Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Electrocardiography wikipedia , lookup
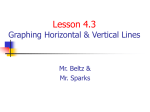
Journal of the American College of Cardiology 2013 by the American College of Cardiology Foundation Published by Elsevier Inc. Vol. 62, No. 10, 2013 ISSN 0735-1097/$36.00 http://dx.doi.org/10.1016/j.jacc.2013.05.054 STATE-OF-THE-ART PAPER What Do We Know About the “Malignant Form” of Early Repolarization? Arnon Adler, MD, Raphael Rosso, MD, Dana Viskin, Amir Halkin, MD, Sami Viskin, MD Tel Aviv, Israel There is an urgent need to identify electrocardiographic characteristics that differentiate the “benign early repolarization pattern” from “malignant early repolarization.” In a previous paper, we considered the different electrocardiographic elements of the early repolarization pattern and analyzed how they confer important prognostic information. In the present article, we review more recent information regarding the importance of the contour of the ST segment, with special emphasis on the currently termed malignant form and its value for risk stratification in early repolarization. (J Am Coll Cardiol 2013;62:863–8) ª 2013 by the American College of Cardiology Foundation There is an urgent need to identify electrocardiogram (ECG) characteristics that differentiate the “benign early repolarization” (ER) pattern from “malignant early repolarization” (1,2). Whereas the former ECG pattern is frequently observed in healthy personsdparticularly young, male (3–5), athletic (6,7), and of African-American origin (4,8)dthe latter is clearly associated with idiopathic ventricular fibrillation (VF) in case-control studies (9,10), and with increased mortality (presumably from myocardial ischemia-related arrhythmias) in population-based studies (11–13). In previous papers, we considered the ongoing debates between basic scientists and clinical cardiologists regarding the actual pathophysiology of early repolarization (14,15), and we analyzed in detail the different ECG elements of the ER pattern and discussed how they are likely to confer prognostic information (2). In brief, ER consists of 2 components: prominent J waves and ST-segment elevation. Whereas a prominent J-wave is the noticeable finding in idiopathic VF, often increasing in amplitude just before arrhythmia onset (9,16,17), ST-segment elevation is the feature emphasized in reports of benign ER (2). The importance of the J wave notwithstanding, in the present article we review more recent information regarding the importance of the contour of the ST-segment, with emphasis on the currently termed malignant form and its value for risk stratification in ER. From the Tel Aviv Medical Center and Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel. The authors have reported they have no relationships relevant to the contents of this paper to disclose. Manuscript received April 26, 2013; accepted May 22, 2013. Historical Aspects: Evolution of Concept of Malignant (Horizontal) Versus Benign (Rapidly Ascending) ST-Segment Morphology Tikkanen et al. (6) were the first to focus on the contour of the ST-segment in ER. To define a benign form, Tikkanen et al. (6) initially studied 2 populations of healthy athletes, knowing that ER is particularly frequent in this group who generally enjoys an excellent prognosis. He found that the vast majority of healthy athletes with ER (85% in 1 series and 96% in the other) had a “rapidly ascending” ST-segment blending with the T-wave (Fig. 1A). They naturally assumed this rapidly ascending form to be benign. The remaining minority of athletes with ER features an STsegment that remains flat, horizontal, or even descends toward the T-wave (Fig. 1B). This “horizontal/descending” pattern drew Tikkanen’s suspicion to a “potentially malignant” variant of ER. He tested that hypothesis by reanalyzing data from his landmark population study, which had already demonstrated a highly significant association between the presence of ER on the baseline electrocardiogram and arrhythmic mortality during long-term follow-up (Fig. 2A) (11). Indeed, the association between ER and increased arrhythmic death risk was found to be restricted to persons with the horizontal pattern (Fig. 2B), whereas the prognosis of persons with a rapidly ascending ST-segment was similar to that of persons without ER (6) (see population studies section in following text). Our interest in the horizontal versus rapidly ascending classification by Tikkanen arose from a figure from a previously published article by Cappato et al. (18) (reproduced here as Figs. 1C and 1D). The study by Cappato et al. (18) was at odds with the accepted notion that ER in athletes is invariably benign. In this case-control series, ER was more prevalent among athletes with unexplained sudden death 864 Adler et al. Malignant Form of Early Repolarization than in a control group of healthy athletes (18). The study has been criticized because the incidence ECG = electrocardiogram of ER in the control group was ER = early repolarization lower than that observed in larger MI = myocardial infarction series of healthy athletes (1). The VF = ventricular fibrillation intriguing aspect of the article, however, was that the original figure showed 2 ECGs, 1 of a healthy athlete and 1 of an athlete who eventually died suddenly. That figure (Figs. 1C and 1D) shows that the healthy athlete with ER had a rapidly ascending ST-segment, whereas the athlete with cardiac arrest had the horizontal pattern. Obviously, no conclusions can be drawn from the ECGs of 2 persons; nevertheless, it was intriguing that this figure (Figs. 1C and 1D) was published before Tikkanen recognized the prognostic value of the ST-segment morphology in adults with ER. With this in mind, we reanalyzed our original case-control series of idiopathic VF (10) and found that the association between ER and cardiac arrest was related to the fact that idiopathic VF patients with J waves mostly had a horizontal ST-segment, whereas healthy controls had primarily the rapidly ascending type (Fig. 3) (19). Soon, additional studies on ER began reporting the prognostic impact of the ST-segment morphology. Most of these studies used the definition proposed by Tikkanen and associates (6), allowing for legitimate comparisons across studies. As often happens in medicine, the emerging picture is less straightforward but very interesting. The evolving story is presented herein, covering the various forms of ER, from the most benign type, observed in healthy athletes, to the most malignant pattern found in idiopathic VF (Fig. 4). Early repolarization in athletes. Abundant data demonstrate that early repolarization is very common among young athletes (1). Indeed, both the prevalence and magnitude of ER in athletes increase as their training intensifies (7). Four recent studies (6,7,10,18) provide data on ST-segment morphology in 1,930 athletes. In these studies, the percentage of athletes with ER ranged from 23% to 44%. Yet, in all but 1 study (18), the vast majority of unselected athletes with ER had the rapidly ascending pattern and <5% had ER with a horizontal ST-segment (Fig. 4). Only 1 of the latter studies included athletes with malignant ventricular arrhythmias. This already alluded to study by Cappato et al. (18) compared 21 athletes who sustained a “cardiac arrest of unclear etiology despite extensive evaluation” to >300 healthy athletes. In this retrospective case series, athletes with ER with no ST-segment elevation (which is the equivalent of ER with horizontal ST-segment in the Tikkanen classification [6]) were 11 times more likely to have a cardiac arrest (18). Population-based studies. Six studies (5,6,19–22) provide data on the ST-segment morphology of 21,577 non-athlete adults (Fig. 4). Here, the incidence of ER ranged from 5% to 13%. Three of these studies were large population-based studies involving thousands of adults (mean age z46 years) (6,20,22). In these studies, the malignant form of ER was JACC Vol. 62, No. 10, 2013 September 3, 2013:863–8 Abbreviations and Acronyms Figure 1 Electrocardiographic Examples of ER (Top panel) Examples of early repolarization (ER) with (A) rapidly ascending and (B) horizontal ST segment as presented in the landmark study by Tikkanen et al. (6). Only the horizontal form (B) was associated with increased arrhythmic mortality during long-term follow-up. (Middle panel) The 2 electrocardiograms (ECGs) presented in the study by Cappato et al. (18) associating early repolarization with unexplained arrhythmic death in athletes: the ECG on the left (C) is from a healthy athlete; the ECG on the right (D) is from an athlete who eventually died suddenly. Note the J waves (arrows) and the ST-segment that is ascending in the healthy athlete and horizontal in the athlete with cardiac arrest. (Lower panel) The ECG (E) and activation-recovery sequence mapping performed with noninvasive computerized electrocardiographic imaging (F, G) in a 55-year-old man with idiopathic ventricular fibrillation (VF) as published by Ghosh et al. (34). (E) Note the J waves (arrows) and the horizontal ST-segment, best seen in aVF. The electrocardiographic imaging map was performed in sinus rhythm. (F) The sequence of activation (depolarization) smoothly propagates from relatively early (green) to relatively late (blue). (G) The sequence of repolarization (activation recovery intervals) during sinus rhythm. Abnormal repolarization gradients are created because zones of very early repolarization (red) are contiguous to area of later repolarization (blue). LA ¼ left atrium; LAO ¼ left anterior oblique; LPO ¼ left posterior oblique; RA = right atrium; RAO ¼ right anterior oblique. actually the most prevalent: 4% to 9% of unselected adults had ER with horizontal ST-segment whereas only 2% to 5% had ER of the benign ascending type (Fig. 4) (6,20,22). Furthermore, restricting this analysis only to adults with ER shows that the majority of them (65% to 73%) had their J waves followed by a horizontal ST-segment. At first glance, the predominance of the horizontal ST-segment among adults appears to contradict its malignant attribute. JACC Vol. 62, No. 10, 2013 September 3, 2013:863–8 Figure 2 Adler et al. Malignant Form of Early Repolarization 865 Kaplan-Meier Survival Curves for Arrhythmic Death (A) Kaplan-Meier survival curves for arrhythmic death among adults with early repolarization (ER) (red curve) and without ER (blue curve) in their baseline electrocardiogram (ECG) as reported by Tikkanen et al. (11). (B) A subsequent analysis of the same data demonstrates that the association between ER at baseline with increased mortality during long-term follow-up is due to a strong association between ER with horizontal ST segment (dotted line) and arrhythmic death (6). The arrhythmic mortality rate of persons with ER of the ascending type (dashed line) is like that of persons without ER (solid line). However, 2 of these studies (6,20) also correlated the pattern of ER with long-term outcome, and in both, the presence of malignant (horizontal) ST-segment was associated with a worse prognosis. First, in the study by Tikkanen et al. (6), subjects with ER had a higher risk for sudden death only if their ST-segment was horizontal; for such patients the risk of arrhythmic death was 1.42-fold higher (1.7-fold higher if the horizontal ER was recorded in the inferior leads) (6). In the more recent study by Rollin et al. (20) the presence of ER in the inferior leads was associated with an almost 5-fold higher risk for cardiovascular mortality, and the risk was 7-fold higher when ER was followed by the horizontal ST-segment pattern (20). The highest risk (hazard ratio: 8.7, 95% confidence interval: 3.5 to 22) was observed for persons with ER of the “notched” type followed by horizontal ST-segment (20). A third study retrospectively analyzing a hospital database (in which 15% of patients had established coronary artery disease) did not report the Figure 3 Distribution of Patients With ER Distribution of patients with early repolarization (ER) in our original case-control series (comparing patients with idiopathic ventricular fibrillation [VF] to matched controls and healthy athletes) (10) according to the morphology of their ST segment (19). The predominant form of early repolarization in the idiopathic VF group is the horizontal form (black bars); the predominant form in the 2 control groups is the ascending form (gray bars), more so in the athletes’ group. incidence of ER but did report the partition of the latter into ascending versus horizontal (23). In this study, the predominant form of ER (77%) was the rapidly ascending pattern. Again, only ER with horizontal ST-segment (present in 23% of patients with ER) was associated with increased mortality (hazard ratio: 1.75) (23). Given the age of the patients reported in these studies, both at the time of inclusion and, more importantly, at the time of survival curves divergencedsometime 20 years after inclusion in the study (6)dwe speculated 2 years ago (1) that adult patients with ER have an underlying increase in dispersion of myocardial repolarization that places them at higher risk for having VF during acute myocardial infarction (MI). Several recent studies support that hypothesis (see following text). Early repolarization and coronary disease. Three recent studies (24–26) suggest that patients who have ER are at increased risk for having ischemic VF. First, Naruse et al. (24) described 220 consecutive patients who presented with a first MI and had a previous (pre-morbid) ECG for analysis. As expected from previous studies (27), shorter duration of symptoms and higher Killip class at presentation correlated with higher risk for VF. However, the strongest independent predictor of VF on multivariate analysis (odds ratio: 7) was an ER pattern recorded before the ischemic event (24). The risk was even greater when the pre-morbid ECG showed ER with horizontal ST-segment in the inferior leads (odds ratio: 8; 95% confidence interval: 2 to 30). Conversely, ER with an ascending ST-segment did not confer additional risk from that predicted by clinical features (24). In the second study (26), 30 patients with a first MI complicated by primary VF were compared to 30 age- and sex-matched patients with a first uncomplicated MI (26). On the ECG performed 5 days after MI, ER was significantly more frequently observed among the 30 VF cases compared with the 30 controls (14 [47%] vs. 4 [3%], p ¼ 0.05). All 14 patients with VF, and also 866 Figure 4 Adler et al. Malignant Form of Early Repolarization JACC Vol. 62, No. 10, 2013 September 3, 2013:863–8 Incidence of ER Incidence of early repolarization (ER) with rapidly ascending ST-segment (blue bars) and with horizontal ST segment (red bars) in different populations. The numbers in parentheses represent the number of patients included in each study. *Only 107 of 151 ER-positive electrocardiograms (ECGs) were available for ST-segment morphology evaluation, and values in the figure were estimated based on the available data. **Definition of ascending ST-segment was in accordance with the Tikkanen et al. (6) study (>0.1 mV elevation of the ST-segment within 100 ms after the J point or a persistently elevated ST-segment of 0.1 mV throughout the ST-segment) for all studies in the figure except for Cappato et al. (>0.05 mV above baseline) (18) and Noseworthy et al. (visual analysis without cutoffs) (7). MI ¼ myocardial infarction; SCD ¼ sudden cardiac death; VF ¼ ventricular fibrillation. 3 of the 4 patients with uncomplicated infarction, had the horizontal pattern (26). The third and largest study on this issue compared 432 victims of out-of-hospital sudden death (believed to be due to a fatal arrhythmogenic MI), with 532 patients with a nonfatal MI (25). Clinical correlates of a fatal arrhythmic outcome were male sex, younger age, lower body mass index, current smoking status, and nonuse of beta-blockers and other cardiac medications, whereas a history of prior angina or prior MI actually correlated with a nonfatal outcome (25). The presence of ER on a pre-morbid ECG strongly correlated with a fatal outcome even after adjusting for gender and age (25). Specifically, the ER pattern with a horizontal ST segment (but not with an ascending pattern) was an independent predictor of sudden death (odds ratio: 2.15, 95% confidence interval: 1.20 to 3.85) (25). The ER has also been linked to higher cardiac death and arrhythmic death rates in vasospastic angina (28). Of 281 consecutive patients with documented vasospastic angina, 60 (21%) had ER during a remote ECG (recorded before or long after the ischemic event). Subjects with ER and horizontal ST-segment had a higher age- and sex-adjusted risk for cardiac events (mainly arrhythmic death) with a hazard ratio of 8. In contrast, persons with the ascending type of ER did not have an increased risk for arrhythmic events during coronary spasm induced myocardial ischemia (28). Idiopathic VF. We recently reviewed all published reports that have ECG illustrations of idiopathic VF and found 89 ECG traces with ER. In accordance with our own experience (see following text), in 70 (78%) of cases with malignant ER, the ST-segment was horizontal (D. Viskin, unpublished data). In our own case-control series of idiopathic VF, ER was more prevalent among patients with idiopathic VF than among age- and sex-matched controls (42% vs. 13%, p < 0.001) or among young athletes (42% vs. 22%, p ¼ 0.013) (10). Moreover, while the horizontal pattern was the predominant form in idiopathic VF (68% idiopathic VF patients with J waves had an horizontal ST-segment), the vast majority of healthy controls with ER had an ST-segment of the rapidly ascending type, and this was particularly true for the young athletes control group (Fig. 3) (19). Two subsequent case-control studies comparing survivors of unexplained cardiac arrest (presumed to have idiopathic VF) to age- and sex-matched controls (21,29) support our observations. In the first study, 5 (20%) of 25 cardiac arrest survivors but only 2 (3%) of 60 controls, had ER with horizontal ST-segment (p ¼ 0.02) (21). In fact, all the patients with presumed idiopathic VF who had ER had the horizontal pattern (21). The second study did not provide data on ST-segment morphology for the control group but did report that 9 of 10 cases with idiopathic VF and ER demonstrated the horizontal ST-segment pattern (29). The Emerging Story: What Do We Know About Early Repolarization Figure 4 demonstrates that the morphology of the STsegment in ER varies across the sudden death risk spectrum. Adler et al. Malignant Form of Early Repolarization JACC Vol. 62, No. 10, 2013 September 3, 2013:863–8 The predominant ST-segment pattern gradually changes from “ascending” (in blue) in the lowest risk group to “horizontal” (in red) in the highest risk group. Important limitations of the data presented in this figure should be noted. First, the studies portrayed in Figure 4 differ greatly from each other by design and population size, ranging from population-based studies of thousands of patients to case-control series of <50 (Fig. 4). Second, classification of the ST-segment is not always straightforward, mainly because the ST-segment may be horizontal in some leads and ascending in others. In such cases, we have adopted a “worst-case scenario” approach and have labeled such ECGs as horizontal (19); however, this was an empiric decision not necessarily followed by others. By definition (6), a rapidly ascending ST-segment rises to >0.1 mV within 100 ms or remains elevated >0.1 mV throughout the STsegment; yet it remains to be defined if the prognostic significance of this elevated but not ascending subtype is comparable to that of the truly ascending type. Also, in some patients, the ST-segment rises but at a slower rate. and it is not clear how this slowly ascending ST segment type should be classified. Conversely, idiopathic VF has been linked to the congenital short QT syndrome (30) and patients with symptomatic short QT often have ER (31). The combination of very short QT and ER will inevitably prevent a horizontal ST segment despite a high risk for VF. In all frankness, it is not at all clear whether the horizontal pattern and the rapidly ascending pattern represent 2 truly different forms of ER or whether they represent a continuum. Above all, the heated debate between leading basic electrophysiologists (32) and authorities in clinical electrocardiography (33) concerning the true nature of ER is yet to be resolved. Specifically, some argue that the premature and heterogeneous repolarization of the action potential at different myocardial levels, demonstrated clearly in the laboratory (32), is not necessarily the ECG feature long termed “ER.” In this regard, it is important to focus on the patient presented in Figures 1E and 1F. These traces (reproduced from Ghosh et al. [34]) are from a cardiac arrest survivor with a clinical diagnosis of malignant ER (9), who has the ECG features of ER with horizontal ST-segment (best appreciated in lead aVF in Fig. 1E) and also has intracardiac evidence of premature repolarization recorded from the epicardial surface with noninvasive electrocardiographic imaging (note the very short activation-recovery intervals in nearby sites of normal repolarization in Fig. 1F) (34). Finally, the increased risk associated with the horizontal pattern of ER demonstrated by Figure 4 should be put into the proper perspective. It is of key importance that the terms malignant and benign ER commonly used nowadays be viewed as relative terms. In other words, although careful analysis of the ST-segment morphology is useful for risk stratification, the added value is generally not sufficient for clinical decision making. For example, for the asymptomatic patient with ER, an ascending ST-segment is certainly reassuring but a horizontal form should not be interpreted as 867 a sign of high risk. As explained in detail elsewhere (19), the risk of cardiac arrest due to idiopathic VF for an asymptomatic young adult with ER is only 1:3,000 even when the ST-segment is horizontal. That is far lower than the estimated VF risk in asymptomatic Brugada syndrome (z3% at 3 years) (35), a condition for which the optimal management is ardently debated (36,37). Similar arguments can be made for patients with syncope and no evidence of structural heart disease. The vast majority of young patients in this category have benign vagal syncope; only rarely, a syncopal episode with malignant characteristics may raise concerns about a condition predisposing to malignant ventricular arrhythmias. In our series, as many as 32% of cardiac arrest survivors with established idiopathic VF had the benign rapidly ascending form (19). Thus, in a patient with ER presenting with malignant syncope, a rapidly ascending STsegment cannot be automatically accepted as guaranty of an excellent prognosis. The converse is also true: a horizontal ST-segment in a patient presenting with typical vagal syncope should not necessarily be interpreted as a malignant sign. As a matter of fact, in a recent series of 160 patients with suspected benign vagal syncope, 50 (31%) had ER. Of these, the ST-segment pattern was horizontal in 8 (16%) and ascending in 42 (84%) (38); thus 5% of all patients with vagal syncope had horizontal ER (38). This is not surprising considering that, in large series of unselected adults, the predominant form of ER is actually the horizontal form (Fig. 4). Conclusions Early repolarization has long been regarded as a benign electrocardiographic phenomenon, literally, a sign of good health. It was only 13 years ago when the suspicion that ER might be proarrhythmic began to emerge from isolated case reports (39) and pioneering experimental work (40). Moreover, it has been only 5 years since the association between ER and idiopathic VF was finally established by case-control studies (9,10,41). The advances in our understanding of the pathophysiological (32) and genetic basis (recently reviewed by Antzelevitch [42]) of ER during such a short time frame have been remarkable. It is now clear that the morphology of the ST segment, within the frame context of ER, provides important diagnostic and prognostic information. This information, however, needs to be viewed in the proper perspective. Reprint requests and correspondence: Dr. Sami Viskin, Department of Cardiology, Tel Aviv Medical Center, Weizman 6, Tel Aviv 64239, Israel. E-mail: [email protected]. REFERENCES 1. Rosso R, Adler A, Halkin A, Viskin S. Risk of sudden death among young individuals with J waves and early repolarization: putting the evidence into perspective. Heart Rhythm 2011;8:923–9. 868 Adler et al. Malignant Form of Early Repolarization 2. Viskin S, Rosso R, Halkin A. Making sense of early repolarization. Heart Rhythm 2012;9:566–8. 3. Ezaki K, Nakagawa M, Taniguchi Y, et al. Gender differences in the ST segment: effect of androgen-deprivation therapy and possible role of testosterone. Circ J 2010;74:2448–54. 4. Walsh JA III, Ilkhanoff L, Soliman EZ, et al. Natural history of the early repolarization pattern in a biracial cohort: CARDIA (Coronary Artery Risk Development in Young Adults) study. J Am Coll Cardiol 2013;61:863–9. 5. Panicker GK, Manohar D, Karnad DR, Salvi V, Kothari S, Lokhandwala Y. Early repolarization and short QT interval in healthy subjects. Heart Rhythm 2012;9:1265–71. 6. Tikkanen JT, Junttila MJ, Anttonen O, et al. Early repolarization: electrocardiographic phenotypes associated with favorable long-term outcome. Circulation 2011;123:2666–73. 7. Noseworthy PA, Weiner R, Kim J, et al. Early repolarization pattern in competitive athletes: clinical correlates and the effects of exercise training. Circ Arrhythm Electrophysiol 2011;4:432–40. 8. Perez MV, Uberoi A, Jain NA, Ashley E, Turakhia MP, Froelicher V. The prognostic value of early repolarization with ST-segment elevation in African Americans. Heart Rhythm 2012;9:558–65. 9. Haissaguerre M, Derval N, Sacher F, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med 2008;358:2016–23. 10. Rosso R, Kogan E, Belhassen B, et al. J-point elevation in survivors of primary ventricular fibrillation and matched control subjects incidence and clinical significance. J Am Coll Cardiol 2008;52:1231–8. 11. Tikkanen JT, Anttonen O, Junttila MJ, et al. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med 2009;361:2529–37. 12. Haruta D, Matsuo K, Tsuneto A, et al. Incidence and prognostic value of early repolarization pattern in the 12-lead electrocardiogram. Circulation 2011;123:2931–7. 13. Sinner MF, Reinhard W, Muller M, et al. Association of early repolarization pattern on ECG with risk of cardiac and all-cause mortality: a population-based prospective cohort study (MONICA/KORA). PLoS Med 2010;7:e1000314. 14. Antzelevitch C, Yan GX, Viskin S. Rationale for the use of the terms J-wave syndromes and early repolarization. J Am Coll Cardiol 2011;57:1587–90. 15. Rosso R, Halkin A, Viskin S. J waves and early repolarization: do not confuse me with the facts! Heart Rhythm 2012;9:1603–4. 16. Haissaguerre M, Sacher F, Nogami A, et al. Characteristics of recurrent ventricular fibrillation associated with inferolateral early repolarization role of drug therapy. J Am Coll Cardiol 2009;53:612–9. 17. Aizawa Y, Sato A, Watanabe H, et al. Dynamicity of the J-wave in idiopathic ventricular fibrillation with a special reference to pause-dependent augmentation of the J-wave. J Am Coll Cardiol 2012;59:1948–53. 18. Cappato R, Furlanello F, Giovinazzo V, et al. J wave, QRS slurring, and ST elevation in athletes with cardiac arrest in the absence of heart disease: marker of risk or innocent bystander? Circ Arrhythm Electrophysiol 2010;3:305–11. 19. Rosso R, Glikson E, Belhassen B, et al. Distinguishing “benign” from “malignant early repolarization”: the value of the ST-segment morphology. Heart Rhythm 2012;9:225–9. 20. Rollin A, Maury P, Bongard V, et al. Prevalence, prognosis, and identification of the malignant form of early repolarization pattern in a population-based study. Am J Cardiol 2012;110:1302–8. 21. Kim SH, Kim do Y, Kim HJ, et al. Early repolarization with horizontal ST segment may be associated with aborted sudden cardiac arrest: a retrospective case control study. BMC Cardiovasc Disord 2012;12:122. 22. Sinner MF, Porthan K, Noseworthy PA, et al. A meta-analysis of genome-wide association studies of the electrocardiographic early repolarization pattern. Heart Rhythm 2012;9:1627–34. JACC Vol. 62, No. 10, 2013 September 3, 2013:863–8 23. Stavrakis S, Patel N, Te C, et al. Development and validation of a prognostic index for risk stratification of patients with early repolarization. Ann Noninvas Electrocardiol 2012;17:361–71. 24. Naruse Y, Tada H, Harimura Y, et al. Early repolarization is an independent predictor of occurrences of ventricular fibrillation in the very early phase of acute myocardial infarction. Circ Arrhythm Electrophysiol 2012;5:506–13. 25. Tikkanen JT, Wichmann V, Junttila MJ, et al. Association of early repolarization and sudden cardiac death during an acute coronary event. Circ Arrhythm Electrophysiol 2012;5:714–8. 26. Rudic B, Veltmann C, Kuntz E, et al. Early repolarization pattern is associated with ventricular fibrillation in patients with acute myocardial infarction. Heart Rhythm 2012;9:1295–300. 27. Gheeraert PJ, De Buyzere ML, Taeymans YM, et al. Risk factors for primary ventricular fibrillation during acute myocardial infarction: a systematic review and meta-analysis. Eur Heart J 2006;27:2499–510. 28. Oh CM, Oh J, Shin DH, et al. Early repolarization pattern predicts cardiac death and fatal arrhythmia in patients with vasospastic angina. Int J Cardiol 2013;167:1181–7. 29. Talib AK, Sato N, Asanome A, et al. Impaired ventricular repolarization dynamics in patients with early repolarization syndrome. J Cardiovasc Electrophysiol 2013;24:556–61. 30. Viskin S, Zeltser D, Ish-Shalom M, et al. Is idiopathic ventricular fibrillation a short QT syndrome? Comparison of QT intervals of patients with idiopathic ventricular fibrillation and healthy controls. Heart Rhythm 2004;1:587–91. 31. Watanabe H, Makiyama T, Koyama T, et al. High prevalence of earlyrepolarizationinshortQTsyndrome.HeartRhythm2010;7:647–52. 32. Antzelevitch C, Yan GX. J wave syndromes. Heart Rhythm 2010;7: 549–58. 33. Surawicz B, Macfarlane PW. Inappropriate and confusing electrocardiographic terms: J-wave syndromes and early repolarization. J Am Coll Cardiol 2011;57:1584–6. 34. Ghosh S, Cooper DH, Vijayakumar R, et al. Early repolarization associated with sudden death: insights from noninvasive electrocardiographic imaging. Heart Rhythm 2010;7:534–7. 35. Viskin S, Adler A, Rosso R. Brugada burden in Brugada syndrome: the way to go in risk stratification? Heart Rhythm 2013;10:1019–20. 36. Wilde AA, Viskin S. EP testing does not predict cardiac events in Brugada syndrome. Heart Rhythm 2011;8:1598–600. 37. Brugada J, Brugada R, Brugada P. Electrophysiologic testing predicts events in Brugada syndrome patients. Heart Rhythm 2011; 8:1595–7. 38. Bartczak A, Lelonek M. Early repolarization variant in syncopal patients referred to tilt testing. Pacing Clin Electrophysiol 2013;36: 456–61. 39. Kalla H, Yan GX, Marinchak R. Ventricular fibrillation in a patient with prominent J (Osborn) waves and ST segment elevation in the inferior electrocardiographic leads: a Brugada syndrome variant? J Cardiovasc Electrophysiol 2000;11:95–8. 40. Gussak I, Antzelevitch C. Early repolarization syndrome: clinical characteristics and possible cellular and ionic mechanisms. J Electrocardiol 2000;33:299–309. 41. Nam GB, Kim YH, Antzelevitch C. Augmentation of J waves and electrical storms in patients with early repolarization. N Engl J Med 2008;358:2078–9. 42. Antzelevitch C. Genetic, molecular and cellular mechanisms underlying the J wave syndromes. Circ J 2012;76:1054–65. Key Words: athletes - early repolarization - ventricular fibrillation.