Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
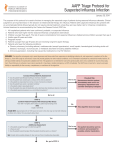
PRACTICE POINT The use of antiviral drugs for influenza: Guidance for practitioners, 2012/2013; Paediatric summary Upton D Allen; Canadian Paediatric Society Infectious Diseases and Immunization Committee Paediatr Child Health 2013;18(3):155-8 Posted: Mar 1 2013 Reaffirmed: Feb 1 2016 Abstract This practice point summarizes the use of antiviral drugs to manage influenza illness in children and youth for the 2012/2013 season. It excerpts a re cently published, full-length update of Canadian recommendations for clinicians on the use of antivi ral drugs for the prevention and treatment of in fluenza, with a focus on paediatric antiviral therapy. Detailed information on the selective use of chemo prophylaxis can be found in the source document, which also highlights the importance of secondary bacterial infections (Streptococcus pneumoniae, methicillin-sensitive Staphylococcus aureus and methicillin-resistant S aureus) in cases of severe in fluenza illness. Key Words: Antiviral therapy; Children; Influenza; Neuraminidase inhibitors Citation for the full-length source document: Aoki FY, Allen UD, Stiver HG, Evans GA. The use of antiviral drugs for influenza: Guidance for practitioners 2012-2013. Can J Infect Dis Med Microbiol 2012;23(4):e79-e92. Available at: www.ammi.ca/me dia/48038/14791_aoki_final.pdf.pdf. Antiviral use in children There are fewer data to guide the management of in fluenza illness in children generally, and especially in infants, than for adults. Background information on this illness in children, provided in the full-length guidance document, was based on data derived from paediatric populations.[1]-[5] More on the strengths and weakness es of current evidence relating to antiviral use can be found at: http://onlinelibrary.wiley.com/doi/ 10.1002/14651858.CD008965.pub3/abstract. Signifi cant issues include high influenza attack rates in school-aged children,[1]-[2] the atypical, non-specific na ture of influenza illness in young children,[3] and the high risk of adverse outcomes from influenza illness among children younger than five years of age.[5] Hos pitalizations occur more frequently among children younger than two years of age compared with older children, with the highest hospitalization rates being among infants younger than six months of age.[3] These statistics do not necessarily translate into deci sions to use antiviral therapy in patients younger than two years of age; children of any age with mild influen za illness do not usually require treatment. Three currently available antiviral agents are approved for use for children in Canada. Amantadine, for sea sonal influenza A, is not currently useful because of re sistance. Oseltamivir (Tamiflu, Hoffman-La Roche Ltd, Canada) and zanamivir (Relenza, GlaxoSmithKline Inc, United Kingdom) are used for influenza A and B. More recent studies on the neuraminidase inhibitors (NAIs) have been reported or are in progress, and ex perience with their use is increasing.[6]-[9] However, there is a notable paucity of current data from random ized trials in infants and young children. Two recent studies provided valuable safety data[10] and data on oseltamivir use in premature newborns.[11] However, oseltamivir use for 2012/2013 seasonal influenza in children younger than one year of age should be han dled on a case-by-case basis based on severity of ill ness. Oseltamivir is not approved for this indication in Canada, though it was temporarily approved for use in infants under one year on the basis of a favourable risk-to-benefit ratio during the 2009 H1N1 pandemic. INFECTIOUS DISEASES AND IMMUNIZATION COMMITTEE, CANADIAN PAEDIATRIC SOCIETY | 1 Published recommendations for oseltamivir dosing for babies younger than one year of age vary within a rea sonably narrow range.[12]-[14] Treatment recommendations Risk factors and drug doses are summarized in Table 1 and Table 2. A treatment algorithm is included as Figure 1. For explanation of levels of evidence, see the full guidance document. TABLE 1 At-risk groups and comorbid medical conditions that predispose to severe influenza illness • Asthma or other chronic pulmonary diseases, including bronchopulmonary dysplasia, cystic fibrosis, chronic bronchitis and emphysema • Cardiovascular disease (excluding isolated hypertension; including congenital and acquired heart disease, such as congestive heart failure and symptomatic coronary artery disease) • Malignancy • Chronic renal insufficiency • Chronic liver disease • Diabetes mellitus and other metabolic diseases • Hemoglobinopathies such as sickle cell disease • Immunosuppression or immunodeficiency due to disease (eg, HIV infection, especially if CD4 is <200×106/L), or iatrogenic, due to medication • Certain rheumatological diseases, such as rheumatoid arthritis, systemic lupus erythematosus, psoriatic arthritis, antiphospholipid syndrome, scleroderma, spondyloarthropathies, Sjogren’s syndrome, dermatomyositis, vasculitis, sarcoidosis and polyarteritis nodosa • Neurological disease and neurodevelopmental disorders that compromise handling of respiratory secretions (cognitive dysfunction, spinal cord injury, seizure disorders, neuromuscular disorders, cerebral palsy, metabolic disorders) • Children younger than five years of age* • Children or youth who reside in homes or other chronic care facilities • Pregnant women and women up to two weeks postpartum regardless of how the pregnancy ended • Individuals <18 years of age who are on chronic acetylsalicyclic acid therapy • Obesity with a BMI ≥40 kg/m2, OR a BMI ≥3 z-scores above the mean for age and gender • First Nations, Inuit and Métis children and youth Adapted from references 15 and 16. * Children who are two years through four years of age have a higher rate of complications compared with older children; however, the risk for these children is lower than the risk for children younger than two years of age. BMI: Body mass index General principles: • If the decision is made to start an antiviral drug, treatment should be initiated as soon as possible after onset of illness. The benefits of treatment are much greater with initiation at <12 h than at 48 h. (Strong recommendation, Grade B evidence) • Otherwise healthy patients of any age with relative ly mild, self-limited influenza are not likely to benefit from neuraminidase inhibitor (NAI) therapy initiated >48 h after illness onset. Clinical judgment should be used. (Option, Grade D evidence) However, an tiviral therapy should be initiated even if the interval between illness onset and administration of antiviral medication exceeds 48 h if: 2 | THE USE OF ANTIVIRAL DRUGS FOR INFLUENZA: GUIDANCE FOR PRACTITIONERS, 2012/2013; PAEDIATRIC SUMMARY – The illness is severe enough to require hospital ization; (Strong recommendation, Grade X evi dence) – The illness is progressive, severe or complicat ed, regardless of previous health status; (Strong recommendation, Grade X evidence) or – The individual belongs to a group, other than age, at high risk for severe disease. (Strong rec ommendation, Grade X evidence) • Parents of children for whom antiviral therapy is not recommended should be advised of symptoms and signs of worsening illness that might warrant re assessment. (Recommendation, Grade D evi dence) • Treatment duration should routinely be five days (Strong Recommendation, Grade A evidence), but may be continued longer than five days if clinically indicated. (Option, Grade D evidence) Intubated patients with influenza illness should receive os eltamivir through a nasogastric tube. (Recommen dation, Grade C evidence) • For patients unable to tolerate or receive oral os eltamivir, inhaled or intravenous zanamivir is a suit able option. However, children younger than seven years of age are unlikely to be able to use the deliv ery device for zanamivir effectively. (Option, Grade D evidence) • Zanamivir may be preferred to oseltamivir in the fol lowing situations: – Patients not responding to oseltamivir therapy (Recommendation, Grade C evidence); or – Patients with illness despite oseltamivir prophy laxis (Recommendation, Grade C evidence). • For severely ill patients, zanamivir administered in travenously is preferred to inhaled drug. (Recom mendation, Grade D evidence) • In ventilated patients, zanamivir should only be ad ministered intravenously. (Strong Recommenda tion, Grade X evidence) • If patients are not responding to oseltamivir thera py, their virus should be tested for oseltamivir resis tance and the possibility of co-infection with anoth er pathogen considered. (Option, Grade D evi dence) Treating infants, children and youth with mild or uncomplicated influenza illness (Figure 1): • For those with mild disease and no risk factors other than age: – Younger than one year of age: NAIs are current ly not approved for the routine treatment of sea sonal influenza illness. Given that infants younger than six months of age are not eligible for influenza vaccination, immunization of their household and other close contacts is important in protecting them against influenza, thereby po tentially leading to reduced need for antiviral therapy. Influenza immunization of the pregnant woman may also provide protection for her in fant during the first six months of life. (Option, Grade D evidence) – One to less than five years of age: Although children under five years of age are classified as ‘high risk’ (with those younger than two years of age having the highest risk), those who are otherwise healthy and have mild disease not re quiring hospitalization do not routinely require antiviral therapy. For these children, treatment is optional. (Option, Grade D evidence) – Five or more years of age: Antiviral therapy is not routinely recommended for children and youth who are otherwise healthy and have mild disease not requiring hospitalization. (Option, Grade D evidence) • For those with mild disease and risk factors other than age: – Younger than one year of age: NAIs are cur rently not approved for the routine treatment of seasonal influenza illness. – One or more years of age: For illness of ≤48 h duration, treat with oseltamivir or, if age-appro priate, inhaled zanamivir. (Recommendation, Grade B evidence) – One or more years of age: For illness of >48 h duration, treat with oseltamivir or, if age-appro priate, inhaled zanamivir may be considered on a case-by-case basis. (Option, Grade D evi dence) Note: Grade X evidence denotes situations where vali dating studies cannot be performed and there is a clear preponderance of benefit or harm. INFECTIOUS DISEASES AND IMMUNIZATION COMMITTEE, CANADIAN PAEDIATRIC SOCIETY | 3 Treating infants, children and youth with moderate, progressive, severe or complicated influenza ill ness with or without risk factors: • Consider hospitalization and admission to the in tensive care unit. (Recommendation, Grade C evi dence) • Start antivirals immediately. (Strong recommenda tion, Grade B evidence) Treat with oseltamivir or zanamivir in appropriate doses. (Table 2) • Oseltamivir or zanamivir should be started even when the window between symptom onset and ini tial administration of the antiviral is >48 h. (Recom mendation, Grade C evidence) • Treatment with zanamivir instead of oseltamivir should be considered for: – Patients not responding to oseltamivir therapy: (Recommendation, Grade C evidence) or – Patients with illness despite oseltamivir prophy laxis. (Recommendation, Grade C evidence) • Although oseltamivir was approved temporarily for use in infants younger than one year of age on the basis of a favourable risk-to-benefit ratio during the 2009 H1N1 pandemic, its use in this population for seasonal influenza should be handled on a caseby-case basis, based on severity of illness. (Option, Grade D evidence) 4 | THE USE OF ANTIVIRAL DRUGS FOR INFLUENZA: GUIDANCE FOR PRACTITIONERS, 2012/2013; PAEDIATRIC SUMMARY TABLE 2 Oseltamivir and zanamivir treatment of influenza in children and youth (<18 years of age) – October 2012 Medication Treatment (five days) Chemoprophylaxis (10 days) 75 mg twice daily 75 mg once daily Oseltamivir* Adults Children ≥12 months Body weight, kg Body weight, lbs ≤15 ≤33 30 mg twice daily 30 mg once daily >15 to 23 >33 to 51 45 mg twice daily 45 mg once daily >23 to 40 >51 to 88 60 mg twice daily 60 mg once daily >40 >88 75 mg twice daily 75 mg once daily Children 3 months to <12 months† 3 mg/kg/dose twice daily 3 mg/kg/dose once per day Children <3 months‡ 3 mg/kg/dose twice daily Not recommended unless situation judged critical due to limited data on use in this age group Zanamivir§ Adults 10 mg (two 5 mg inhalations) 10 mg (two 5 mg inhalations) once twice daily daily Children (≥7 years) 10 mg (two 5 mg inhalations) 10 mg (two 5 mg inhalations) once twice daily daily Treatment regimens adapted from reference 17. Please note that in Canada antivirals are not authorized for the routine treatment of seasonal influenza illness in babies younger than one year of age. Such use may be considered on a case-by-case basis.*Oseltamivir is administered orally without regard to meals, although adminis tration with meals may improve gastrointestinal tolerability. Oseltamivir is available in 30 mg, 45 mg, and 75 mg capsules, and as a powder for oral suspension that is reconstituted to provide a final concentration of either 6 mg/mL or 12 mg/mL. If the commercially manufactured oral suspension is not available, the capsules may be opened and the contents mixed with a sweetened liquid to mask the bitter taste or a suspension can be compounded by retail pharmacies (final concentration 6 mg/ mL). When dispensing commercially manufactured oseltamivir (Tamiflu Powder for Oral Suspension [6 mg/mL or 12 mg/mL] Hoffman-La Roche Ltd, Canada), phar macists should ensure the units of measure on the prescription instructions match the dosing device; †Weight-based dosing is preferred. However, if weight is not known, dosing by age for treatment of influenza (give two doses per day) or prophylaxis (give one dose per day) in full-term infants younger than one year of age may be necessary: 0 to 3 months = 12 mg per dose for treatment (not for prophylaxis); 3 to 5 months = 20 mg per dose; 6 to 11 months = 25 mg per dose; ‡Current weight-based dosing recommendations are not intended for premature infants. Premature infants may have slower clearance of oseltamivir due to immature renal function, and doses recommended for full-term infants may lead to very high drug concentrations in this age group. Very limited data from a cohort of premature in fants demonstrated that oseltamivir concentrations among premature infants given 1 mg/kg body weight twice daily were similar to those observed with the recom mended treatment doses in term infants (3 mg/kg body weight twice daily). Observed drug concentrations were highly variable among premature infants. The Infec tious Diseases Society of America’s 2011 recommendations for paediatric pneumonia suggest 2 mg/kg/day divided twice daily. Currently available data are insuffi cient to recommend a specific dose of oseltamivir for premature infants; it is strongly suggested that an infectious disease physician or clinical pharmacist should be consulted; §Zanamivir is administered by inhalation using a proprietary ‘Diskhaler’ device (Relenza, GlaxoSmithKline Inc, United Kingdom) distributed together with the medication. Zanamivir is a dry powder, not an aerosol, and should not be administered using nebulizers, ventilators or other devices typically used for administer ing medications in aerosolized solutions. Zanamivir is not recommended for persons with chronic respiratory diseases, such as asthma or chronic obstructive pul monary disease, which increase the risk of bronchospasm. INFECTIOUS DISEASES AND IMMUNIZATION COMMITTEE, CANADIAN PAEDIATRIC SOCIETY | 5 References 1. American Academy of Pediatrics. Influenza. In: Picker ing LR, Baker CJ, Kimberlin DW, Long SS, eds. Red Book 2012 Report of the Committee on Infectious Dis eases, 29th edn. Elk Grove Village: American Academy of Pediatrics, 2012:439-52. 2. Centers for Disease Control and Prevention. Influenzaassociated pediatric deaths – United States, September 2010 – August 2011. Morb Mortal Wkly Rep 2011;60:1233-8. 3. MacDonald N, Bortolussi R; Canadian Paediatric Soci ety, Infectious Diseases and Immunization Committee. The new influenza A virus: A/Mexico/2009 (H1N1) prac tice point for caregivers of children and youth. Acc cessed January 23, 2013. 4. Dawood FS, Subbarao K, Fiore AE. Influenza viruses. In: Long SS, Pickering LK, Prober CG, eds. Principle and Practice of Pediatric Infectious Diseases, 4th edn. Edinburgh: Elsevier Inc, 2012:1149-58. 5. Neuzil KM, Zhu Y, Griffin MR, et al. Burden of interpan demic influenza in children younger than 5 years: A 25year prospective study. J Infect Dis 2002;185:147-52. 6. Kitching A, Roche A, Balasegaram S, et al. Oseltamivir adherence and side effects among children in three Lon don schools affected by influenza A (H1N1)v, May 2009 – an internet-based cross-sectional survey. Euro Surveill 2009;14:19287. 7. Barr CE, Schulman K, Iacuzio D, et al. Effect of os eltamivir on the risk of pneumonia and use of health care services in children with clinically diagnosed in fluenza. Curr Med Res Opin 2007;23:523-31. 8. Piedra PA, Schulman KL, Blumentals WA. Effects of os eltamivir on influenza-related complications in children with chronic medical conditions. Pediatrics 2009;124:170-8. 9. Gums JG, Pelletier EM, Blumentals WA. Oseltamivir and influenza-related complications, hospitalization and healthcare expenditure in healthy adults and children. Expert Opin Pharmacother 2008;9:151-61. 10. Kimberlin DW, Shalabi M, Abzug MJ, et al. Safety of os eltamivir compared with the adamantanes in children less than 12 months of age. Pediatr Infect Dis J 2010;29:195-8. 11. Acosta EP, Jester P, Gal P, et al. Oseltamivir dosing for influenza infection in premature neonates. J Infect Dis 2010;202:563-6. 12. WHO. Guidelines for pharmacological management of pandemic influenza A (H1N1) 2009 and other influenza viruses. Revised February 2010. Part I. Recommenda tions http://www.who.int/csr/resources/publications/ swineflu/h1n1_guidelines_pharmaceutical_mngt.pdf (Accessed August 2012). 13. CDC. Interim Guidance on the use of influenza antiviral agents during the 2010-2011 influenza season. http:// www.cdc.gov/flu/professionals/antivirals/guidance/ (Ac cessed August 2012). 14. Hackett S, Hill L, Patel J, et al. Clinical characteristics of pediatric H1N1 admissions in Birmingham, UK. The Lancet 2009;374:605. 15. National Advisory Committee on Immunization (NACI). Statement on seasonal trivalent inactivated influenza vaccine (ITV) for 2012-2013: http://www.phacaspc.gc.ca/publicat/ccdr-rmtc/12vol38/acs-dcc-2/indexeng.php (Accessed January 8, 2013). 16. Blanton L, Peacock G, Cox C, et al. Neurologic disor ders among pediatric deaths associated with the 2009 pandemic influenza. Pediatrics 2012;130:390-6. 17. American Academy of Pediatrics. Antiviral drugs. In: Pickering LR, Baker CJ, Kimberlin DW, Long SS, eds. Red Book 2012: Report of the Committee on Infectious Diseases, 29th edn. Elk Grove Village: American Acade my of Pediatrics, 2012:841-7. CPS INFECTIOUS DISEASES AND IMMUNIZATION COMMITTEE Members: Robert Bortolussi MD (Past Chair); Natalie A Bridger MD; Jane C Finlay MD; Susanna Martin MD (Board Representative); Jane C McDonald MD; Heather Onyett MD; Joan L Robinson MD (Chair) Liaisons: Upton D Allen MD, Canadian Pediatric AIDS Research Group; Michael Brady MD, Committee on Infectious Diseases, American Academy of Pediatrics; Janet Dollin MD, College of Family Physicians of Canada; Charles PS Hui MD, Committee to Advise on Tropical Medicine and Travel, Public Health Agency of Canada; Nicole Le Saux MD, IMPACT (Immunization Monitoring Program, ACTive); Dorothy L Moore MD, National Advisory Committee on Immunization (NACI); John S Spika MD, Public Health Agency of Canada Consultant: Noni E MacDonald MD Principal author: Upton D Allen MD Also available at www.cps.ca/en © Canadian Paediatric Society 2017 The Canadian Paediatric Society gives permission to print single copies of this document from our website. or reproduce multiple copies, please see our copyright policy. 6 For| permission THE USE toOFreprint ANTIVIRAL DRUGS FOR INFLUENZA: GUIDANCE FOR PRACTITIONERS, 2012/2013; PAEDIATRIC SUMMARY Disclaimer: The recommendations in this position statement do not indicate an exclusive course of treatment or procedure to be followed. Variations, taking in to account individual circumstances, may be appropriate. Internet addresses are current at time of publication.