Article 64.1 of this directive prohibits the movement of vaccinated animals between member states and, in all likelihood, the movement of such animals would also be restricted nationally, anticipating the difficulty that authorities would have in identifying virus carriers using existing NSP tests. In the UK, a further consequence has been the extension of the legal authority to cull, which now includes “any animal the Secretary of State thinks should be slaughtered with a view to preventing the spread of foot-and-mouth disease”, as outlined in the Animal Health Act of 2002. The UK authorities were poorly prepared for the 2001 outbreak, and the consequent renewal of investment in attempts to develop 680 | AUGUST 2004 | VOLUME 2 better vaccines and diagnostic methods, and to improve contingency planning is both welcome and long overdue. The addition of epidemiological models to the range of techniques used in the formulation of FMD control policy is a significant advance. However, we must learn how information from quantitative models should be incorporated into policy formulation in a balanced way, mindful of its persuasive but often illusory level of numerical precision. It is essential that models are developed and used in a manner that allows both their strengths and inevitable short-comings to be recognized and widely understood33,41. The implications of limited logistical and human resources need to be integrated into modelling of control scenarios and we need to understand how such limitations influence the choice of policy options. The aims of a successful control policy need to be defined more precisely and the ability to coordinate policy centrally, without losing capability to tailor control tactics locally needs to be developed. We need to understand more about the precise mechanisms that allow the local spread of disease. We need to develop rigorous protocols for exploring phenotypic variability which might characterize different viral strains, and not simply track, but react to, the locations of strains worldwide. In addition, although traditional methods have worked for most occasions when infection has been introduced into the United Kingdom, we need to learn why and when these measures can fail. The current DEFRA FMD contingency plan recognizes the need for a flexible set of control procedures, but the timing of the decisions regarding control options is crucial, and criteria are required with which the seriousness of outbreaks can be evaluated early so that an appropriately measured response is selected. On the basis of analyses of published data from the 2001 epidemic, we cannot conclude that traditional methods of control no longer work, only that, as implemented in 2001, they did not work to an acceptable standard. What is now required is a marriage of the value of the expert advice so staunchly defended by the veterinary practice, with the benefits of modern surveillance, diagnostic and data management technologies and the analytical capabilities of theoretical modelling at the strategic level. This will require drive, focus and coordinated cross-disciplinary communication, and patience, good listeners, and open minds. Properly resourced, FMD contingency planning should provide a model for twenty-first century disease control. Daniel T. Haydon is at the Division of Environmental and Evolutionary Biology, University of Glasgow, Glasgow G12 8QQ, UK. Rowland R. Kao is at the Department of Zoology, University of Oxford, South Parks Rd, Oxford OX1 3PS, UK. R. Paul Kitching is at the National Centre for Foreign Animal Diseases. 1015 Arlington Street, Winnipeg, Manitoba R3E 3M4, Canada. Correspondence to D.T.H. e-mail: [email protected] All authors contributed equally to this work. doi:10.1038/nrmicro960 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. Correa Melo, E., Saraiva, V. & Astudillo, V. Review of the status of foot and mouth disease in countries of South America and approaches to control and eradication. Rev. Sci. Tech. 21, 429–436 (2002). Thomson, G. R. et al. Shifting paradigms in international animal health standards: the need for comprehensive standards to enable commodity based trade. [online] <http://www.eldis.org/fulltext/shiftingparadigms.pdf> (2004). Woods, A. To vaccinate or vacillate? The British response to foot and mouth disease, 1920–2001. Hist. Res. (in the press). Northumberland. Report of the Committee of Inquiry on Foot-and-Mouth Disease. (Her Majesty’s Stationery Office, London, 1969). The Royal Society. Inquiry into Infectious Diseases in Livestock. (The Stationery Office, London, 2002) [online], <http://www.royalsoc.ac.uk/inquiry/index.html> (2002). Anderson, I. Foot and Mouth Disease 2001: Lessons to be Learned Inquiry [online], <http://www.defra.gov.uk/ corporate/inquiries/lessons/index.htm> (2001). DEFRA. Foot and Mouth Disease — contingency plan. [online] <http://www.defra.gov.uk/footandmouth/ contingency/index.htm> (2004). Tinline, R. Lee wave hypothesis for the initial pattern of spread during the 1967–68 foot and mouth epizootic. Nature 227, 860–862 (1970). Haydon, D. T., Woolhouse, M. E. J. & Kitching, R. P. An analysis of foot-and-mouth-disease epidemics in the UK. IMA J. Math. Appl. Med. Biol. 14, 1–9 (1997). Gibbens, J. C. et al. Descriptive epidemiology of the 2001 foot-and-mouth disease epidemic in Great Britain: the first five months. Vet. Rec. 149, 729–743 (2001). Haydon, D. T. et al. The construction and analysis of epidemic trees with reference to the 2001 UK foot-andmouth outbreak. Proc. R Soc. Lond. B Biol. Sci. 270, 121–127 (2003). Mansley, L. M., Dunlop, P. J., Whiteside, S. M. & Smith, R. G. Early dissemination of foot-and-mouth disease virus through sheep marketing in February 2001. Vet. Rec. 153, 43–50 (2003). Keeling, M. J. et al. Dynamics of the 2001 UK foot and mouth epidemic: stochastic dispersal in a heterogeneous landscape. Science 294, 813–817 (2001). Gibbens, J. C. & Wilesmith, J. W. Temporal and geographical distribution of cases of foot-and-mouth disease during the early weeks of the 2001 epidemic in Great Britain. Vet. Rec. 151, 407–412 (2002). Donaldson, A. I., Alexandersen, S., Sorensen, J. H. & Mikkelsen, T. Relative risks of the uncontrollable (airborne) spread of FMD by different species. Vet. Rec. 148, 602–604 (2001). Fraser, C., Riley, S., Anderson, R. M. & Ferguson, N. M. Factors that make an infectious disease outbreak controllable. Proc. Natl Acad. Sci. USA 101, 6146–6151 (2004). Alexandersen, S. & Donaldson, A. I. Further studies to quantify the dose of natural aerosols of foot-and-mouth disease virus for pigs. Epidemiol. Infect. 128, 313–323 (2002). Matthews, L. et al. Neighbourhood control policies and the spread of infectious diseases. Proc. R. Soc. Lond. B Biol. Sci. 270, 1659–1666 (2003). Morris, R. S., Wilesmith, J. W., Stern, M. W., Sanson, R. L. & Stevenson, M. A. Predictive spatial modelling of alternative control strategies for the foot-and-mouth disease epidemic in Great Britain, 2001. Vet. Rec. 149, 137–144 (2001). Ferguson, N. M., Donnelly, C. A. & Anderson, R. M. Transmission intensity and impact of control policies on the foot and mouth epidemic in Great Britain. Nature 413, 542–548 (2001). www.nature.com/reviews/micro PERSPECTIVES 21. Ferguson, N. M., Donnelly, C. A. & Anderson, R. M. The foot-and-mouth epidemic in Great Britain: pattern of spread and impact of interventions. Science 292, 1155–1160 (2001). 22. Phillips, N., Bridgeman, J. & Ferguson–Smith, M. Report of the Inquiry into BSE and Variant CJD in the United Kingdom. (Her Majesty’s Stationery Office, London, 1999). 23. Kao, R. R. The role of mathematical modelling in the control of the 2001 FMD epidemic in the UK. Trends Microbiol. 10, 279–286 (2002). 24. Woolhouse, M. E. Foot-and-mouth disease in the UK: what should we do next time? J. Appl. Microbiol. 94, S126–S130 (2003). 25. Alexandersen, S., Kitching, R. P., Mansley, L. M. & Donaldson, A. I. Clinical and laboratory investigations of five outbreaks of foot-and-mouth disease during the 2001 epidemic in the United Kingdom. Vet. Rec. 152, 489–496 (2003). 26. Kao, R. R. The impact of local heterogeneity on alternative control strategies for foot-and-mouth disease. Proc. R. Soc. Lond. B Biol. Sci. 270, 2557–2564 (2003). 27. Gloster, J. et al. Airborne transmission of foot-and-mouth disease virus from Burnside Farm, Heddon-on-the-Wall, Northumberland, during the 2001 epidemic in the United Kingdom. Vet. Rec. 152, 525–533 (2003). 28. Mikkelsen, T. et al. Investigation of airborne foot-andmouth disease virus transmission during low-wind conditions in the early phase of the UK 2001 epidemic. Atmos. Chem. Phys. Disc. 3, 677–703 (2003). 29. Wingfield, A. S., Middlemiss, C. H. & Eppink, L. FMD control strategies. Vet. Rec. 152, 479–480 (2003). 30. Taylor, N. M., Honhold, N., Paterson, A. D. & Mansley, L. M. Risk of foot-and-mouth disease associated with proximity in space and time to infected premises and the implications for control policy during the 2001 epidemic in Cumbria. Vet. Rec. 154, 617–626 (2004). 31. National Audit Office. Report by the Comptroller and Auditor General: The 2001 Outbreak of Foot and Mouth Disease. (The Stationery Office, London, 2002) [online], <http://www.nao.org.uk/publications/nao_reports/01-02/ 0102939part1.pdf>, <http://www.nao.org.uk/publications/ nao_reports/01-02/0102939part2.pdf> (2002). NATURE REVIEWS | MICROBIOLOGY 32. Thompson, D. et al. Economic costs of the foot and mouth disease outbreak in the United Kingdom in 2001. Rev. Sci. Tech. 21, 675–687 (2002). 33. Royal Society (Edinburgh). Inquiry Into Foot and Mouth Disease in Scotland. (Royal Society of Edinburgh, Edinburgh, 2002). 34. Sutmoller, P. & Olascoaga, R. C. in Evidence for the Temporary Committee on Foot-and–Mouth Disease of European Parliament. Meeting 2nd Sept. (European Parliament 2002). 35. Bouma, A. et al. The foot-and-mouth disease epidemic in The Netherlands in 2001. Prev. Vet. Med. 57, 155–166 (2003). 36. Barnett, P. V. & Carabin, H. A review of emergency footand-mouth disease (FMD) vaccines. Vaccine 20, 1505–1514 (2002). 37. Donaldson, A. I. & Kitching, R. P. Transmission of footand-mouth disease by vaccinated cattle following natural challenge. Res. Vet. Sci. 46, 9–14 (1989). 38. Barnett, P. V. et al. Evidence that high potency foot-andmouth disease vaccine inhibits local virus replication and prevents the ‘carrier’ state in sheep. Vaccine 22, 1221–1232 (2004). 39. Mackay, D. K., Forsyth, M. A., Davies, P. R. & Salt, J. S. Antibody to the nonstructural proteins of foot-and-mouth disease virus in vaccinated animals exposed to infection. Vet. Q. 20, S9–11 (1998). 40. The Council of the European Union. Council Directive 2003/85/EC. Official J. European Union L 306, 1–41 (2003). 41. Eddy, R. Vets asked valuable questions about foot-andmouth measures. Nature 412, 477 (2001). 42. Haydon, D. T., Samuel, A. R. & Knowles, N. J. The generation and persistence of genetic variation in foot-andmouth disease virus. Prev. Vet. Med. 51, 111–124 (2001). 43. Donaldson, A. I., Gloster, J., Harvey, L. D. & Deans, D. H. Use of prediction models to forecast and analyse airborne spread during the foot-and-mouth disease outbreaks in Brittany, Jersey and the Isle of Wight in 1981. Vet. Rec. 110, 53–57 (1982). 44. Donaldson, A. Foot-and-mouth disease: the principal features. Ir. Vet. J. 41, 325–327 (1987). 45. Alexandersen, S., Zhang, Z., Donaldson, A. I. & Garland, A. J. The pathogenesis and diagnosis of foot-and-mouth disease. J. Comp. Pathol. 129, 1–36 (2003). 46. Woolhouse, M. E. J., Haydon, D. T., Pearson, A. & Kitching, R. P. Failure of vaccination to prevent outbreaks of foot-and-mouth disease. Epidemiol. Infect. 116, 363–371 (1996). 47. Hughes, G. J. et al. Serial passage of foot-and-mouth disease virus in sheep reveals declining levels of viraemia over time. J. Gen. Virol. 83, 1907–1914 (2002). 48. Bouma, A., Dekker, A. & de Jong, M. C. No foot-andmouth disease virus transmission between individually housed calves. Vet. Microbiol. 98, 29–36 (2004). 49. Woolhouse, M. E. J. et al. Foot-and-mouth disease under control in the UK. Nature 411, 258–259 (2001). 50. Kao, R. R. Landscape fragmentation and foot-andmouth disease transmission. Vet. Rec. 148, 746–747 (2001). Acknowledgments We thank the anonymous referees for their helpful comments and many colleagues for advice that has greatly improved the various drafts of this manuscript. R.R.K. is funded by the Wellcome Trust. Competing interests statement The authors declare that they have no competing financial interests. Online links FURTHER INFORMATION DEFRA Summary report of the foot-and-mouth disease modelling workshop: http://www.defra.gov.uk/science/ Publications/FMD_modelling_Summary_Report.pdf Daniel T. Haydon’s laboratory: http://www.gla.ac.uk:443/ibls/staff/staff.php?who=PQdGSP Access to this links box is available online. VOLUME 2 | AUGUST 2004 | 6 8 1