Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
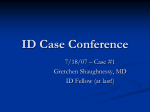
T i n s A M E R I C A N .IOUKNAL O F C L I N I C A L PATHOLOGY Vol. 40, N o . 1, p p . 21-33 J u l y , 1063 C o p y r i g h t © 11)63 b y T h e Williams & Wilkins C o . Printed in U.S.A. THE PATHOGENETIC SPECTRUM OF ASPERGILLOSIS JOHN H. SEABURY, M.D., AND MONROE SAMUELS, M.D. Louisiana State University School of Medicine, and Charity Hospital of Louisiana, New Orleans, Louisiana and secondary varieties may appear obviously satisfactory to the clinician. For example, aspergillosis may be called primary "in the absence of underlying disease or other predisposing factors," 2 and secondary aspergillosis is "associated with a local process, debilitating illness, impaired host defenses, or complicating antibacterial and/or steroid hormone therapy." 2 Is such a classification biologically defensible? Classification into primary or secondary infections on the basis of the presence or absence of an antecedent disorder is not valid in the light of present knowledge concerning pathogenesis. Despite our expanding knowledge about host factors that may favor infection, we are usually ignorant of which ones may be operational in the natural occurrence of human disease. We speak of "resistance"—of various types—and even "local immunity" to explain the infrequency with which some people are infected even under epidemic conditions. We know that local tissue injury, from any cause, favors localization of infection at the injured site, but does not necessarily explain infection in the first place. We know that organisms may enter and circulate in the blood stream without producing any recognizable evidence of disease. It is recognized that tuberculosis and many fungous infections are more common among diabetics than nondiabetics, yet we believe that this increased susceptibility to infection is not sufficient to justify classifying tuberculosis as secondary when it occurs in a diabetic. In considering disease produced by facultative parasites, the dividing line between saprophyte and parasite is often narrow and may be undiscernible under present limitations of knowledge. The relationship is not firm, by definition, and may be altered by recognized or unrecognized changes in host or microorganism. Disease of an organ or a system predisposes to other disease. Rather than trying to express this relation- The role that aspergilli may be playing in disease is often difficult to assess. When looked for, they are frequently found growing in chronic lung abscesses,4 either loosely in the necrotic cavitary content or tightly applied to the abscess wall. Under such circumstances, the fungus appears to be leading a purely saprophytic existence, although the frequency of hemoptysis in these patients is disturbing when bronchiectasis is not demonstrated. Occasionally, an Aspergillus may penetrate the wall of the abscess and invade pericavitary lung tissue. The fungus can produce extensive pneumonitis, and cerebral metastasis may occur. In the latter situations the fungus is clearly pathogenic. Most of the fungi that produce disease in man pursue a free-living existence in nature as saprophytes. When transported to man by whatever means, they may or may not produce disease. These fungi are, therefore, ordinarily saprophytic but are facultative parasites. This is no special property of fungi, being equally true of a multiplicity of bacteria. Difficulty arises in designating fungous infections as "primary" or "secondary." "Primary" implies that the infection is either first in order or principal. "Secondary" may mean second or inferior in order of time, place, or importance. The term "secondary" is used frequently in infectious processes to designate a complicating infection or superinfection appearing after treatment of the primary infection has been initiated. Classification of fungous infections into primary Received, August 20,1962; accepted for publication, April 9,1963. Dr. Seabury is Professor of Medicine, Louisiana State University School of Medicine and Senior Visiting Physician at Charity Hospital. Dr. Samuels is Clinical Assistant Professor of Medicine and Pathology, Louisiana State University School of Medicine, and Associate Pathologist at Charity Hospital. 21 22 Vol. 40 SEABUKY AND SAMUELS ship as primary versus secondary, we prefer the term "opportunistic." We would discard the term "primary" as being unnecessary. "Opportunistic" is preferred by us to "secondary infection" with its previously described connotation because "opportunistic" is free from the etymologic implications of temporality and inferiority. It is not a new term, but has been heard with greater frequency in the past several years. It may be used without implying that either the host or microorganism has undergone changes that can be precisely defined in creating the opportunity for infection. One must remember that in a very real sense all infections are opportunistic. In an outbreak of infection by highly virulent Lancefield Group A streptococci under the most favorable conditions of crowding, there will be some persons who do not become ill in spite of adequate exposure. Exposure can be documented by culturing the organism from the nose and throat of the well persons; however, such infections are not, and never have been, graced by the term "opportunistic." The term "opportunistic infection" is clearly not concerned with those factors that bring about infection by organisms which are accepted as pathogens for the host who appears to be normal at the time of acquiring the infection. Emmons 1 has used the designation "versatile opportunists" appropriately for all fungi that have a natural free-living existence as true saprophytes but may produce disease. They are what we would call facultative parasites. The designation of these organisms as "versatile opportunists" TABLE 1 PATIENTS WITH ASPERGILLOSIS* Patient Age Sex Probable Portal of Entry F Bronchi Organs Involved Possible Predisposing Factor Species of Aspergillus yr. O. T . R. D. E. F. 50 23 24 M M 29 L. C. I t . C. 24 42 Bronchi Bronchi Bronchi M F L. J. 35| F D. P. 24f M Bronchi Paranasal sinuses (?) Mouth Paranasal sinuses Both lungs Acute myelogenous leukemia, corticoids, chloramphenicol, penicillin Bronchiectasis, penicillin, Lung abscess streptomycin, sickle cell disease Lung abscess and lung Diabetes, penicillin, streptomycin, occupation,, asthma Lung abscess and lung Diabetes, asthma, occupation Lung bullae, lung, kidneys, Boeck's sarcoid, anemia, malnutrition, penicillin, liver, spleen chloramphenicol, e r y t h romycin, prednisolone (11 days) Brain, cavernous sinus, Streptomycin, oxy t e t r a anterior clinoid process, cycline, erythromycin, optic chiasm cortisone P a r o t i d area, frontal and None ethmoid sinuses, eyelid, orbit, skull, brain (?), lung (?) Orbits, lacrimal sac, eye- None lids, face, maxillary and frontal sinuses A. fumigatus A. fumigalus A. flavas A. ?iiveus A. fumiga1'II.S A. fumigatvs A. Jlavus A. jlavus * This table summarizes the essential data from the 7 patients described. The possible predisposing factors are not listed in a sequence calculated to reflect their order of importance, f Age at onset. July 1963 23 ASPERGILLOSIS is a biologic one with reference to the organism itself rather than the host. We suggest the term "opportunistic fungous infection" to designate those mycotic infections that arise because of the presence of a major abnormal host condition which (1) predisposes statistically to the development of infection by fungi which rarely produce disease in normal man, or (2) makes possible the activation of a previously acquired mycosis that has been latent or arrested. Some of these infections are iatrogenic, as a consequence of the administration of potent therapeutic agents and the increasing use of surgical or semisurgical procedures that provide an unusual portal of entry. Opportunism is also afforded by metabolic and neoplastic diseases, as well as by prolonged debilitating illness. The most important part of the definition relates to the presence of a major abnormal host condition. Some of the fungi that rarely produce disease in normal man do produce infection in persons who seem to be normal by available clinical evaluation and laboratory testing. Both the aspergilli and some of the phycomycetes are in this category. Aspergillosis and subcutaneous phycomycosis are encountered in apparently normal persons. On the other hand, most Aspergillus infections in man arise in the presence of a major host abnormality, and this applies to mucormycosis among the phycomycoses. We have selected a small group of patients with species-identified aspergillosis to illustrate the pathogenetic spectrum of the infection insofar as it can be determined from clinical, mycologic, and pathologic studies. With this purpose in mind, the case reports that follow are reduced to those data which we believe to be pertinent to the host-parasite relationships. Essential data are listed in Table 1. R E P O R T OF CASES Case 1 0 . T., a 59-year-old woman, developed progressive weakness, left lower chest pain, and somnolence in July 1960. In August, a small furuncle appeared on the right side of the face and rapidly enlarged. A second furuncle appeared above the left eye 1 week later. She was admitted to Charity Hospital in September 1960. Laboratory study revealed a severe anemia attributable to acute myelogenous leukemia. She was treated with prednisone, prophylactic penicillin, and chloramphenicol. Chest x-rays at the time of admission and 1 week prior to death revealed no pulmonary abnormality. Physical signs of a left upper lobe pneumonia appeared 3 days before death and were confirmed by chest roentgenogram. Repeated blood, urine, and sputum cultures were negative for significant pathogens. She died on September 28, 1960. Necropsy revealed multiple nodules in the right lung. The left upper lobe was completely consolidated and contained numerous red nodules with central necrosis. Scattered nodules of a similar nature were present in the left lower lobe. Histologically, all areas were either Aspergillus lung abscess or Aspergillus pneumonia. A typical abscess about a central hyphal mass is illustrated in Figure 1. Invasion of the blood vessels was frequent. Culturally, all areas gave rise to pure cultures of Aspergillus fumigatus. This case represents an example of one of the increasingly common associations between lymphomatous and leukemic disease and aspergillosis. Although no antimetabolites or myelodepressive drugs were administered, the reticuloendothelial system was extensively altered by the leukemic process. Host factors were such that multiple antibiotics and corticoid therapy in large doses was sufficient to permit rapid invasion and growth of an opportunistic fungus which manifested no clinical evidence of its presence until 3 days prior to death. A. fumigatus was highly pathogenic in this patient, probably being the immediate cause of death. No definite portal of entry was found, and it is entirely possible that the Aspergillus did not enter the respiratory tract until a few days before death. The situation would seem to be similar to that demonstrated by Sidransky and Friedman 6 in mice treated with antibiotics and cortisone. Case 2 R. D., a 23-year-old man, first developed pneumonia at age 8. Resolution was delayed 24 SEABURY AND SAMUELS and accompanied by the production of large amounts of green sputum. Sickle cell disease was first recognized at age 12. There was a subsequent history of repeated attacks of pneumonia for which he was not hospitalized. In October 1951 he was admitted to Charity Hospital at age 23 because of right lower lobe pneumonia. He was febrile and had a leukocytosis of 26,800 per cu. mm. Treatment with sulfonamides was complicated by sickle cell crisis. In December 1954 he was readmitted with the same complaints and x-ray findings as were present in 1951. X-ray of the chest in January 1955 revealed persistence of the right lower lobe density despite treatment with penicillin and streptomycin. Numerous sputum specimens and bronchial washings were negative for mycobacteria, malignant cells, and pathogenic fungi (including aspergilli). When cavitation appeared in the area of pneumonitis, it was decided to resect the right lower lobe. The resected lobe contained a 5-cm. cavity that was filled with friable material within a firm wall. Fibrosis, bronchiectasis, and chronic bronchitis were present elsewhere in the removed lobe. A portion of the cavity and underlying lung was removed aseptically and sent in a sterile container to the laboratory. Cultures were negative for bacteria, but all gave rise to a pure strain of A. fumigatus. Histologic sections of the cavity wall and adjacent lung revealed a heavy mycelial mat lining the cavity and extending into but not beyond the cavity wall. Histologic appearance suggested that the Aspergillus was saprophytic within the abscess. Figure 2 illustrates the relation of the fungus to the abscess wall. Antibiotic administration was never prolonged and no corticoids were ever administered. We believe that this represents a bronchiectatic abscess of bacterial origin in which the saprophytic presence of an Aspergillus was related to the chronic bronchitis and bronchiectasis rather than to prolonged antibiotic treatment. Case 8 E. F., a 24-year-old man, developed diabetes mellitus in November 1951. During Vol. 40 the autumn of 1954 his diabetes became difficult to regulate, he began to lose weight, and fever developed. A chest roentgenogram revealed an area of pneumonitis and cavitation in the anterior segment of the right upper lobe. This was believed to be a lung abscess, and no specific organisms were cultured. The immediate response to treatment with penicillin was good, but he had numerous short episodes of acute respiratory infection after his discharge. Fever, productive cough, and right anterior chest pain recurred in August 1955. Chest x-rays revealed the same abscess cavity in the anterior segment of the right upper lobe. The right upper lobe was not resected until March 1956. The abscess cavity measured 6 cm. in diameter.* The cavity communicated with an anterior segmental bronchus and its wall was composed of glistening, tough material. No fungous ball was present. Cultures from the cavity revealed a pure strain of Aspergillus flavus. Microscopic study demonstrated a mycelial mat lining the abscess cavity, with numerous extensions of the hyphae into the subjacent lung, which contained nonspecific inflammatory tissue. In our opinion, this lung abscess differs from that of Patient R. D., inasmuch as the role of the Aspergillus is not positively purely saprophytic. It is unlikely that A. flavus was responsible for the original formation of the abscess, but the fungus had penetrated beyond the abscess wall at the time of resection and the lung showed an inflammatory reaction to invasion. Poorly controlled diabetes may have contributed to the presumed transformation from saprophyte to pathogen. Inasmuch as this patient was a medical technologist with long-standing asthma, these factors may also have been important. From 1956 until 1961 this patient was completely asymptomatic except for difficulty in controlling his diabetes. In September 1961 a routine chest x-ray revealed a thin-walled cavity in the apex of the right lung. No etiology could be found. Sputums * We are indebted to Dr. Henry Ransom, Lafayette, Louisiana, for the gross pathology and tissue blocks. F I G . 1 (upper). P a t i e n t 0 . T. Acute abscess and granulation tissue in t h e lung surrounding a central hyphal mass of Aspergillus fumigatus. Hematoxylin and eosin. X 300. F I G . 2 (lower). P a t i e n t R . D . Mycelial mat of A. fumigatus lining the wall of t h e lung abscess. H y p h a l fragments can be seen in the cavitary wall, b u t did not penetrate it. Methenamine-silver. X 300. 25 26 SEABURY AND SAMUELS and bronchial washings were negative for aspergilli or other significant organisms. He had received no antibiotics. The right middle lobe and apical segment of the right lower lobe were resected. There was a very large cavity present with ropy material lying within it. The pleura was grossly thickened. A mycelial mat lined the cavity throughout. The lung inferior to the cavity was non-air-containing, and there was no visible separation between the middle lobe and apical segment of the lower lobe. Figure 3 illustrates a section taken from deep within the lung inferior to the cavity. Hyphae had penetrated well beyond the cavity, and the Aspergillus is here seen to be clearly invasive. There has been no evidence of recurrent infection in a 6-month period after surgery. We believe that his diabetes and occupation as a medical technologist were probably the principal factors providing the opportunity for Aspergillus infection; however, no definite reason for the development of this second abscess was evident clinically or bacteriologically. It might be suggested that the early parasitism evident in the sections of the first abscess was the real explanation for the development of the abscess 5 years later. It might be argued that the Aspergillus remained dormant only to become active later and invade. If this were true, the second episode would represent either "primary secondary" aspergillosis or "secondary primary" aspergillosis, depending upon one's state of confusion. Culture from the abscess and underlying right middle lobe revealed that this clearly invasive Aspergillus was Aspergillus niveus, an entirely different species. Consequently, there is no relation between the first and second episodes of aspergillosis other than the host susceptibility. We are unaware of any similar case report. Case 4 L. C , a 24-year-old man, had an abnormal survey chest x-ray in 1957. In February 1958 severe bilateral uveitis appeared and required hospitalization. The ocular findings Vol. 40 were regarded as compatible with Boeck's sarcoidosis, and bilateral pulmonary infiltration was present. Skin tests for tuberculosis and fungi were negative. Numerous sputum cultures were negative. Axillary lymph node biopsy revealed reactive hyperplasia with a small granuloma containing giant cells. No specific diagnosis could be made. His uveitis responded to topical corticoids, but relapsed when they were discontinued. Cough and blood-streaked sputum developed in May 1959, and were followed by chills, fever, night sweats, and weight loss. Sputum cultures were negative for Mycobacterium tuberculosis, significant pyogens, and all fungi other than Candida. Skin tests for fungi and tuberculosis were again negative. He became afebrile during 11 days of treatment with prednisolone and was then discharged. Symptoms recurred almost immediately and became progressive. He was readmitted to Charity Hospital on August 19, 1959. Chest x-rays revealed bilateral peripheral cystic changes with pericystic infiltration. Hilar lymphadenopathy was obvious. He was emaciated and anemic. Sputum cultures were repeatedly positive for hemolytic Micrococcus aureus, which was thought to be the primary cause of his fever. Candida was still present in the sputum. Complement-fixation studies at this time were positive for histoplasmosis in a dilution of 1:64. Treatment with penicillin, chloramphenicol, and erythromycin did not alter his clinical course. Drill biopsy of the lung, entering one of the peripheral cysts, revealed a non-specific granulomatous reaction, and A. fumigatus was isolated by culture of the biopsy material. He died on October 6, 1959. Necropsy revealed pulmonary aspergillosis with intracavitary hemorrhage. There was miliary aspergillosis of the kidneys, liver, and spleen. The basic pulmonary infiltrate was regarded as the result of sarcoidosis, and the hilar and aortic lymph nodes were histologically compatible with Boeck's sarcoid. Necropsy cultures were positive for A. fumigatus. No histoplasma were isolated, and none was seen by means of periodic acid-Schiff stains. Figure 4 , -41 'fL F i o . 3 (upper). P a t i e n t E . F . A section of lung several centimeters inferior to the cavity in the middle lobe. H y p h a e of Aspergillus niveus are numerous. Methenamine-silver. X 450. F i o . 4 (lower). P a t i e n t L. C. Internal margin of a peripheral cystic lesion of the lung with the conidiophore, vesicle, sterigmata, and spores of Aspergillus fumigalus. Hematoxylin and eosin. X 450. 27 28 SEABURY AND SAMUELS illustrates a vesicle with conidia in a lung cyst. The administration of multiple antibiotics and a brief course of prednisolone may have been important in the pathogenesis of aspergillosis. The peripheral pulmonary bullae were typical of those seen in advanced sarcoidosis and offered considerable opportunity for infection to any organism which might have been present in the bronchial tree. If one assumes that the initial infection of the bullae with A. fumigatus was essentially a saprophytic relation, then the subsequent invasion and dissemination might reasonably be attributed to multiple antibiotic therapy, malnutrition, anemia, brief corticoid therapy, and those unknown altered host factors which may be produced by extensive sarcoidosis. Invasion of blood vessels by the hyphae of Aspergillus was evident histologically and probably related to the persistent hemoptyses. Case 5 R. C , a 42-year-old woman, developed pharyngitis, malaise, and fever of 3 weeks' duration without medication. She was then treated with penicillin for 2 days. Two days later a universal erythematous rash appeared; she became irrational and was admitted to Charity Hospital. She was semicomatose, incontinent, and completely irrational. Slight erythema of the left tympanic membrane, meningismus, and enlarged and hyperemic palatine tonsils were present. Spinal fluid was normal and blood cultures were negative. She became increasingly febrile and developed swelling of the right side of the neck. Treatment with oxytetracycline, streptomycin, and 22 days of cortisone acetate altered neither her febrile course nor her clinical deterioration. The spinal fluid was re-examined, skin and muscle biopsies were obtained, and a search made for L.E. cells. None of these studies was abnormal. She gradually became afebrile and was discharged on the 46th hospital day. Two months later she developed enlargement of the left pupil and marked loss of visual acuity, 0 . S. Left retro-orbital pain developed and increased during the following months. Papilledema was observed. Vol. 40 Readmission to the hospital for numerous studies revealed only an irregular enlargement of the left optic foramen and some slight decrease in filling of the right lateral ventricle by pneumoencephalogram. Orbital symptoms progressed and exophthalmos on the left became measurable. A carotid angiogram was normal. Orbital exploration was unrevealing. Four months later she developed motor aphasia and right hemiplegia. At the time of readmission the spinal fluid was under increased pressure, contained 6 cells per cu. mm., and manifested a paretic colloidal gold curve. Cerebral angiography revealed a block in the left internal carotid. The patient died shortly after left frontal lobectomy with excision of a brain abscess. Histologic examination revealed a granulomatous lesion of the brain, containing giant cells, multiple small abscesses in which there were numerous branching septate hyphae. A portion of one of the abscesses is illustrated in Figure 5. Multiple cultures from the brain and abscess grew out a pure strain of A. fumigatus. Necropsy revealed an additional lesion in the left parietal area with erosion of the anterior clinoid process and destruction of the optic chiasm. Aspergillus was found invading the cavernous sinus and this was believed to be the initial intracranial focus. No lesions were found in the lungs, liver, or spleen. The lesions in the brain were granulomatous and did not suggest pyogenic bacterial origin. The symptoms which prompted her initial admission to the • hospital may have been the result of a penicillin reaction. Nevertheless, the semicomatose state, incontinence, irrationality, and meningismus lead one to suspect that cerebral aspergillosis may have been present before cortisone or any broad spectrum antibiotics were administered. The clinical course suggested the cavernous sinus was involved relatively early. There was no underlying metabolic or neoplastic disease. The Aspergillus was highly pathogenic. The clinical course makes us unwilling to regard this as an opportunistic fungous infection related to either broad 7># F I G . 5 (upper). P a t i e n t R. C. Central portion of a chronic brain abscess with hyphae of Aspergillus fumiqalus in a septum of the cerebrum traversing t h e cavity of the abscess. Hematoxylin and eosin. X 300. F I G . 0 (lower). P a t i e n t L. J. Section of the right orbital mass witli septate hyphae of Aspergillus flavus surrounded by a liistologic reaction t h a t consisted chiefly of dense fibrotic tissue. Periodic acidSchiff. X 584. 29 32 SEABURY AND SAMUELS The Aspergillus seemed to behave much as in the preceding case. It was pathogenic but very slowly invasive and of low virulence. This case also illustrates the fallacy of identifying all aspergilli isolated from human tissues as A. fumigalus. DISCUSSION Species of the genus Aspergillus are very common in our general environment. The nature of their spores is admirably suited to aerial dissemination. They are common and annoying laboratory contaminants. These saprophytes are common in soil and upon vegetation of various sorts. In one way or another, man must come in contact with the aspergilli with great frequency, yet visceral aspergillosis is a relatively rare disease in man. A. fumigatus and A. niger have been recognized as potentially pathogenic to birds and mammals for many years. Unfortunately, there are many instances in which A. fumigatus or A. niger were reported as human pathogens without the tedious cultural study necessary for species identification. As medical mycology has improved, it has become evident that human pathogenicity is not restricted to A. fumigatus and A. niger. Indeed, there is one report7 of concurrent infection by 3 species of Aspergillus in a single host. A. flavus is being isolated with increasing frequency from human aspergillosis. We do not believe that this is attributable to any biologic change in A. flavus. Aspergilli found in cultures of biopsy or necropsy specimens should not be discarded as contaminants until careful microscopic study of properly prepared sections demonstrates an absence of hyphal elements morphologically compatible with these fungi. If histopathology and cultures indicate the presence of an Aspergillus, the isolate should be submitted to a competent mycologist for identification of species. If this were done routinely, it is probable that additional species of Aspergillus would be added to the list of facultative parasites. Although the aspergilli lead much the same free-living, saprophytic existence as Coccidioides and Histoplasma, they are not as restricted geographically and produce recognized human disease much less fre- Vol. 40 quently. They manifest no dimorphic adaptability to tissue existence. The aspergilli have a low order of infectivity and seem to be an excellent genus for the study of host factors permitting infection. In severely debilitated patients who may have been moribund for days, necropsy sometimes reveals aspergilli forming small abscesses with peripheral hyphal extension into air sacs or bronchioles. Fructification has been seen under these circumstances. In such patients the Aspergillus is undeniably pathogenic, but only because of the severely altered host resistance. The bacterial population in such abscesses and the occasional finding of other fungi, such as Candida, in association with the aspergilli strongly suggest that these abscesses are caused by aspiration. The statistical relation of severe diabetes to fungous infections is well known. The observations of Sheldon and Bauer 5 on cutaneous mucormycosis in rats made acutely diabetic and acidotic by alloxan are probably equally applicable to Aspergillus infection in severely diabetic man. They observed that acute alloxan diabetes with acidosis in rats inhibited the normal function of mast cells, delayed and decreased inflammatory response to the fungus, and permitted rapidly progressive and invasive fungous growth. Sidransky and Friedman 6 demonstrated beautifully the marked infectivity and virulence of inhaled A. flavus spores in cortisonized and antibiotically treated mice; this condition was entirely absent in similarly exposed normal mice. Similar experimental studies on fungous infection have been made in relation to leukemic animals and those with reticuloendothelial systems damaged by therapeutic agents used in the treatment of cancer. Our patients Avere selected to illustrate the variable relation which the common saprophyte, Aspergillus, may have to human disease. Patient 0. T. had many host factors, especially acute leukemia, permitting the invasion and rapid extension of an Aspergillus which probably did not infect until a very few days before death. Patient R. D. had a chronic lung abscess and bronchiectasis. The Aspergillus probably entered this cavity during ventilation and continued to July 1963 33 ASPERGILLOSIS pursue a purely saprophytic existence. The same basic relation probably existed initially in Patient E. F.; however, he had a disease (asthma) which promotes obstruction of the smaller airways, and distal infection. His diabetes was severe. Under these conditions, tlie saprophytic Aspergillus began to invade the lung beyond the abscess wall during his first illness and was much more invasive during the second. These 2 observations suggest that patients with cavitary lesions containing fungous balls should certainly have the lesions resected, if possible, in the presence of any major host abnormality which, in itself, would not produce death within several years. Patient L. C. had well established sarcoidosis before developing aspergillosis. Although the association of aspergillosis with Boeck's sarcoid has been previously reported,3 there is no statistical evidence at present to implicate sarcoidosis as a major host abnormality for opportunistic infection by aspergilli. It is more likely that anemia, malnutrition, multiple antibiotic therapy, and brief treatment with prednisolone were tlie factors creating the opportunity for invasion and dissemination. Patient R. C. can not be said to have had an opportunistic fungous infection. Although she received multiple antibiotics and cortisone for several weeks, the clinical and pathologic evidence suggest that infection with Aspergillus may have occurred before treatment. Progression and extension of her infection may have been augmented by drugs. Patients L. J. and D. P. were both free from any host abnormalities known to predispose to fungous infection. Mechanical factors may have been present in the case of Patient D. P. It is intriguing that in this milieu Patient L. J. harbored her disease for 17 years before succumbing to it, and Patient D. P. died from other causes after 16 years of infection. SUMMARY 1. Seven patients with culturally identified aspergillosis have been presented to illustrate some of the host-parasite relations of Aspergillus in man. 2. The aspergilli are common saprophytes which may, as they did in one of our patients, enter the human body and continue a purely saprophytic existence. 3. Aspergilli may begin their life in man as saprophytes, becoming parasitic and pathogenic if the presence of major host abnormalities creates the opportunity for invasion. 4. The aspergilli, although ordinarily saprophytic, are facultative parasites which may produce disease in man in the absence of host factors known to predispose to infection. SUMMARIO I N I N T E R L 1 N G U A 1. Es presentate septe casos de aspergillosis de identification cultural pro illustrar certes del relationes inter hospite e parasite que es characteristic de Aspergillus in le homine. 2. Le aspergillos es commun saprophytes que pote, como illos lo faceva in facto in un de nostre patientes, entrar in le corpore human e continuar un existentia purmente saprophytic. 3. Aspergillos pote comenciar lor vita in le homine como saprophytes e postea devenir parasitic e pathogene si le presentia de major anormalitates del hospite crea le opportunitate pro un invasion. 4. Le aspergillos, ben que ordinarimente saprophytic, es parasites facultative que pote causar morbiditate in le homine in le absentia de factores de hospite que cognoscitemente predispone al contraction de infectiones. REFERENCES 1. EMMONS, C. W . : T h e Jekyll-Hydes of mycology. Mycologia, 52: 669-680, I960. 2. F I N E G O L D , S. M . , W I L L , D . , AND M U R R A Y , J . F . : Aspergillosis. Am. J . Med., 27: 463-4S2, 1959. 3. FOUGNER, K . , AND G.10NE, E . : Aspergillom; ved e t tilfelle av sarcoidosis Boeck i lungene. Nord. med., 59: 303-305, 1958. 4. H I N S O N , K . F . W., M O O N , A. J . , AND P L U M M E B , N. S.: Broncho-pulmonary Thorax, 7:317-333, 1952. aspergillosis. 5. S H E L D O N , W. H . , AND B A U E R , H . : Tissue m a s t cells and acute inflammation in experimental cutaneous mucormycosis of normal, 4S/S0treated, and diabetic rats. J . Exper. Med., 112: 1069-1084, 1960. 6. SIDRANSKY, H . , AND F R I E D M A N , L . : T h e effect of cortisone and antibiotic agents on experimental pulmonary aspergillosis. Am. J . P a t h . , 35: 169-183, 1959.' 7. W E L S H , R. A., AND B U C H N E S S , J . M . : Aspergil- lus endocarditis, myocarditis, and lung a b scesses; report of a case. Am. J . Clin. P a t h . , 25: 782-786, 1955.