Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychopharmacology wikipedia , lookup
Orphan drug wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Compounding wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Theralizumab wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Drug discovery wikipedia , lookup
Drug design wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacogenomics wikipedia , lookup
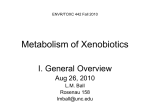
BASEL PROCEEDINGS Transport Proteins and Intestinal Metabolism P-Glycoprotein and Cytochrome P4503A Uwe Christians Abstract: Although traditionally the liver was considered the main site of pharmacokinetic drug interactions, this view has been reexamined in light of the finding that cytochrome P4503A4 (CYP3A) enzymes are expressed at high levels in mature villus tip enterocytes. Because of their topographic location in small intestinal enterocytes and their overlap in substrates, functional interactions between Pglycoprotein and CYP3A were suggested. Although the functional interaction between CYP3A and P-glycoprotein is not yet completely understood, experimental evidence suggests several mechanisms: (1) CYP3A and P-glycoprotein are coregulated via the orphan nuclear receptor SXR/PXR; (2) drugs are repeatedly taken up and pumped out of the enterocytes by P-glycoprotein, and repeated exposure to CYP3A enzymes increases the probability of a drug being metabolized; (3) P-glycoprotein keeps intracellular drug concentrations within the linear range of CYP3A enzymes; (4) metabolism results in better substrates for P-glycoprotein; and (5) metabolism shifts affinity to other intestinal efflux transporters to avoid competitive interaction of metabolites with P-glycoprotein–mediated efflux of the parent drug. Key Words: P-glycoprotein, cytochrome P4503A4, intestinal metabolism (Ther Drug Monit 2004;26:104–106) U nderstanding the interaction between drug-metabolizing enzymes and active drug transporters such as CYP3A and P-glycoprotein will significantly impact research strategies to predict human drug metabolism, intestinal absorption, and drug–drug interactions in vitro. Recently it has become evident that in the small intestine drug efflux pumps and cyctochrome P450 (CYP) enzymes, most importantly P-glycoprotein and CYP3A, form a cooperative barrier against the absorption of xenobiotics.1–3 There are Received for publication September 30, 2003; accepted December 13, 2003. From the Clinical Resarch & Development, Department of Anesthesiology, University of Colorado Health Sciences Center, Denver, Colorado. Supported by NIH grants GM 47502-10, DK065094-01, and HL071805-01. Reprints: Uwe Christians, Clinical Research & Development, Department of Anesthesiology, University of Colorado Health Sciences Center, Mailstop B-113, 4200 East Ninth Avenue, Room 2122, Denver, Colorado 80262 (e-mail: [email protected]) Copyright © 2004 by Lippincott Williams & Wilkins 104 3 levels on which P-glycoprotein and CYP3A enzymes can interact: (1) co-regulation of gene expression, (2) functional interaction, and (3) active transport of drug metabolites (see Fig. 1). The cooperative activities of P-glycoprotein and CYP3A were first suggested by their shared location in small intestinal enterocytes and the significant overlap in their substrate specificities. Coregulation was suggested by the adjacency of their genetic information as well as a significant overlap in drugs inducing their expression.4 COREGULATION OF P-GLYCOPROTEIN AND CYP3A EXPRESSION The pregnane X receptor/steroid and xenobiotic receptor (PXR/SXR) mediates induction of both CYP4503A and MDR genes, the genes responsible for P-glycoprotein expression.5,6 High intracellular free radical concentrations (eg, in diabetic patients), infectious diseases, inflammation, and immune reactions decrease the expression and activity of cytochrome P4503A4.7 Expression and activity of ATP-binding cassette transporters such as P-glycoprotein are affected the same way as cytochrome P4503A.8 Intestinal efflux pumps, such as P-glycoprotein, limit and thus regulate access of drugs to CYP enzymes and prevent CYP enzymes from being overwhelmed by the high drug concentrations in the intestine. As the drug is repeatedly transported out of the mucosa cells and then passively reabsorbed, this continuous repeated exposure leads to more efficient metabolism.2,3 Cummins et al3 studied the extraction ratios across monolayers of Caco-2 cells, a common in vitro model for studying intestinal transport, that were overexpressing CYP3A4. The study demonstrated that inhibition of Pglycoprotein-mediated efflux by the specific P-glycoprotein inhibitor GG918, although not an inhibitor of CYP3Amediated metabolism, decreased the extraction ratios and metabolism rates of dual CYP3A4/P-glycoprotein substrates. These results were recently confirmed in studies based on a rat single-pass intestinal perfusion model in vivo.2 Interestingly, in the liver the topographic relationship between CYP3A enzymes and P-glycoprotein is reversed. After entering the hepatocytes, the drug gets in contact with CYP3A enzymes first. Inhibition of P-glycoprotein without inhibition of CYP3A in a perfused rat liver model using GG918 showed that, in contrast Ther Drug Monit • Volume 26, Number 2, April 2004 Ther Drug Monit • Volume 26, Number 2, April 2004 Intestinal Transport and Metabolism FIGURE 1. Interactions between Pglycoprotein (P-gp) drug transport and cytochrome P4503A (CYP3A)– mediated drug metabolism in the gut mucosa and the effect of Pglycoprotein inhibition on intestinal drug metabolism. to the small intestine, inhibition of P-glycoprotein in the liver results in increased metabolism.2 Inhibition of the efflux of parent drug and metabolites from the hepatocyte leads to increased metabolism of both parent and metabolites as a result of prolonged exposure to drug-metabolizing enzymes. This is supported by and explains the results of a clinical study in bone-marrow transplant patients.9 In this study, graft-versushost disease (GVHD) of the liver significantly increased cyclosporine metabolite concentrations in blood with a significant shift of the metabolite pattern toward metabolites modified at multiple sites. Liver GVHD is known to affect biliary transporters before affecting drug-metabolizing enzymes. DRUG METABOLITES AND P-GLYCOPROTEIN The interaction of P-glycoprotein and metabolites generated by CYP3A was evaluated in a study assessing the formation and transport of tacrolimus metabolites in the pig intestinal mucosa in an Ussing chamber.10 Like tacrolimus, at least its main metabolite, 13-O-desmethyl tacrolimus, is a known P-glycoprotein substrate.2 When tacrolimus was added to the luminal side of the intestinal preparation, more than 90% of the metabolites were transported from the tissue back into the luminal chamber, most likely by active transport. Because the molar concentrations of tacrolimus were more than 100fold higher than the concentrations of the formed metabolites, and because it could be expected that tacrolimus would compete with the metabolites for the transporter, the results suggested that the CYP3A-mediated metabolism of tacrolimus generated metabolites that either have a higher affinity for the P-glycoprotein transporter than the parent or are substrates of a different transporter. This hypothesis is supported by an in vitro study showing that the angiotensin II antagonist losartan © 2004 Lippincott Williams & Wilkins is a P-glycoprotein substrate but that its active main metabolite EXP3174 is not.11 Rather, in Caco-2 cells EXP3174 had a higher affinity for active transporters other than P-glycoprotein. CONCLUSIONS P-glycoprotein and CYP3A in the small intestine significantly contribute to the often low oral bioavailability, pharmacokinetic variability, and drug–drug interactions of drugs that are dual P-glycoprotein/CYP3A substrates. The information about the interactive nature of P-glycoprotein and cytochrome P4503A enzymes that has recently become available will significantly impact general views on drug metabolism and regulatory guidelines.2 It is a common belief that one of the reasons for drug metabolism is to make lipophilic drugs more water soluble and therefore easier to eliminate. There is a good possibility that drug metabolism turns drugs into better substrates for transporters to facilitate their elimination. Current regulatory guidelines for in vitro drug intraction testing, such as those by the US Food and Drug Administration,12 are solely based on assays using isolated microsomes or cytochrome P450 enzymes. However, interaction with active transporters without direct interference with cytochrome P450 enzymes can alter drug metabolism.2,3 In the future, uptake and efflux must be taken into consideration when drug interactions are evaluated in vitro.2 The CYP3A/P-glycoprotein alliance was the first discovered and is currently the best studied drug-metabolizing enzyme/active drug transporter combination. It is reasonable to expect that other important metabolism enzyme/drug transporter pairs, such as UGT and MRP2, will also be of clinical relevance.2 105 Ther Drug Monit • Volume 26, Number 2, April 2004 U. Christians REFERENCES 1. Cummins CL, Jacobsen W, Benet LZ. Unmasking the dynamic interplay between intestinal P-glycoprotein and CYP3A4. J Pharmacol Exp Ther. 2002;300:1036–1045. 2. Benet LZ, Cummins CL, Wu CY. Transporter-enzyme interactions: implications for predicting drug–drug interactions from in vitro data. Curr Drug Metab. 2003;4:393–398. 3. Benet LZ, Cummins CL. The drug efflux–metabolism alliance: biochemical aspects. Adv Drug Deliv Rev. 2001;50(suppl 1):S3–S11. 4. Wacher J, Wu CY, Benet LZ. Overlapping substrate specificities and tissue distribution of cytochrome P4503A and P-glycoprotein: implications for drug delivery and cancer chemotherapy. Mol Carcinogen. 1995;13: 129–134. 5. Synold TW, Dussault I, Forman BM. The orphan nuclear receptor SXR coordinately regulates drug metabolism and efflux. Nature Med. 2001;7: 584–590. 6. Geick AW, Eichelbaum M, Burk O. Nuclear receptor response elements mediate induction of intestinal MDR1 by rifampin. J Biol Chem. 2001; 276:14581–14587. 106 7. Iber H, Sewer MB, Barclay TB, et al. Modulation of drug metabolism in infectious and inflammatory diseases. Drug Metab Rev. 1999;31:29–41. 8. Sukhai M, Piquette-Miller M. Regulation of the multidrug resistance genes by stress signals. J Pharm Pharmaceut Sci. 2000;3:268–280. 9. Christians U, Spiekermann K, Schottmann R, et al. Cyclosporin metabolite patterns in blood from patients with acute graft versus host disease after bone marrow transplantation. Bone Marrow Transplant. 1993;12: 27–33. 10. Lampen A, Christians U, Gonschior AK, et al. Metabolism of the macrolide immunosuppressant, tacrolimus, by the pig gut mucosa in the Ussing chamber. Br J Pharmacol. 1996;117:1730–1734. 11. Soldner A, Benet LZ, Mutschler E, et al. Active transport of the angiotensin-II antagonist losartan and its main metabolite EXP 3174 across MDCK-MDR1 and Caco-2 cell monolayers. Br J Pharmacol. 2000;129: 1235–1243. 12. CDER, US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research and Center for Biologics Evaluation and Research (CBER). Guidance for the Industry. Drug Metabolism/Drug Interaction Studies in the Drug Development Process: Studies In Vitro. April 1997 (www.fda.gov/cder/guidance) © 2004 Lippincott Williams & Wilkins