Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
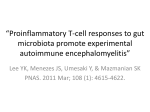
Immunology and Cell Biology (2016) 94, 715–716 & 2016 Australasian Society for Immunology Inc. All rights reserved 0818-9641/16 www.nature.com/icb NEWS AND COMMENTARY Vitamin A restrains γδ T cells Taming pathogenic γδ T cells with vitamin A Catarina F Almeida and Dale I Godfrey Immunology and Cell Biology (2016) 94, 715–716; doi:10.1038/icb.2016.54; published online 5 July 2016 γ δT-cell receptor (TCR)+ T cells (γδ T cells) are a major histocompatibility complex (MHC)-unrestricted innate-like T-cell lineage with a unique and influential role in many different types of diseases (reviewed in Godfrey et al.1 and Vantourout and Hayday2). Although many studies emphasise a protective role for γδ T cells in the context of microbial infection and tumours, they can also have a pathogenic role in autoimmune disease. In this issue, Raverdeau et al.3 show that interleukin (IL)17 secreting γδ T cells contribute to the pathogenesis of experimental autoimmune encephalomyelitis (EAE), an animal model of multiple sclerosis (MS), and that selective targeting of these cells with the vitamin A metabolite, retinoic acid (RA), inhibits IL-17 production and is sufficient to ameliorate this disease. This highlights the central role that γδ T cells have in this disease model and suggests that they may be important therapeutic targets for MS and other autoimmune diseases. MS is an autoimmune disease where T cells target and degrade the myelin sheath surrounding nerves in the central nervous system (Figure 1). The mouse model for this disease, EAE, has been used extensively to understand the immunological mechanisms that contribute to MS. IL-17A, a T-cellderived cytokine, is known to be a key mediator of pathogenesis in EAE4. Furthermore, γδ T cells, which produce IL-17A in response to IL-1β and IL-23 stimulation, contribute to the severity of this disease by inhibiting the activity of FoxP3+ regulatory T cells (Treg) and enhancing the expansion of CF Almeida and DI Godfrey are at Department of Microbiology and Immunology, The Peter Doherty Institute for Infection and Immunity, The University of Melbourne, Melbourne, Victoria, Australia; and the Australian Research Council Centre of Excellence in Advanced Molecular Imaging, The University of Melbourne, Melbourne, Victoria, Australia E-mail: [email protected] or godfrey@ unimelb.edu.au pathogenic IL–17–producing Th17 CD4+ T cells5,6. The active metabolite of vitamin A, RA, inhibits IL-17 production by CD4 T cells and promotes Treg generation7, and it has long been appreciated that RA can ameliorate EAE (reviewed in Raverdeau and Mills.8). Given that the balance between Tregs and Th17 CD4+ T cells tightly correlates with the manifestation, severity and relapse/remit episodes in EAE (reviewed in Fletcher et al.9) and in patients with MS,10 it is important to properly understand the mechanisms and therapeutic potential of RA in this disease. Raverdeau et al.3 demonstrate that RA can suppress IL-17A and IL-17F production by γδ T cells in vitro and in vivo, and furthermore, that this activity on γδ T cells is important for the therapeutic activity of RA in EAE. Myelin oligodendrocyte glycoprotein (MOG)-primed T cells, cultured in the presence of IL-1 and IL-23 (Th17-priming conditions), elicit EAE upon transfer to naïve recipient mice. The disease transferring potential of these MOG-primed T cells is ameliorated by inclusion of RA in these cultures, or by depletion of γδ T cells before culture. Moreover when γδ T cells and γδ-depleted T cells were separated and only the γδ T cells were cultured with RA, before recombining these cells in the presence of MOG/IL-1β/IL-23, the recombined cells also lost much of their disease-inducing capacity. The authors of this study3 demonstrated that Vγ4+ γδ T cells were responsible for RA mediated disease inhibition and that although IL-17 production was inhibited, it had no effect on IFNγ production by γδ T cells. This selectivity likely correlates with the much higher levels of RA nuclear receptor α (RARα) in IL-17-producing (CD27−) γδ T cells compared with their IFNγ+ (CD27+) counterparts3. They also provide evidence that RA leads to a partial reduction in the cell surface level of IL-1R and IL-23R, and a corresponding decrease in phosphorylated STAT3 in response to these cytokines. Given that IL-17 production depends on STAT3 phosphorylation,11 the authors propose that this represents the underlying mechanism of how RA reduces IL-17 production by these γδ T cells3. Because the role for γδ T cells in this disease was not absolute, this raises the question of whether other IL–17–producing innate-like cell types might also contribute to pathogenesis. Candidates worthy of further investigation include IL-17producing mucosal-associated invariant T (MAIT) cells, which have also been implicated in EAE, Natural Killer T (NKT)-17 cells (reviewed in Godfrey et al.1) or Innate lymphoid cells type 3 (ILC3) cells (reviewed in Sonnenberg and Artis12). Previous studies have shown that the timing of administration of RARα agonists can be critical in the disease outcome of EAE. Thus, while administration of these agonists during the disease induction phase can inhibit disease (reviewed in Raverdeau and Mills8), administration at later stages of disease can hamper the generation of immunosuppressive populations involved in the recovery phase, such as myeloid-derived suppressor cells.13 Considering that MS and other autoimmune diseases are generally only detected in patients following disease manifestation, this may limit the therapeutic potential of RAR agonists in the clinic. However, with rapid advances in human genetic profiling and disease prediction, it will be increasingly possible to intervene before the onset of disease symptoms. Another possible caveat associated with translation of the work in the study by Raverdeau et al.3 is that mouse and human γδ T cells are very distinct in terms of their TCR specificity, cytokine production and function (reviewed in Godfrey et al.1 and Vantourout and Hayday2). As γδ T cells tend to accumulate in lesions of patients with MS,14 it will be important to determine if these cells produce IL-17 and News and Commentary 716 Neuron Retinoic acid + Th17 CD4 T cells Vγ4+ γδT cells CD8+ T cell Myelin sheath IL-17 Axon Vγ4+ γδT cell Pro-inflammatory and cytotoxic molecules Stat3 Macrophage Lesions pStat3 RARα IL-1Rβ Activated microglia IL-23R Figure 1 Proposed model for RA modulation of pathogenic IL-17-secreting Vγ4+ γδ T cells in EAE. IL-17 is a driver of pathogenesis of EAE, associated with the demyelination and lesions of neurons. Vγ4+ γδ T cells produce IL-17 in response to IL-1 and IL-23 activation in a TCR–independent manner and this promotes differentiation and expansion of pathogenic Th17 CD4+ T cells. RA interferes with this process at multiple levels. It impairs the differentiation of Th17 CD4+ T cells, prevents DC maturation and antigen presentation and inhibits IL-17 production by Vγ4+ γδ T cells. RA binds the (RARα) expressed in Vγ4+ γδ T cells, reducing their response to IL-1 and IL-23 signalling and inhibiting STAT3 phosphorylation, which is required for Th17 production. modulate autoimmunity in a similar manner to mouse γδ T cells, and moreover, if this activity can also be modulated by RA treatment. Furthermore, as IL–17–producing Vγ4+ γδ T cells have been reported to promote tumour growth,15 the potential to manipulate these cells in other diseases such as cancer deserves further investigation. In summary, the study by Raverdeau et al. 3 shows that RA can modulate the pathogenic activity of γδ T cells in EAE, the mouse model of MS, and that this is a key mechanism underlying RA-mediated inhibition of EAE. It highlights the unique role that γδ T cells have in the immune system and the therapeutic potential of targeting these cells. If this also applies to MS in humans, this work opens up new therapeutic possibilities for treating this devastating autoimmune disease. Additionally, the possibility that a similar mechanism might underpin other IL-17-mediated diseases, such as psoriasis, colitis and even cancer, suggests even broader immunotherapeutic potential that will be important to investigate in future studies. CONFLICT OF INTEREST The authors declare no conflict of interest. Immunology and Cell Biology ACKNOWLEDGEMENTS The authors of this commentary are supported by research grants from the National Health and Medical Research Council of Australia (NHMRC) and the Australian Research Council (ARC). 8 9 10 1 Godfrey DI, Uldrich AP, McCluskey J, Rossjohn J, Moody DB. The burgeoning family of unconventional T cells. Nat Immunol 2015; 16: 1114–1123. 2 Vantourout P, Hayday A. Six-of-the-best: unique contributions of gammadelta T cells to immunology. Nat Rev Immunol 2013; 13: 88–100. 3 Raverdeau M, Breen CJ, Misiak A, Mills KH. Retinoic acid suppresses IL-17 production and pathogenic activity of γδ T cells in CNS autoimmunity. Immunol Cell Biol 2016; 94: 763–773. 4 Park H, Li Z, Yang XO, Chang SH, Nurieva R, Wang YH et al. A distinct lineage of CD4 T cells regulates tissue inflammation by producing interleukin 17. Nat Immunol 2005; 6: 1133–1141. 5 Petermann F, Rothhammer V, Claussen MC, Haas JD, Blanco LR, Heink S et al. gammadelta T cells enhance autoimmunity by restraining regulatory T cell responses via an interleukin-23-dependent mechanism. Immunity 2010; 33: 351–363. 6 Sutton CE, Lalor SJ, Sweeney CM, Brereton CF, Lavelle EC, Mills KH. Interleukin-1 and IL-23 induce innate IL-17 production from gammadelta T cells, amplifying Th17 responses and autoimmunity. Immunity 2009; 31: 331–341. 7 Mucida D, Park Y, Kim G, Turovskaya O, Scott I, Kronenberg M et al. Reciprocal TH17 and regulatory 11 12 13 14 15 T cell differentiation mediated by retinoic acid. Science 2007; 317: 256–260. Raverdeau M, Mills KH. Modulation of T cell and innate immune responses by retinoic Acid. J Immunol 2014; 192: 2953–2958. Fletcher JM, Lalor SJ, Sweeney CM, Tubridy N, Mills KH. T cells in multiple sclerosis and experimental autoimmune encephalomyelitis. Clin Exp Immunol 2010; 162: 1–11. Jamshidian A, Shaygannejad V, Pourazar A, Zarkesh-Esfahani SH, Gharagozloo M. Biased Treg/ Th17 balance away from regulatory toward inflammatory phenotype in relapsed multiple sclerosis and its correlation with severity of symptoms. J Neuroimmunol 2013; 262: 106–112. Yang XO, Panopoulos AD, Nurieva R, Chang SH, Wang D, Watowich SS et al. STAT3 regulates cytokinemediated generation of inflammatory helper T cells. J Biol Chem 2007; 282: 9358–9363. Sonnenberg GF, Artis D. Innate lymphoid cells in the initiation, regulation and resolution of inflammation. Nat Med 2015; 21: 698–708. Moline-Velazquez V, Ortega MC, Vila del Sol V, Melero-Jerez C, de Castro F, Clemente D. The synthetic retinoid Am80 delays recovery in a model of multiple sclerosis by modulating myeloid-derived suppressor cell fate and viability. Neurobiol Dis 2014; 67: 149–164. Selmaj K, Brosnan CF, Raine CS. Colocalization of lymphocytes bearing gamma delta T-cell receptor and heat shock protein hsp65+ oligodendrocytes in multiple sclerosis. Proc Natl Acad Sci USA 1991; 88: 6452–6456. Ma S, Cheng Q, Cai Y, Gong H, Wu Y, Yu X et al. IL-17A produced by gammadelta T cells promotes tumor growth in hepatocellular carcinoma. Cancer Res 2014; 74: 1969–1982.