Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Cardiac Diagnosis from Examination
of Arteries and Veins
By NOBLE
0.
FowiLn, M.D.,
A"N
Inspection of the Neck
WILLIAM J. MARSHALL, M.D.
Neck Vein Distention
The degree of distention and the quality of
the pulsations in the external and internal
jugular veins should be examined in detail.
The external jugular veins, which are often
distended abnormally in patients with congestive heart failure, may at times be invisible
because of increased venous tone. As a result failure to appreciate the degree of distention and the level of pulsation in the internal jugular veins beneath the sternocleidomastoid muscle may lead to the erroneous
conclusion that the venous pressure is normal.
Distention and pulsation in both external and
internal jugular veins are normal when the
patient is in the recumbent position and the
veins are below the level of the manubrium
sterni. When the head and chest are elevated
450 from the horizontal, distention of these
veins and their pulsations should extend not
more than 1 or 2 cm. above the manubrium
sterni. If they ascend higher, the venous pressure is elevated. In some patients with congestive heart failure in whom the venous
pressure elevation is borderline or questionable, valuable information may be obtained
by sustained compression of the abdomen.
The compression may be made in the right
upper quadrant; however, if the patient has a
congested, tender liver, abdominal pressure
should be exerted elsewhere. At this time it is
essential that the patient not hold his breath
and thereby perform a Valsalva maneuver,
which will distend the neck veins in the absence of congestive heart failure. If one observes that abdominal pressure exerted during
normal breathing causes a rise of the vertical
level of pressure or pulsation in the neck
veins, failure of the right heart is strongly
suggested. This sign is called the hepatojugular reflux. Unilateral or bilateral distention of
the neck veins without pulsations in the sit-
Distinction between Arterial and Venous
Pulsation
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
TH E examiner may acquire much valuable
information pertaining to cardiac diagnosis by careful inspection of the major vessels
in the neck with proper tangential lighting. It
is important that the quick-rising carotid arterial pulsations be not confused with the
more gradually rising internal jugular venous
pulsations, which also originate beneath the
sternocleidomastoid muscle. Distinction between the two may be made in the following
manner. The carotid arterial pulse is single;
ordinarily two or three venous pulse waves
can be seen with each cardiac cycle. Internal
jugular venous pulsations are readily obliterated by light pressure over the sternomastoid muscle just above the medial end
of the clavicle, whereas carotid arterial
pulsations are unaffected. Venous pulsations
can be altered by changing the position of the
patient. The veins usually become more distended as the patient lies in a horizontal position and less distended as he sits upright. If
the venous pressure is low, or normal, the
venous pulsations are more evident when the
patient is lying flat. In general, with higher
venous pressures, the venous pulse is best
seen with the patient more upright. If the
venous pressure is elevated because of congestive heart failure, sustained abdominal
compression will cause the venous pressure
to rise and the venous pulsations to ascend
higher in the neck.
From the Cardiac Laboratory, Cincinnati General
Hospital, and the Department of Internal Medicine,
University of Cincinnati College of Medicine, Cincinnati, Ohio.
Supported in part by Postgraduate Training Grant
HE-5445-04, U. S. Public Health Service.
272
Circtdation, Volume XXX, August 1964
SYMPOSIUM-PHYSICAL DIAGNOSIS
273
EKG
Si
PHONOCARDIOGRAM
._
S2
4
SI
C
44 II
A
S]
e,
s2
z
t
5C
5s
p,
2
¢r
A
,2
*1
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
JUGULAR
VENOUS
PULSE
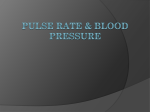
Figure
Simutltaneoufsb recording of ntormlal jul-alr vcenous pulse, lecetrofb.ticliogiatrn, aa(lpdlponocalriogrami. The a, c, and V waves of the juigiulair pulse are cleahj slo)tbn.
tiiig patient may reflect obstruiction of the
superior vena cava or the inniominate vein
ratlher than heart failire. Collateral veins over
the upper clhest, absence of lheart disease, ancl
lack of lhepatic engorgement are confirmnatory
evidence of su-iperior caval obstruction.
Neck Vein Pulsations
It is important that the examiner analyze
the pulsations in the neck veins. Ordinarily
three positive pulses can be seeni for each cardiac cycle (fig. 1). These are the a, c, an(l
v waves. The a wxave is related to atrial
conitraction. There is a negative wave or
trough following the a wave, which is called
the x descent and is related to atrial diastole anti perhaps to downward movemenlt
of the tricuispid valve dulring ventricullar systole. The second positive wave is the c wx ave
produiced by lulging of the tricuispid valve at
the onset of ventricular conitraction. The c
wave is invisible in many niormal subjects in
the right atrial pressure pulse record, but
in the neck is often exaggerated by the transmitted carotid arterial puilse. The third xvave is
tlhe v wave, which is produced by passive
Circulation, Vs/awe XXX, A gnst 1964
atrial filliing. The v wave is followved by a
negative xv ax(e, the y descent, wlxiclh is produiced duIiring diastole as blood flows from the
riglht atritum to the right ventricle. \Vhen a
normal per-soii inlhales, the vertical level of
plsations in the neck veinis falls slightly with
the decrease of intrathoracie pressure. Whlen
the level of ptulsations in the veinis rises duiring
inspiration, this is an alnormal phenomenon
(Kuissmaui's sign). Altlhouigh generally regarded as a sign of conistrictive pericarditis,
this physical findiing is not diagnostic of constrictive pericarditis, since it may be found
in some patients wxith congestive hieart failure.
A dlisproportionate increase in the amplitLide of the ci wave is a valuable plhysical sign
that occIirs in certain disor-ders in wl iebl outfloNx fromii the riglht aitriumin is impeded. Among
these are tricuspid stenosis and tricuspid atresia (fig. 2). Very large ai waves are fouind in
patients wh1o lhave moderately severe or severe
pulmonie xvalvLlar stenosis. In these patients
tlhere are right ventricuilar hypertroplhy and
decreased right xventricular compliance, xvhich
rereder righlt atrial emptying more difficult.
FOXVLER, MARSHALL
274
The a wave is increcased for- a similar reason
in patients xvho lhave mioderately sexvere, or
severe, pulmonary liypertensioni. As a result,
a prominent a wave may l)e observed in patients who have severe mitral stenosis witl
pulmonary hypertension and in patients vitlh
congenital lheart disease w ith l.eft-to-right
shunting complicated by pullmonarv hypertension (Eisenmenger's complex) . Large a
waves may be found iin patients witlh otlher
aS
varieties of pulmonary lhypertension sucal:s
primary pulmonary lhypertension, repeated
S,
S2 OS.
S?
pulmonary embolism, and cor puilmonale related to plulmonary disease.
Venous Pulse Patterns in Cardiac Arrhythmias
The axwave is absent in patients with atrial fibrillatioln. In some patients witlh atrial
fluttter it is possible to discern very rapid a
wavaes occurrinig at a rate of approximately
300 per minuite, with slower c and v waves at
a rate of 150 or 100 per miniute, or at an
irreguilar interxval, whiicl depends upon the
degree of atrioventrictiular block. In patients
S2 0.S.
SI
OS
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
a wave
a wove
a wave
FiguLre 2
Jugular venous pulse recotiitig shooing giant a twaves ini
and tricuspid steniosis.
a
paticent twithi rhletumatic hecart disease
Ss
Phonocardiogroma _m 10
. -6 1-0
.4
d
s,
:-11
''
.C
connCl
c
1,.# .o-
-h
'I
11
5
1
1.
---T-
111
l tm.
--
-1
-1 ~
ccnn
a
f:
'f/
jugular
venous
pulse
. jt
--
ECG
K.
1-
*1.1
QRS
P
P
~~~~1
^
L=
S
-eQRS
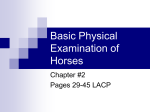
FU iguire 3
Jugular venioul.s puilse recording, demornstratinig eannroni a wares irn a patient witih coimplete atrioventricular block. The canntoan lttves occuri. wh12et the a waves fall within the QT2l interval of the
electrocardiogram.
(,rrcuiatizon, Volumae XXX, August 1964
SYMPOSIUM-PHYSICAL DIAGNOSIS
275
EKG
PHONO-
S2
S,
-1
S,
s2
Ad ..
CARDIOGRAM
CAROTID
PU LSE
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Figure 4
n iard-iogrri.atn and el ctr.ocardiogi an.i1
Simuiltaneous recor.dintg of normal carotidi pulsc thitli1otioe
xxith coimplete atrioventricular 1lock the diagnosis may be made or stronigly stuspecte(1 by
inispection of the neck vein:s. The atrial waves,
or a waves, usually occur at a normal rate of
60 to 100 times per minlute. The c and v
waves occur less often, usulally about 40 times
per minuite in the aduilt. The atrial rate, (leterimined from the neck veins, is ustually more
rapid than the ventricular rate, xvliclh may be
confirmed by palpation of the pulse or auscultationi of the precordium. The most significant
clue to complete atrioventricular block from
inspection of the neck veins are cannon wxaves
(fig. 3). The cannon xvaves are intermittent
gianit a vaves produced when atrial systole
occurs at a time when the tricuspid valve is
closed. Thtus, if atrial systole occurs at a time
corresponding to the QT interval of the electrocardiogram, narmely, betveen the first and
second lheart sounds, very large a waves will
be produced. Cannon a waves occur regularly in nodal rhiytlhms antl in first-degree
atrioventricular block with very long atrioventricuilar conduction time, but occur irreguilarly in complete atrioventricular block.
Whlen there is organic or relative tricuispid
Circua/ion, Vo/unIt XXX, AuguCt l96)C
ius.ufficieney, a positive regurgitant venous
xx7 ave precedes the v xxwave. The c and v waves
tenld to mierge xvith this regurgitant xvave, so
that they are in effect replaced by one large
positive pulsaItion. By far the commonest
cause of this physical fincding is relative triculspid instufficiency. Regurgitant venouis
xvaves are a common observation in patients
xx ithl riglht ventricular failure reega,rdlless of
the catuse, and are often found in patients
vitlh systeinic lhyperteinsioni or coronary disease xwith botlh left and righlt ventricuilar failure. Reglurgitant wavxes may be found vhlen
tlere is no mturmulr of tricuiispicl inisufficiency.
In patients xvitlh constrictive pericardlitis, inspection of the neck veins yields valtuable information. Tlhe level of the venotus pressure is
determined by the distention of the veins and
b)y the heiglt of the Pulsations. The venous
pressure is almost alwx ays increased in constrictive pericarditis. The Kussmaul sign may
be present, namiiely, the vertical level of venous pulsations may ascend with inspiration.
The a and v waxaes tend to be increased but
the trough produced by the y descent tends
to be the predo1minanit vxenous event.2 In pa-
FOWLER, MARSHALL
276
tients xvithl tricuspid stenosis xxho have prominent a waves, and at times large u, waves,
the y descent is graduial.
Carotid Arterial Pulse (fig. 4)
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Normally the carotid arterial pil.sations
may be invisible if the patient is stocky or
moderately obese. They may be readily visible in a thin person. Bounding carotid arterial puilsations suggest that the systemic
arterial pulse pressure is increase(l and are
usually associated vith bounding radial and
femoral pulses. Most commonly stuelh exaggerated carotid arterial pulsations are caiused
by apprelhension. The comimonest patlhologic
cause is aortic valvular instufficiency. However, they may be associated witlh otlher
causes of increased systemic arterial pulse
pressure, including patent ductis arteriosus,
other forms of congeniital conimunication )etween the systemic circulation and the riglht
heart, xvith severe aniemia, \vitlh syst:emic arteriovenous fistula, and xw itli thlyrotoxicosis. A
bounding carotid arterial pulse is strong evidence against severe uincomplicated aortic valvuilar stenosis but brisk carotid pulsations often occur with idiopathic lhypertroplie sillaortic stenosis. The carotid arterial pulse is
often increased in coaretation of the aorta.
Carotid arterial pulsations may be (IJuiet or invisible in patienits with severe aortic stenosis,
and when there is systemic hypotension. It is
Right
Carotid
ThMPI.
-
wJi
WsJo
00-----7 -!" i!
importaint to call attention to imnilateral increase of carotitd arterial puilsations. These are
imost commonly observed just above the right
clavicle and are often associated with an apparent wideniing of tl-he carotid artery. This
finding is often misiniterpreted as an aneulrysm
of the carotid artery 3 or of the iiinoininate artery. It is most commonly catused by tortuiosity
or kinikinig of the common carotid artery in association with arteriosclerosis or hypertension
bitt withouit true aneurysm formationi. This
disorder is most commonll in hypertensive
women of middle age and beyond.
Palpation and Auscultation of the
Neck Vessels
The qtiality of the carotid arterial ptilsation
mayvbe confirmned by palpation of the neck.
Some patients wvith aortic stenosis have a systolic thrill and mumtinur over tlhe carotid arteries. Hoxxwever, suelh a finding is not (liagnostic of aortic stenosis. It may be observed in
patients xlxo have loud precordial mturmurs
ancd tlhrills of other cauise, especially ventricular septal defect and pulmonic stenosis. A
systolic thrill over the carotid arte-ies may on
occasion be, a nornal fincling in clhildren and
yoiung adults in associatioi wxitlh a supraclavicular arterial brtiit. In suiclh instances the
tlhrill is oftenimore initense over the subelavian
artery, and especially so oni the right side. A
localized svstolic thirill and murmuntir over the
4
.'. t-
!-~ -.
PI"'t-~
..
....._..
..
-t...
--
1745qnpwirl
._ _W_ . . . ............ . . . .
. . . . . . .......
t~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~._. ._ _._ _ . . . . .
A
Om..iiii;iigiw
-w
ortic
_*........................................ .--..-....
.-
. . .-_-._. . . . -_ _. . . . . . . . . . .
... ._....._....._..........__.......__
m,z1,p1,_,:.____
__
I .. .WI_____A______
Iz_._
______
___.j___l_;j__i_m.__ ._ iV~~~~~~~~~~~~~~~~~~~~.
_._
._
W.B., Carotid Murmur
ECG.
Figure 5
1
Phtonacard{:iogram.171 demonstrating af (,cZ1ontinuouis outir77iur ovec'r thte right carotid artery int apatient
wvith partial obstruction of the carotid aritery demonstrated by arteriography.
(ir- lation, TVoljime XXX, Aegust 1964j
277
SYMPOSIUM-PHYSICAL DIAGNOSIS
Sl M
Phonocordiogrom
q
>
SM
5b
S2
N '
52
SM
S
$2
S SM
S2
-
AortiC
Area
Phonocordiogram
Right
-~
vft;
W
S
FP
Suprocloviculor
Auec
ECG
Figure 6
Simultaneous pihonocardiograrns fromi tic second rig/it intcureo,stal .s)ace and right stiipraclaticicular
area, showinjg tariasmiissioii of a snpraclaular briti to fthe aorlic area ini a ormiail yfoling 21an.
cOr1()rrcotis diagntiosis of aortic stenoNote thle brief duration of the mtiruaratr. In suci instances at
sis iiiay be maide.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
carotid artery may 1)e a reflection of partial
obstruction (f the carotid artery, inost comnmonly cauised by arteriosclerosis.4 In Some
such instances a more severe obstruction may
produice a continuouls tlhrill and muirmulr over
the carotid artery (fig. 5). Bilateral systolic
carotid muiruLirs are cormmonly founird ill hiigl
carcliac output states, suichl as anemia, hernalc sys1eri, thyrotoxicosis, hepatic fanilure,
temic arteriovenouis fistula.
It is essential that the examiner 1)e familiar
with two common cervical mturmnurs fou-cnd in
normal children and youing people. These
mnurmurs are often misinterpreted.
Cervical Venous Hum
The first of these is the cervical venious
UInm. The cervical venous hutm is a continuous murmuir with diastolic accentuiationi. It
is best detected juist above the medial enid of
the clavicle over the sternomastoid mnuscle.
Usually it is readily obliterated by light pressuire with a stethoscope or tlhe finger over the
internal juguilar vein. This murmulr is uisually
detected with the individulal in the sittingy
postuire. It almost always disappears or becomes very faint wh:en hie lies down. It can be
increased by turning the lhead a-xay from the
side being examined or by elevating the chin.
The cerviccal venous hlum is found in 9.5 per
cent of clhildren between the ages of 5 ancd
15 years, anid somexlhat less frequeently beloxv
the age of 5 years.) In young adtults it may be
Circwlation VolYmuocAegimst
XXX,
196i4
fouind as oftetn as 75 per cent of instances.
Of especial ii-lportance is the fact that in 10
to 19 per cenlt of subjects between irnfancy
and 49 years the inmurmuir may be lheard below the clavicle, and at timnes may be heard
in the second righit or left intercostal spaces.
Wh1en tlhe munitrunir is discovered adjacent to
the upper sternum and is not traced to its
origin in the nieck, it ml-ay he coniftised on the
left w ithi the mnurmuir of patent duictus arteriosuis, ancd oni the righlt with the murmurs of
aortic stenosis and insufficiency.6 \Vlhen beard
in the neck alone the venouis hium miay be
mistaken for the muirmuir of an arteriovenous
fisttula. The proper diaguosis may be almost
always made by attention to the following
points. (1) the murtmur can be obliterated by
lighlt o}r moderate pressuire over the internal
jutgular vein; (2) the murmnur becomes faint
or disappears when the individual lies down;
(3) the murmullr h-as diastolic accentuation
rather than the tusual systolic accentuation of
a muirmur of patent ductus arteriosuis or arteriovenotus fistila.
Supraclavicular Arterial Bruit
Anotlher very common benign murmur
found in the neck cind the adjoining supraclavicular area is the supraclavicular bruit.7
We lhave observed this milurmuri in children
as youing as 2_ years of age. It is also quite
common in teenagers. The muirmur occurs in
early systole (fig. 6) and is uisually loudest in
F(OWLER, MARSHALL
278
and 8). The mturintmr imayvbe refer-red inito tlhe
aniterior thorax. On the right side, its detection over the aortic area may lead to a mistaken diagnosis of aortic va,ilvular stenosis. Oni
the left side, its dliscoxvery in the seconcl left
initercostal spee mnay lead to ani erroneous
nliaignos.is of pulmonary valve steniosis. The
the supraclavicular fossa and oxver the carotid
artery. The mturmu.r may he of grade IV or V
intensity anti may 1)e associated wxith a thrill.
The muirmur may be obliterated in most instances. bhut not all. by compressing tlim sutb)clavian artery on the same sinle uintil the
radial puilse on that sidce disappears (figs. 7
SM
51
Supraclaviculor
Phonocorcio-
Sz
SM
51M
joegin Subclovian Artery Compression Sp
S
.4
gram
A
VI----
-i .1
ECG
1,
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Complete
5i
Supracloviculor
SM
Artery
*
Sa
Stibclaovion
'Cmpression Sh
S2
Vt t
Phonocardlogrom
~
ECG
1-250se
Figure 7
Phonocardiogramn shotowinlg the efect of suibclaviain artery comptl)ressioni uiponI a srluraclauicular
brutit. The murm7iuir is accenituated (aS' the (at ery is pairtially occluded, and then dlisappears when
fturther pressure is exerte(l. The muzrmur isappears as the ipsilaterail radial pulse becomes in-s
perceptible.
Partial Release
of Subclovion
Artery Compression
SI
SM
Sl
52
SM
S?
Supraclaviculor
Phonocardiogram
ECG
1:
IComplete Release of Subclovian Artery Compression
S SM
S2
St
SM
S2
St
SM
5z
Suprclovicular
Phonocordiogroin
ECG
Figure 8
Phonocardiogram demonstratinfg thfe reappearance of the sutpraclavicular bruit shown in fig. 7
as the compressicm of the subclarian artery is grraduailly released. The murmlutir is at first quite
loud, and then returns to its usual intensity.
Circulation, Volume XXX, Ausust 1964
SYMPOSIUMPI-PIYSICAL DIAGNOSIS
clistinction may be mnade, as a rile, lby careful
attention to the follow i7g points. First, the
murmur is louder in the supraclavicular area
than in the thorax; secondly, tlhe murmtuir is
of short duration, usually being limiter] to the
first half of systole; and thirdly, the murmuir
may u-sulally be obliterated by compressing
the subelavian artery on that side against the
first rib until the radial pulse disappears.
'Witlh light compression of the subclavian artery the muirmuri. uisually becomes louder (fig.
7).
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Auscultation of the Thorax
An important featuire of cardiovascular examiniation is the careful autlscutltation of the
thorax for mnurmurs that may originate outside the lheart. Not infrequently suiclh imtirmtirs may be heard over the precorldiuiul. If
the physician does not examine the remainder
of the thorax, an erroneouis diagnosis of cardliac valvila]lr disease may be madei, when in
fact none exists. An extracardiac systolic or
continuiotus murmtiur suggests certain diagnostic possibilities. These iniclude (1) coaretation of the aorta; (2) pseudotriincus arteriosus; (3) pulmonary arteriovenous fistula; (4)
pulmonary branch stenosis; (5) anomalous
pulmonary artery arising from the aorta; (6)
internal mammary arteriovenous fistula; (7)
other anomalous arterial branches arising
from the aorta or the subelavian artery. We
xvill discuss only the more common of these
possibilities.
With coaretation of the aorta there is often
a systolic murmur louder over the back of the
clhest, especially betveen the scapuilae, than
over the front of the chest. The studies of
Spencer and associates lhave shovn that this
murmuir often arises xvitlhin the coaretation itself, althouglh in some patients there is an
additional murmur of aortic valvuilar disease.
When the coaretation is severe, vlth an opening 2.5 mm. or less in diameter, there may be
a continuous murnmur over the back of the
chest. Althouglh in some instances a svstolic murmur accompanying coarctation
of the aorta may arise from dilated collateral intercostal vessels and scapular vessels,
Circulation, Volume XXX, Augst 1964
279
in most instancli'es the continuous murmur
arises from the coarcted area. The pulsation
of enlar-ged collateral arteries may be palpable anAd ()ccasionally vZisible in the inter-
scapular spac(s or beneath the angles of the
scapulae. The dliagniosis is confirmed by the
dlemoinstrationi of w eak anid delayed femoral
arterial p)tllses.
Patients wxlho have increased bronchial collater,al circuilation associated with pulmonary
atresia (psedtiotrunciis arteriosus) commonly
have a continuous murmur over the thorax.
This is ofteni louidest over the posterior thorax.
Patients xx ith p)ulmoniary arteriovenous fistulaave often eitlher cvery long systolic
lae
murtmriiIIi or a continuious mnuri-mur over the
Figure 9
A ugiocardiogramn revealing ai pulmonary arteriovenous
fislula in the left lower ltimg. The arrow indicates a
pulmonary t(ein cvonnnnieotrng between the fistula
and thce left atriumol Thle pulmonary artery, which
supplies the fistula, is just above the vein. This patient had a long systolic murmnur over the chest in the
area of the flstula.
FOWLER, \ IARSHALL
280
tasia, stronigly suggests ptulmon a rv l)ratclh
stenosis. Radiologic stuidies are desirable to
confirm the diagnosis. Patients witlh plilmonary 1)ranch stenosis oftein have associated
cardiac (lisease. Atricl- septal (lefect and
mIIomalolus pulmionary veiouits drainage h1ave
been commonly fouincd in ouir patients. Others
haxe founid that this disordler is not uincomiiimon in association xw ith tetralogy of Fallot.
Here it is ofte nimissed unl.ess the angiocardio-
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
thorax. The mu:rmulr may be increased in intensity and duiration by inspiration. Many patients with this disorder lhave accompanying
Osler-Weber-Rendi disease or hereditary
heemorrhagic telangiectasia and may be found
to have telangiectasia of the tongue and perliaps over the fingertips. This diagnosis is
most clearly demonstrated by angiocardiography (fig. 9).
Pulmonary branch stenosis mnay be associlted with either a long systolic muirmuir or
a continuouis mu.rm-ur. Stucdies mnade by Eldridge and associates 9 hiave shown that milodcrate compression of ani artery causes a systolic murmulr, but more severe compression
causes the pressuire proximal. to the obstruction to exceed that distal to the obstruction
dulring bothi systole and diastole. This observation explains the continuouis murmu-1r that
may be associated with this disorder. Thuiis
patients witlh pulmonary branch stenosis may
be fouind to have a Jlong systolic murmulir or
a continuLouis mutrmur that originates outside
the heart (fig. 10). This observation, in the
absence of the plhysical findings of coarctation of the aorta, in the absence of cyanosis,
and in the absence of hereditary telanlgiec-
gram is
carefuilly stuidied.
Systemic Arteriovenous Fistula
Thlis disorder has been referred to earlier
as a cause of increase(l carotid arterial puiilsatiois. Systemie arterioveniouis fistuilae that produce cardliac dlisal)ilitv are most commonly
single, large, acqulired lesions, altlhoulglh they
are occasionally mu-itiltiple, small, congenital
lesions. It is important to inquire concerning
a Isiitory of traurma or of at surgical operation.
The detection of a -X7ide puilse pressure xvithout a c¶ardiac muir-mulr suggests that careful
auisculltationi and palpation be performed over
all scars and areas of previouis traumtiiia or surgical operation. In typical instances suchli patients, in addition to a bouinding lulllse, have
PULMONIC AREA -2 H.S. Split 0.03 - 0.06 sec.
Aortc
A 0S#6n
L.
li ll
t411
'..
t> _ _>veX-~~~~~~~~~~~~~~~f
i +i. g.S 4 .~ - . + . N~s H;F
W-7
LSB
4 ICS
1"
.11
N.McF. Pulmonary Branch Stenosis
ECG
i
r
1
Figulre 10
Phionocardiogrant shlo.tintg a long sy,rtolic murmur over the precordium int a partient with pudlmnonary (rterial brtanch stenosis.
Ci culaI/tcon, Volii7J/c XXK, Augmot 1,964
200]
x
200-
ARTA
t>
- p....
100-1
Of
ml j.,
1001-
E0-
sI
E
6
O
O -.
PE........IU*
AR. M
+5
0 ..
,+.
0-
PS -aEa t.
M7
15 ...E.BB
iO
0-
'
i.
C1
x
-10
RA.......
-
E
-k-
-20 -
+6000-
FLOWY N
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
E~ ~ .5SEMs:.w't
281
SYMPOSIUM-PHYSICAL DIAG`NOSIS
DESC¢ENPNGAORTA
.LOR N PESCENQIN dACIRTA
+60001-
0
+40O0-
s:
(9
~~~~~~~~~~~~~~~~~~~~~~~~~~~~...... .........~
..
E +2000]
.....
-20001,
1
73 85 82
cc: 60 83 8 82 70
Paper Speed 25 mmsz/sec
8'
2 000
cc: 2.8
77
,7
08 23
69
Paper Speed 25mm/sec.
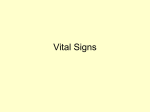
Figure 1 1
62
56
48
389
2.7
0-8 13
6.5
54
pleuiral sj)ela,and( flow recording in the
experimental c(arrcliac tam lponad1e. In the
dlecline of intro-pletiral
onset of inspiration, indlicaited by the
control record
pressre4, there is a decrease of aortic flotr and pressure. The record ont the right is nmade
after cardiac tau p?1i)a(tle Wvas /)t)dltced bl the ittjeCtidon of phtioyslogic salin-te solhitio-n into the
pericairdiol space. 71'le perieardiol pressullre is icreased approximiiatelil 10 n7uni,. Hg from the
Presstire
finro the aurt,
(dog twhiich
the left, icithi the
recordings
d-escenditng
aorta
opt
of
a
and
te(as
subjectecl
to
control. There is striking paradoxical piLse in the aortic pressulre recordings. The i-nspiratory
fall of blood pressure is ac,,coupanr1iedl byi considerable decline in aortic stroke faote during
a
a
inspiration.
ceontiiitiutis murmulr ,tniil palpable cointinuithlrill over the site of the lesioni. If tlhe
fistifla can be ol)literatte(l by imanutial compression there is clactracteristically a fall in systolic
1loo0d presstire a(lnd rise in (liastolic b)o100(
pressuire and slowing (of tile leart, the latter
a
a
otis
tlhc radial pulse. Neithier can we consider the
several cauises of xveakness or obliteration of
botlh radial or femoral pulses.
oine
or
The Paradoxical Pulse
a
being called Branhiam's sign. Suchli phlysical
findings are more likely if the fistuila inv olves
the larger arteries ineluiding the aorta, its inmmnediate branchies, or the femoral arterv. As
stated earlier, sulchI fistuilate may follow surgical proceduires and rarely miay follow a nephrectomy. The diagnosis imay be confirmed by
arteriography.
Palpation of the Pulse
Space (Toes not t)erunit a disetssion of the
diagn.osis of the variouis car(liac arrhytlhmias,
whlichi may be suggested fromi palpation of
Circrrlation. Vol7l]Ji XXX.
At
tgitur 1964
W7e shoul.d like to (levote ouir attention to
paradoxical puilse. A paradoxical pulse is
an abnornmal (lecline in systolic blood presduiring inspiration. It is sell knoxn that
sxvstolic blood pressuire normally falls several
mm. of mercury ssith inspiration. Stu.dies of
laboratory lhave
experimnental animals in
shiowrn that there is in fact a decrease in left
tile
sure
our
ventricular stroke outpult duiring normal inspiration 10 (fig. 11). Thlis decrease is believeed to be related to the expiratory fall of
right ventrictular ouitpult and the delay in
transmission tlhrouiglh th-ie puilmonary circulation. Wheu systolic blood pressuire falls as
F0\VILER, NI ±ATRSHALL
19i8 2
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
much as S or 10 mnmi. Hg dutiring quiet inspiration, a p)aradoxiecl pulse is saidl to be
prescsnt. Wh1en the para(loxical puilse is nlolcrate, it is best de-tected (luring 10lo01 pressture measturement while the patient l)reltlhes
normally Deep inspiration ixv cause 10 or
15 mm. fluettuation in systolic 1)loo0( pressure
in a normal. persois hut shou.ld oiot cauise tIle
radial. pulse to disappear. T1he latter event
suiggests that there is at significamt paradoxical
pulse. Paradoxical lpulse lhas been most comn
inonly described in association \vxith p)ericairdlial disease thazt compresses thehleart eitlher
l) flutd or scar tissue. It is important to state,
that a )aradoxical plulse is inore commonly
cause.d by emphli sem-na or l)ronehld
ailstlma,
and it may be foundloec,asionally in patients
xwith mnyocardial (lisease.
The meclanism of tlc )aara(loxical puilse in
pericar(lial disease has beeni of considerable
initerest to us. Katz and Gauichat 11 suggested
in 1924 that the paradoxical ptulse of pericarAORTIC
PRESSURE
mm
150
100
Hg 0X;---+ ^
P~~~~~~~~
PLEURAL
PRESSURE
m m gH
K
dial, disease xas produce(l by a greater inspiratory fall. in p)lllmonary venotus pressuire
than in intracardiac pressuire, tlhus producing
a rediuced pressutre gradient for filling of the
left heart (lutring inspiraltioni. Dock 12 has
stated that inspiratorv traction uipon the periecardiuim inncreases iiutraipericardial pressure
and tlmis interferes xx ith cardiac filling dluring
iis1)irationi. Dornhorst anld associates 3 postulated that increased riglt hieart filling duiring
irnspiration compresses the left heart thus interfering withl its filling. Decreased filling in
tuirn leads to decreased left lheart ouitpuit dturinig inispiration. Stutdlies in our laboratory lave
demonstratedl that tlhere is inispiratory increase of riglht hleairt filling duiring cardiac
taiimipoinalO.de)-' If ii(rilgt lheart venous retuirn is
ila(le constaint dutiring eardiae tamponade, the
paradoxica.l ptilse ni longer occuirs (fig. 12).
Studdeni increase in riglht heart filling (lutring
cardiac tamnponadle leatds to temporary dcecrease in left heart otutpuit. Tlhu.s it seemns that
150 -AORTIC
-0
°
PRESSURE
mm H5
[-
~~~~~~~~~~~~~.
.
.|.>!t4 :+..
0.
0
PLEURAL
PRESSURE
I
-.5 l
-0g
S.t<-- +
*
j
PERICARDIAL Z0-~
PRESSURE
m1
CONTROL
H1 l+ .^ 4T-l
..~~~~~~~~~~~~~~~~~~~~~. ......
...<4
10
PERICARDIAL
PRESSUREmmHg
H,
mm
0
t0
0
TAMPONADE
Figure 12
Simnultaneous recording of aiortic pressure, intropleural piessuXre, an-id intrapericardial pressure
in a dog subjected to cardiac tamponade. In this animnal, stystemiiic venouis retuirn wias drained
into a reservoir and the blood pumped at a constant rate intto the righit atrium. The control
record is shown on the left; ont the right, the intrapericairdial pressure hals been increased
approximately 10 mm. Hg by the injection of physiologic saline solution into the pericardial
space. The inspiratory decline of aortic pressur.e is no greater than during the control period
and no significant paradoxical pulse is produced by cardiac tamponade. Compare with fig. 11.
Circulation, Volumne XXX, August 1964
SYMPOSIUM-PHYSICAL DIAGNOSIS
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
the paradoxical pulse is related to increased
inspiratory filling of the right heart which increases the pressure within the pericardial
space. Increased intrapericardial pressure interferes with left heart filling during inspiration. Patients with myocardial disease may
have a paradoxical pulse. This abnormality is
more likely in patients with primary myocardopathy, myocardial fibrosis, and cardiac
amyloidosis. Relative to this point, we have
been able to show that acute cardiac dilatation in the experimental animal in effect
causes the normal pericardium to compress
the distended heart. A sudden increase of
right heart return again leads to a temporary
decrease in left heart stroke output. With experimental respiratory obstruction left heart
output shows no greater-than-normal inspiratory fall.'0 The abnormal inspiratory decline
of blood pressure is caused by the increased
variation of intrathoracic pressure.
References
1. BROWN, J. W., HEATH, D., AND WHITAKER, W.:
Eisenmenger's complex. Brit. Heart J. 17:
273, 1955.
2. WOOD, P.: Diseases of the Heart and Circulation.
Philadelphia, J. B. Lippincott Company,
1956.
3. DETERLING, R. A., JR.: Tortuous right common
carotid artery simulating aneurysm. Angiology 3: 483, 1952.
4. CREVASSE, L. E., LOGUE, R. B., AND HURST, J.
Circulation, Volume XXX, August 1964
283
5.
6.
7.
8.
9.
W.: Syndrome of carotid artery insufficiency.
Early clinical recognition and therapy. Circulation 18: 924, 1958.
FOWLER, N. 0.: Physical Diagnosis of Heart
Disease. New York and London, The Macmillan Company, 1962.
CASTLE, R. F.: Clinical recognition of innocent
murmurs in children. J.A.M.A. 177: 1, 1961.
STAPLETON, J. F., AND EL-HAJJ, M. M.: Heart
murmurs simulated by arterial bruits in the
neck. Am. Heart J. 61: 178, 1961.
SPENCER, M. P., JOHNSTON, F. D., AND MEREDITH, J. H.: The origin and interpretation of
murmurs in coarctation of the aorta. Am.
Heart J. 56: 722, 1958.
ELDRIDGE, F., SELZER, A., AND HULTGREN, H.:
Stenosis of a branch of the pulmonary
artery. An additional cause of continuous
murmurs over the chest. Circulation 15:
865, 1957.
10. SHABETAI, R., FOWLER, N. 0., AND GUERON, M.:
The effects of respiration on aortic pressure and flow. Am. Heart J. 65: 525, 1963.
11. KATZ, L. H., AND GAUCHAT, H. W.: Pulsus
paradoxus (with special reference to pericardial effusion). II. Experimental. Arch.
Int. Med. 33: 371, 1924.
12. DOCK, W.: Inspiratory traction on the pericardium. The cause of pulsus paradoxus in
pericardial disease. Arch. Int. Med. 108:
837, 1961.
13. DORNHORST, A., HOWARD, P., AND LEATHART,
G. C.: pulsus paradoxus. Lancet 1: 746,
1952.
14. SHABETAI, R., AND FOWLER, N. 0.: Dynamics
of cardiac tamponade. Fed. Proc. 21: 103,
1962.
Cardiac Diagnosis from Examination of Arteries and Veins
NOBLE O. FOWLER and WILLIAM J. MARSHALL
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Circulation. 1964;30:272-283
doi: 10.1161/01.CIR.30.2.272
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1964 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/30/2/272.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/