Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
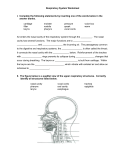
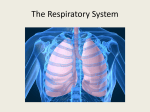
Patel D et al IJARPB: 2013, 3(4),1-10 ISSN: 2277-6222 Available online on www.ijarpb.com Review Article Received on 10/12/2013; Revised on 20/12/2013; Accepted 28/12/2013; An Overview on Respiratory System Dipal Patel*1, Komal Sharma1, C. S. Chauhan1Gunjan Jadon2 1Department of Pharmacology 2Department of Pharmaceutical Chemistry 1B.N. Institute of Pharmaceutical Science, Udaipur (Rajasthan), 313001 Shrinathji Institute of Pharmacy, Nathdwara (Raj.) 313301 E mail: [email protected] Introduction The respiratory system is the biological system of any organisms that engages in gas exchange. Even tree have respiratory systems, taking in carbon dioxide and emitting oxygen during the day, consuming carbon dioxide and producing oxygen constantly. The respiratory works with the circulatory system to deliver oxygen from the lungs to the cells and remove the carbon dioxide return it to the lungs to be exhaled. The exchange of oxygen and carbon dioxide between the airs: blood and body tissue is known as respiration. Healthy lungs take in about 1 pint of air about 12-15 times each minutes. All of the blood in the body is passed through the lungs every minute. FUNCTION OF RESPIRATORY SYSTEM The functions of the nose is to begin the process by which the air is warmed, moistened and filtered. The nose is the organ of sense. The nerve endings that detect smell are located in the roof of the nose. Passage way for food and air- The pharynx is an organ involved in both the respiratory and digestive systems air passes through. The functions of the nose are to begin the process by which the air, moistened and filtered. The nose is the organ of sense the nerve endings that detect smell are located in the roof of the nose. Passage way for food and air- The pharynx is an organ involved in both the respiratory and digestive systems: air passes through the nasal and oral sections, and food through the oral and laryngeal section. Warming and humidifying- The air is further warmed and moistened as it passes through the pharynx. Patel D et al IJARPB: 2013, 3(4),1-10 Taste- There are olfactory nerve endings of the sense of taste in the epithelium of the oral pharyngeal parts. Hearing- The auditory tube allows air to enter the middle ear. Satisfactory hearing depends on the presence of air at atmospheric pressure on each side of the tympanic membrane. Protection- The lymphatic tissue of the pharyngeal and laryngeal tonsils produces antibodies in response to antigens, e.g. microbes. 1,3,4.5,9 ANATOMY OF RESPIRATORY SYSTEM ISSN: 2277-6222 The organs of the respiratory system are Nose Pharynx Larynx Trachea Two bronchi (one bronchus to each lung) Bronchioles and smaller air passages Two lungs and their coverings, the pleura Muscles of breathing-the intercostals muscles and the diaphragm Figure A shows the location of the respiratory structures in the body. Figure B is an enlarged view of the airways, alveoli (air sacs), and capillaries (tiny blood vessels). Figure C is a closeup view of gas exchange between the capillaries and alveoli. CO2 is carbon dioxide, and O2 is oxygen. Fig- 1 Anatomy of respiratory system NOSE AND NASAL CAVITY ciliated columnar epithelium, which contains mucus-secreting goblet cell. Position and Structure Function The nasal cavity is the main route of air 1. The functions of the nose is to entry, and consists of a large irregular begin the process by which the cavity divided into two equal passages air is warmed, moistened and by a septum. The perpendicular plate of filtered. the ethmoid born and the vomer form the 2. The nose is the organ of sense. posterior bony part of the septum. The nerve endings that detect Interiorly, it consists of hyaline cartilage. smell are located in the roof of The nose is lined with very vascular the nose. Patel D et al IJARPB: 2013, 3(4),1-10 PHARYNX Position and Sturcture The pharynx is a tube 12 to 14cm long that extend from the base of skull to the level of the sixth cervical vertebra. It lies behind the nose, mouth and larynx and it’s wider at its upper end. The pharynx is divided into three parts: nasopharynx, oropharynx and laryngopharynx. The pharynx is composed of three layers of tissue: Mucous membrane lining, fibrous tissue and smooth muscles. 1. 2. 3. 4. 5. Function Passage way for food and air- The pharynx is an organ involved in both the respiratory and digestive systems: air passes through the nasal and oral sections, and food through the oral and laryngeal section. Warming and humidifying- The air is further warmed and moistened as it passes through the pharynx. Taste- There are olfactory nerve endings of the sense of taste in the epithelium of the oral pharyngeal parts. Hearing- The auditory tube allows air to enter the middle ear. Satisfactory hearing depends on the presence of air at atmospheric pressure on each side of the tympanic membrane. Protection- The lymphatic tissue of the pharyngeal and laryngeal tonsils produces antibodies in response to antigens, e.g. microbes. ISSN: 2277-6222 6. Speech- The pharynx functions in speech; by acting as a resonating chamber for sound. LARYNX Position And Structure The larynx or voice box extends from the root of the tongue and the hyoid bone to the trachea. it lies in front of the laryngopharynx at level of the third, fourth, fifth and sixth cervical vertebrae. The larynx is composed of several irregularly shaped cartilage attached to each other by ligaments and membranes. The main cartilages are1. 2. 3. 4. 1. 2. 3. 4. 5. 6. Thyroid cartilage Cricoids cartilage Arytenoids cartilages Epiglottis Function Production of sound- Sound has the properties of the pitch, volume and resonance. Pitch of the voice depends upon the length and tightness of the cords. Volume of the voice depends upon the force with which the cords vibrate. Resonance, or tone, dependent upon the shape of the mouth, the position of the tongue and the lips, the facial muscles and the air in the Para nasal sinuses. Speech- this occurs during the expiration when the tongue, cheeks and lips manipulate the sounds produced by the vocal cords. Protection of the lower respiratory tract- During swallowing the larynx moves upwards, occluding the opening into it from the pharynx and hinged epiglottis closes over the larynx. Patel D et al IJARPB: 2013, 3(4),1-10 7. Passageway for air- This is between the pharynx tracheas. 8. Humidifying, filtering and warmingThese processes continue as inspired air travels through the larynx. TRACHEA Position And Structre The trachea is a continuation of the larynx and extends downwards to about the level of the fifth thoracic vertebra where it divides at the carina into the right and left primary bronchi, one bronchus going to each lung. It is approximately 10 to 11 cm long and lies mainly in the median plane in front of the esophagus. The trachea is composed of the three layers of tissue and held open by between 16 and 20 incomplete rings of hyaline cartilage lying one above the other. The rings are incomplete posterior. Three layers of tissue clothe cartilage of trachea. 1. The outer layer consist have the fibrous and elastic tissue and encloses the cartilages. 2. The middle layer consists of the cartilages and bands of smooth muscles that bound the trachea in a helical arrangement. 3. The inner lining consists of ciliated columnar epithelium, containing mucus-secreting goblet cells. Functions 1. Support and potency- The arrangement of cartilage and elastic tissue prevent kinking and obstruction of the airway as the head and the neck moves. The cartilages prevent the collapse of trachea when the internal pressure is less then intrathoresic pressure. ISSN: 2277-6222 2. Mucociliary escalator- This is the synchronous and regular beating of the cilia of the Mucous membrane lining that wafts mucus with adherent particles upwards towards the larynx where it is either swallowed or coughed up. 3. Cough reflux- Nerve ending in the larynx, Trachea and bronchi are sensitive to irritation, which generates nerve impulses conducted by the vagus nerve to the respiratory center in the brain steam. 4. Warming, humidifying and filtering- These continue as in the nose, although air is normally saturated and body temperature when it reaches the trachea. 1,5,8 LUNGS Position And Structure In an elastic connective tissue matrix, each lobe is made up of a large number of lobules. Bronchi and Bronchioles The two primary bronchi are formed when the trachea divide, i.e. about the level of the fifth thoracic vertebra. There are two lungs, one lying on each side of the midline in the thoracic cavity. They are cone-shaped and medial surface. The apex is rounded and rises into the root of the neck, about 25 cm above the level of the middle third of the clavicle. It lies close to the first rib and the blood vessel and nerve in the root of neck. The base is concave and semi lunar in shape, and lies on the thoracic surface of the diaphragm. The costal surface convex lies against the cortical cartilage, the ribs and the intercostals muscles. The medial surface is concave has a roughly shaped area the right lung is divided into three distinct lobes: superior, Patel D et al IJARPB: 2013, 3(4),1-10 middle and inferior. The left lung is smaller because the heart occupies space left two of the midline. It is divided into only two lobes: superior and inferior. PLEURA AND PLEURAL CAVITY The pleura consist of serous membrane, which contains a small amount of serous fluid. The lung is invaginated into this sac so that it forms two layers: one adheres to the lung and other to the wall of the thoracic cavity. The pleural cavity is only a potential space. The thin film of serous fluid separates the two layers of the pleura, which allow them glide over each other, preventing friction between them during breathing. The epithelial cell of the membrane secretes the serous fluid. If either layer of pleura is punctured, the underlying lung collapses owing to its inherent properties of elastic recoil. The lungs are composed of the bronchi and smaller air passages, alveoli, connective tissue, blood vessel, lymph vessel and nerves, all embedded. The right bronchus- This is wider, shorter and more vertical then the left bronchus and is therefore more likely to become obstructed by an inhaled foreign body. It is approximately 2.5 cm long. The left bronchus- This is about 5 cm long and is narrower than the right. After entering the lung at the hilum it divide into two branches, one to each lobe. Each branch then subdivides into progressively smaller tubes within into lung substance. The bronchi are composed of the same tissues as the trachea, and are the lined with ciliated columnar epithelium. The bronchi progressively subdivide into bronchioles, terminal bronchioles, respiratory bronchioles, alveolar ducts and finally alveoli. ISSN: 2277-6222 Function 1. Control of air entry 2. Warming and humidifying 3. Support and potency 4. Removal of particulate matter 5. Cough reflux 6. Defense against microbes MUSCLES OF BREATHING The main muscle used in normal quiet breathing is the intercostals muscles and the diaphragm. Intercostals muscles There are 11 pairs of intercostals muscles that occupy the spaces between the 12 pairs of ribs. They are arranged in two layers, the external and internal intercostals muscle. The external intercostals muscle fibers: these extend downwards and forwards from the lower border of the rib above to the upper border of the rib below. The internal intercostals muscle fiber: these extend downwards and backwards from the lower border of the rib above to the upper border of the rib below, crossing the external intercostals muscle fibers at the right angle. The first rib is fixed. Therefore, when the intercostals muscle contract they pull all the other ribs towards the first rib. Because of the shape and sizes of the ribs, they move outwards when pulled upwards, enlarging the thoracic cavity. The intercostals muscles are stimulated to contract by the intercostals nerves. 1,6,10 DIAPHRAGM The diaphragm is a dome shaped muscular structure separating thoracic and abdominal cavities. It forms the floor of the thoracic cavity and the roof of the abdominal cavity. And consist of a central tendon from which muscle fibers radiate to be attached to the lower ribs and sternum and to the vertebral column by two Patel D et al IJARPB: 2013, 3(4),1-10 crura. When the muscle of the diaphragm is relaxed, the central tendon is at the level of the eighth thoracic Vertebra. When it contracts, its muscle fiber shorten and the central tendon is pulled downwards to the level of the ninth thoracic vertebra, enlarging the thoracic cavity in length. This decreases pressure in the thoracic cavity and increases it in the abdominal and pelvic cavity. The phrenic nerves supply the diaphragm. The intercostals muscles and the diaphragm contracts simultaneously, enlarging the thoracic cavity in all directions, i.e. from back to front, side to side and top to bottom.2 PHYSIOLOGY OF RESPIRATORY SYSTEM EXCHANGE OF GASES External respiration Exchange of O2 & CO2 between external environment & the cells of the body. Efficient because alveoli and capillaries have very thin walls & are very abundant (your lungs have about 300 million alveoli with a total surface area of about 75 square meters). Internal respiration - intracellular use of O2 to make ATP. Occurs by simple diffusion along partial pressure gradients. PARTIAL PRESSURE It’s the individual pressure exerted independently by a particular gas within a mixture of gasses. The air we breathe is a mixture of gasses: primarily nitrogen, oxygen, & carbon dioxide. So, the air you blow into a balloon creates pressure that causes the balloon to expand (& this pressure is generated as all the molecules of nitrogen, oxygen, & carbon ISSN: 2277-6222 dioxide move about & collide with the walls of the balloon). However, the total pressure generated by the air is due in part to nitrogen, in part to oxygen, & in part to carbon dioxide. That part of the total pressure generated by oxygen is the 'partial pressure' of oxygen, while that generated by carbon dioxide is the 'partial pressure' of carbon dioxide. A gas's partial pressure, therefore, is a measure of how much of that gas is present (e.g., in the blood or alveoli). The partial pressure exerted by each gas in a mixture equals the total pressure times the fractional composition of the gas in the mixture. So, given that total atmospheric pressure (at sea level) is about 760 mm Hg and, further, that air is about 21% oxygen, then the partial pressure of oxygen in the air is 0.21 times 760 mm Hg or 160 mm Hg. Partial pressures of o2 and co2 in the body (normal, resting conditions) Alveoli PO2 = 100 mm Hg PCO2 = 40 mm Hg Alveolar capillaries Entering the alveolar capillaries PO2 = 40 mm Hg (relatively low because this blood has just returned from the systemic circulation & has lost much of its oxygen) PCO2 = 45 mm Hg (relatively high because the blood returning from the systemic circulation has picked up carbon dioxide) Patel D et al IJARPB: 2013, 3(4),1-10 While in the alveolar capillaries, the diffusion of gasses occurs: oxygen diffuses from the alveoli into the blood & carbon dioxide from the blood into the alveoli. Leaving the alveolar capillaries PO2 = 100 mm Hg PCO2 = 40 mm Hg Blood leaving the alveolar capillaries returns to the left atrium & is pumped by the left ventricle into the systemic circulation. This blood travels through arteries & arterioles and into the systemic, or body, capillaries. As blood travels through arteries & arterioles, no gas exchange occurs. Entering the systemic capillaries PO2 = 100 mm Hg PCO2 = 40 mm Hg Body cells (resting conditions) PO2 = 40 mm Hg PCO2 = 45 mm Hg Because of the differences in partial pressures of oxygen & carbon dioxide in the systemic capillaries & the body cells, oxygen diffuses from the blood & into the cells, while carbon dioxide diffuses from the cells into the blood. Leaving the systemic capillaries PO2 = 40 mm Hg PCO2 = 45 mm Hg ISSN: 2277-6222 Blood leaving the systemic capillaries returns to the heart (right atrium) via venules & veins (and no gas exchange occurs while blood is in venues & veins). This blood is then pumped to the lungs (and the alveolar capillaries) by the right ventricle. How are oxygen & carbon dioxide transported in the blood? Oxygen is carried in blood: 1 - Bound to hemoglobin (98.5% of all oxygen in the blood) 2 - Dissolved in the plasma (1.5%) Because almost all oxygen in the blood is transported by hemoglobin, the relationship between the concentration (partial pressure) of oxygen and hemoglobin saturation (the % of hemoglobin molecules carrying oxygen) is an important one. 5 HEMOGLOBIN SATURATION Extent to which the hemoglobin in blood is combined with O2 depends on PO2 of the blood. The relationship between oxygen levels and hemoglobin saturation is indicated by the oxygen-hemoglobin dissociation (saturation) curve (in the graph above). You can see that at high partial pressures of O2 (above about 40 mm Hg), hemoglobin saturation remains rather high (typically about 75 - 80%). This rather flat section of the oxygen-hemoglobin dissociation curve is called the 'plateau.' Recall that 40 mm Hg is the typical partial pressure of oxygen in the cells of the body. Examination of the oxygen-hemoglobin dissociation curve reveals that, under resting conditions, only about 20 - 25% of hemoglobin molecules give up oxygen in the systemic capillaries. This is significant (in other words, the 'plateau' is significant) because it means that you have a substantial reserve of oxygen. In other Patel D et al IJARPB: 2013, 3(4),1-10 ISSN: 2277-6222 words, if you become more active, & your cells Factors that affect the Oxygen-Hemoglobin need more oxygen, the blood (hemoglobin Dissociation Curve molecules) has lots of oxygen to provide. When The oxygen-hemoglobin dissociation curve you do become more active, partial pressures of 'shifts' under certain conditions. These factors oxygen in your (active) cells may drop well below can cause such a shift: 40 mm Hg. A look at the oxygen-hemoglobin Lower pH dissociation curve reveals that as oxygen levels Increased temperature decline, hemoglobin saturation also declines More 2,3-diphosphoglycerate and declines precipitously. This means that the Increased levels of CO2 blood (hemoglobin) 'unloads' lots of oxygen to active cells - cells that, of course, need more oxygen.7,8 CLASSIFICATION OF DRUG Medications for Lower Respiratory Conditions Table- 4 Medications for Lower Respiratory Conditions Bronchoconstriction Mediators Cytokines, Chemokines Bronchodialation Mediators Prostaglandin’s Leukotrienes Histamine Nor epinephrine (SNS-beta) Asthma Methylxanthines (Theophylline, aminophylline, choline theophyllinate) Anticholinergics (Ipratropium, tiotropium, oxitropium) Beta2-agonists Non-selective (epinephrine) Relatively selective (albuterol, metaproteronol) Medications for Upper Respiratory Conditions Table- 5 Medications for Upper Respiratory Conditions 11 Decongestants Antihistamines 1. Pseudo- ephedrine (Sudafed) 2. Phenylpropanolamine (Contac) Sedating 1.diphen-hydramine (Benadryl) 2.chlor-pheniramine (Chlor-Trimeton) Low sedating 1.cetrizine (Zyrtec) Non sedating 2.fexofenadine (Allegra) Intra nasal steroids & cromolyn Anti-tussive Expectorant Central Acting 1. codeine 2. dextro-methorphan Local 1.Benzonatate 1.Guaifenesin 2.Bromhexine 3.Dornasealfa 4.Amonium-chloride Patel D et al IJARPB: 2013, 3(4),1-10 DISEASES & TREATMENT Common respiratory diseases treated by respiratory care physicians and other specialists include Asthma - constriction of hypersensitive airways. Chronic Obstructive Pulmonary Disease (COPD) - lung disease causing shortness of breath Chronic Bronchitis - inflammation and permanent scarring of the bronchial tube. Emphysema - damage to air sacs walls causing loss of elasticity. Pleurisy - inflammation of the pleural membrane lining lungs and the chest cavity. Lung Cancer - malignant tumors that develop in lung tissue. Acute Bronchitis-inflammation bronchial tubes. Influenza - serious infection cause by the influenza virus. Pneumonia - infection of the lungs caused by a virus or bacteria. Sinusitis - inflammation of the sinus cavities. Common Cold - infection caused by a virus. of the However, respiratory disease may involve more than lung disease, and can include a malfunction of the brain stem controlling the breathing mechanism, or disease and malfunction of the diaphragm and surrounding muscles. CONCLUSION Respiratory system is the essential body part of living beings. Disturbance of it or its organ in respect of anatomy, physiology can cause severe disease or may be death. Care in normal ISSN: 2277-6222 condition as well as disease state is necessary. Now day the various medication objects are available which protect it from any malfunctioning or disease condition. It included the various drug systems, devises and many more. REFERENCE 1. Waugh, A.; Grant, A.; “The respiratory system, In “Anatomy $Physiology in Health and Science”, Ross and Willson; 9th Edition, 240-248. 2. Chaurasia, B.D.; The Diaphragm; In “Human Anatomy”; 3rd Edition; Volume-II, 267-269. 3. Lachman, L.; Liberman, A.; Kanji, L.; Pharmaceutical Aerosols, In “The Theory Practice of Industrial rd Pharmacy”, 3 Edition; 589,590,597610. 4. Bansal, R.; Gupta, A.; Bansal, M.; “Pathophysiology of Respiratory Disorder; 1st Edition-2008-2009; Volume-I 5. Chatterjee, C.C.; Respiratory System, In “The Human Physiology”; 11th Edition Reprint 1992; 365,366,425,426. 6. Chaurasia’s, B.D.; The Lung, In “Human Anatomy”, 4th Edition; VolumeII; 267-269. 7. Chandramoulli, R.; Respiratory Physiology, In “Text Book of Physiology”; 214,235-237. 8. Glenister, T.A.; Ross, R.W.; Respiratory System. In “Anatomy and Physiology for Nurses” 3rd Edition, Page No.- 321323,338-339,342-345. 9. Rang, H.P.; Dale, M. M.; Respiratory System, In “Pharmacology”; 5th Edition-2000; 340-341. Patel D et al IJARPB: 2013, 3(4),1-10 10. Barar, F. S. K.; Drug Acting on Respiratory System, In “Essentials of Pharmacotherapeutics”; 3rd Edition2000; 530-543. 11. Geoffrey J.Laurent,Steven D.Shapironew.;“Encyclopedia for RespiratoryMedicine”. 12. Banker, G. S.; Rhodes, C. T.; Delivery of Drugs by The Pulmonary Route, In “Modern Pharmaceutics, 4th Edition, 479-490. ISSN: 2277-6222 13. Sharma, V. N.; Drugs Affecting on Respiratory System, In “Essentials of Pharmacology”;1st Edition-1999; 210. 14. Mishra, A. N.; Jain, N. K.; Advances in Pulmonary Drug Delivery, In “Advances in Controlled And Novel Drug Delivery”, 1st Edition-2001; 120127. 15. Allan R.Cook and Peter D.Dresser.; “Respiratory Disease And Disorders”.