Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Dynamic insulation wikipedia , lookup
Underfloor heating wikipedia , lookup
R-value (insulation) wikipedia , lookup
Thermal comfort wikipedia , lookup
Intercooler wikipedia , lookup
Radiator (engine cooling) wikipedia , lookup
Solar air conditioning wikipedia , lookup
Thermal conduction wikipedia , lookup
Thermoregulation wikipedia , lookup
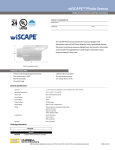
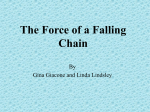
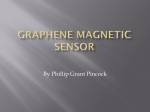
British Journal of Anaesthesia 111 (5): 768–75 (2013) Advance Access publication 25 June 2013 . doi:10.1093/bja/aet217 Temporal and spatial dispersion of human body temperature during deep hypothermia O. Opatz 1*†, T. Trippel 2†, A. Lochner 1, A. Werner1, A. Stahn 1, M. Steinach1, J. Lenk 1, H. Kuppe 3 and H. C. Gunga 1 1 Charité Centrum für Grundlagenmedizin, Institut für Physiologie, Thielallee 71, Berlin 14195, Germany Charité - Campus Virchow Klinikum, Medizinische Klinik m. S. Kardiologie, Augustenburger Platz 1, Berlin 13353, Germany 3 Deutsches Herzzentrum Berlin, Abteilung für Anästhesiologie, Augustenburger Platz 1, Berlin 13353, Germany 2 * Corresponding author. E-mail: [email protected]; [email protected] Editor’s key points † There is uncertainty as to the best site to measure the core body temperature from. † Spatial and temporal relationship of temperature measurements were investigated in patients undergoing cardiothoracic surgery. † The sensors should be placed as close as possible to the site of interest to be measured. † A non-linear relationship between sensor sites was found; contributory factors need further study. Background. Clinical temperature management remains challenging. Choosing the right sensor location to determine the core body temperature is a particular matter of academic and clinical debate. This study aimed to investigate the relationship of measured temperatures at different sites during surgery in deep hypothermic patients. Methods. In this prospective single-centre study, we studied 24 patients undergoing cardiothoracic surgery: 12 in normothermia, 3 in mild, and 9 in deep hypothermia. Temperature recordings of a non-invasive heat flux sensor at the forehead were compared with the arterial outlet temperature of a heart–lung machine, with the temperature on a conventional vesical bladder thermistor and, for patients undergoing deep hypothermia, with oesophageal temperature. Results. Using a linear model for sensor comparison, the arterial outlet sensor showed a difference among the other sensor positions between 20.54 and 21.128C. The 95% confidence interval ranged between 7.06 and 8.828C for the upper limit and 28.14 and 210.628C for the lower limit. Because of the hysteretic shape, the curves were divided into phases and fitted into a non-linear model according to time and placement of the sensors. During cooling and warming phases, a quadratic relationship could be observed among arterial, oesophageal, vesical, and cranial temperature recordings, with coefficients of determination ranging between 0.95 and 0.98 (standard errors of the estimate 0.69–1.128C). Conclusion. We suggest that measured surrogate temperatures as indices of the cerebral temperature (e.g. vesical bladder temperature) should be interpreted with respect to the temporal and spatial dispersion during cooling and rewarming phases. Keywords: body temperature; deep hypothermics circulatory arrest; intraoperative monitoring; mathematical model; non-linear model Accepted for publication: 18 March 2013 Suitable sensors and sensor placement for the correct measurement of core body temperature (CBT) have been the subject of continuous debate since the first published measurements of human body temperature by Carl Reinhold August Wunderlich.1 Thermodynamic monitoring has shown that the slopes of warming and cooling differ according to sensor location and tissue type. Thus, estimating the brain temperature or CBT, respectively, by monitoring peripheral surrogates implies knowledge about the dynamic aspects of temperature changes. To demonstrate the wide range of human body temperatures, iatrogenic hypothermia can be used as a model, as it is reversible and of considerable clinical interest as opposed to accidental hypothermia, which may result in shivering and lead to severe cardiocirculatory or coagulative complications, and tissue damage.2 3 By lowering temperature below the optimal temperature for intracellular enzymatic systems, hypothermia has been in † therapeutic use for decades to appreciably slow down cell metabolism.4 Mild hypothermia (34–378C) has been reported to ameliorate the neurological outcome after cardiopulmonary resuscitation.5 – 8 Additionally, the metabolic advantages of deep hypothermia (,308C) have been used during operations on great vessels, which require a circulatory arrest of several minutes to clear the surgical field. Thus, for accidental and also for the therapeutic use of hypothermia, an easy-to-use, reliable, and secure system for monitoring the brain temperature or CBT would be needed. However, previous reports show remarkable disparity regarding proper sensor placement and temporal interdependency.9 – 12 The current study evaluates temporal and spatial dispersion of human body core temperature in induced hypothermia, using four sites of temperature measurement. A novel cranial heat flux sensor has shown to be a reliable measure of body Shared first authorship. & The Author [2013]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: [email protected] BJA Non-linearity of physiological recordings core temperatures of patients in intensive care under normothermic conditions.13 It displayed good applicability for the determination of heat strain during exercise and has been tested under extreme environmental conditions.14 The other sites were the arterial outlet of the heart– lung machine, the vesical bladder, and the oesophagus. Thus, by correlating temperatures in normothermia, mild and deep hypothermia obtained at different sites of the human body, we aim to integrate these into a projection regarding their inter-relationship and to discuss its implications for clinical medicine. Methods Patients The following study was performed at the German Heart Institute Berlin (DHZB). All patients included in the study were recruited within 1.5 yr. All participants gave their written informed consent. We enrolled 12 patients who underwent surgery in normothermia and 12 patients who underwent surgery under hypothermic conditions (3 in moderate hypothermia and 9 in deep hypothermia). The study was designed according to the ethical statutes of the Declaration of Helsinki, Revision 6, 2008. It was approved by the Ethics Committee of the Charité – Universitätsmedizin Berlin. All patients suffered from severe cardiac diseases or abnormalities that provided an indication for surgical reconstruction (American Society of Anesthesiologists Classification, ASA IV) and received open-heart surgery. Exclusion criteria were met if a proper fixation of the cranial double sensor the Doppler/ pulse oximetry unit or both was not possible. In five of the nine deep hypothermic patients, a temporary circulatory arrest (DHCA) was needed. Body temperatures were measured at the head using a heat flux sensor, oesophageal (only in deep hypothermic patients), at the arterial outlet of the membrane oxygenator, and in the vesical bladder. Because of the fact that surgery in deep hypothermia (i.e. aortic arch aneurysm) often takes place under emergency conditions, we also studied cases of moderate hypothermia. For simplification, patients were therefore allocated to three groups depending on the extent of hypothermia (normothermia, moderate hypothermia, and deep hypothermia). To focus on the different phases of deep hypothermia, the course of each measurement was divided into five phases, namely P1–P5, representing specific periods of the cooling and rewarming processes. Experimental set-up and protocol Data were acquired during four types of surgery: aortic arch surgery (9), heart valve replacement (13), tumour extirpation (1), and pulmonary thrombectomy (1). Operations on the aortic arch frequently require temporary circulatory arrest in deep hypothermia. Thus, they provide the opportunity to record core temperatures as low as 9.3 and 13.88C (depending on the sensor position). We chose to study heart valve replacements of the aortic, the tricuspid, the mitral, or a combination of valves, because they are routine procedures on the open heart with high comparability. They were performed in normothermic patients using a cardiopulmonary bypass (CPB). Operations such as tumour extirpation or the placement of a left ventricular assist device were also performed predominantly under normothermic conditions. Transoesophageal echocardiography (TOE) was used intermittently during surgery in deep hypothermia and continuously during valve replacement surgery in mild hypothermia and normothermia. The temperature sensors were applied after the patients had been brought into the operating theatre (OT) and were positioned on the operating table. Sensors were removed after the surgeons had finished the sutures, but before the patients left the OT. Thermal management in the OT was performed according to a standardized clinical protocol. Patients were cooled and warmed using CPB. Ice packs were used on the head as an additional means of neuroprotection. The sensors were kept at a secure distance from the ice to ensure data accuracy. Sodium nitroprusside was administered by the anaesthesiologist to ensure peripheral vasodilation of the arterial and venous vascular bed and to provide a homogeneous change of the body temperature. The type of anaesthesia, other medications given, and the mode of mechanical ventilation followed a standardized clinical protocol, in accordance with the guidelines of the Society of Cardiovascular Anesthesiologists (http://www.scahq. org/ClinicalPracticeGuidelines/guideLines.html) and the European Society of Cardiology (http://www.escardio.org/guidelinessurveys/esc-guidelines/Pages/GuidelinesList.aspx). Three agents were used for induction: (i) etomidate at a dose of 0.3–0.4 mg kg21, (ii) pancuronium bromide at a dose of 0.05 –0.1 mg kg21, (iii) and sufentanil at a dose of 0.5 –1 mg kg21. For maintenance during surgery, propofol was administered at a dose of 3–6 mg kg21 h21 according to bispectral index combined with sevoflurane at an end-tidal concentration of 0.5–1.0 vol.%. For analgesia, sufentanil was administered at a dose of 0.3 –0.8 mg kg21 h21. The sevoflurane administration was stopped after the patients had been connected to CPB. Sodium nitroprusside was administered at a dose of 0.5–8 mg kg21 min21. During surgery, the following parameters were recorded: arterial pressure (invasive arterial measurement), heart rate, electrocardiogram, pulse oximetry, blood gas analysis, and blood flow. Additionally, CBT (measured by the double sensor on the forehead), capillary-venous oxygen saturation, blood flow in microcirculation, and relative amount of haemoglobin (measured by laser-doppler and tissue-spectrometry at forehead and tibia by Oxygen 2 See [O2C], LEA Medizintechnik, Giessen, Germany). Anaesthesia and CPB In order to provide an acceptable operational field, the movement of the heart and the lungs sometimes has to be stopped. Via insertions in the right atrium and the ascending aorta, all 769 BJA Opatz et al. Koralewski, Hambuhren, Germany). In our study, it was only possible to use the head sensor, because the sternum was inaccessible during open-heart surgery. The double sensor is made up of two temperature probes, T1 and T2, with an insulation disc placed between them. One probe (T1) had close contact to the skin surface and the other (T2) to the ambient environment. Both probes are within an isolative casing. Given that the heat transfer coefficients of human tissue (ht) and of the insulation disc between the probes (hs) are known and that there is no heat loss of any type, the CBT can be calculated using the following equation: blood was redirected to the CPB, was oxygenated, and reperfused into the vascular system. For operations requiring hypothermic circulatory arrest, the heart–lung machine also served as an external cooling device of the bypassed blood. In some cases, the complexity of the procedure required prolonged periods of circulatory arrest with an increased risk of neurological damage because of hypoxaemia. Although some of the patients were extubated in the ICU, our data collection ended just before they left the theatre. Temperature monitoring devices Vesical sensor Tc = T1 + For standard temperature monitoring at the German Heart Institute, a Level 1 Foley catheter (in situ) with a temperature sensor (thermistor: equivalent to YSI 400 series, Smiths Medical International Ltd, Ashford, Kent, UK) was used. The catheter was inserted before the operation and not removed until the patient was in a stable clinical condition, usually 2–3 days after operation. hs (T1 − T2 ) ht where Tc is core temperature, T1 skin-side probe of the double sensor, T2 ambient-side of double sensor probe facing away from skin, hs heat transfer coefficient of the double sensor and ht heat transfer coefficient of human tissue. In the further development of the double sensor, lateral heat loss and also possible changes in the ambient temperature were taken into consideration. Further details are given in Gunga and colleagues.14 15 The sensor was applied using a two-sided adhesive ring tape and also an additional adhesive tape to securely fix it to the skin on the lateral forehead. Combined skin and heat flux sensor (double sensor) To measure CBTat the head, a novel heat flux sensor developed by Draeger was used (Fig. 1). It records CBT using cranial or sternal sensors every 2 s. Data were sampled and recorded using a wearable data logger system (Health Lab-System, Tsa Tamb hsa hiso T2 Qloss hs As Inner insulation Qloss Qs Outer insulation T1 Skin Qt Tissue ht Tc Fig 1 Principle of the heat flux double sensor. Tc is calculated by measuring the heat flux dQ/dt from the body core to the outer sensor T2. Heat loss (Qloss) is taken into account. 770 BJA Non-linearity of physiological recordings Oesophageal sensor CPB was performed using the Stöckert S5 made by the Sorin Group. Each of the bypass machines used an oxygenator with thermosensors at the inlet and outlet. The data at the bypass inlets were not recorded continuously, so they were not used for evaluation. outliers, and differences of .108C were considered artifacts; 155 outliers (2.9%) were removed. Scatter plots and correlation analysis were used to examine the relationship among temperature-recording sites. The CCC was computed as described by Lin16 17 to obtain a measure of association that includes a correction factor, which indicates how far the regression line deviates from the line of identity. Furthermore, we assessed agreement between the two methods according to Bland and Altman18 by plotting their differences against their means. Because of the non-linearity of the temperature changes, the process was divided into five phases (P1 –P5) and the cooling and rewarming periods were analysed separately. We performed a two-sided Spearman and Pearson correlation regarding the dependence of measurement error on the temperature change slope. Statistics Results Statistical analyses were performed using the SPSS statistics software, Version 19. The concordance correlation coefficient (CCC) was computed using R, Version 2.13 (http://www.rproject.org). Descriptive data are reported as means and standard deviations (SDs). Measurements were scanned for The study included 24 patients, 16 males and 8 females, with an average age of 61.7 yr (range 32–81) and average body mass index of 25.3 (range 15.2 –31.0). Overall, the four temperature sensors recorded 5275 data points. The mean temperature varied between 34.48C (SD 4.0) and 36.78C (SD 0.6) in Monitoring of oesophageal temperature was performed using a standard Mallinckrodtw medical sensor (Mon-a-ThermTM , Mallinckrodt, Inc., St Louis, MO, USA). The oesophageal sensor was placed in the distal oesophagus, at 30 cm lip level. This was confirmed by laryngoscopical inspection after intubation. Oesophageal temperature was recorded only in deep hypothermic patients, as described below. Sensor at the arterial outlet of the membrane oxygenator Fig 2 Bland –Altman plots of all sensor positions vs the arterial membrane oxygenator (AMO). Colours represent phases: P1, black; P2 (cooling), blue; P3, white; P4 (warming), red; and P5, black. The first row represents the cranial double sensor compared with the arterial outlet of the membrane oxygenator; the second represents the oesophageal sensor; and the third represents the vesical sensor. The middle horizontal line represents the average of all values, whereas the lines above and below represent the 1.96-fold SD (95% of all values). 771 BJA Opatz et al. Table 1 Linear correlations of the temperature sensors. AMO, arterial membrane oxygenator; CRAN, cranial heat flux double sensor; VES, vesical sensor; OES, oesophageal sensor; CCC, correlation concordance coefficient; SD, standard deviation; CI, confidence interval; UL, upper limit; LL, lower limit. All correlations were two-sided significant with P,0.01; all patients’ data are shown using linear correlation. The patients are split into three groups: normothermia, mild hypothermia, and deep hypothermia. AMO CRAN VES OES Deep (n¼9) Table 1 Continued AMO CRAN VES VES CCC 0.46 0.52 Pearson 0.56 0.64 1 1 BIAS 0.28 1.04 0 CI 95% UL 4.85 4.94 0 CI 95% LL 24.2868 22.8604 0 2.33 1.99 0 CCC 1 0.29 0.08 Pearson 1 0.48 0.21 BIAS 0 0.39 20.28 CI 95% UL 0 2.35 0.82 CI 95% LL 0 21.57 21.38 SD 0 1 0.56 0.12 SD OES AMO CCC 1 0.82 0.69 0.89 Normal (n¼12) Pearson 1 0.84 0.82 0.89 AMO BIAS 0 21.12 20.90 20.54 CI 95% UL 0 7.70 8.82 7.06 CI 95% LL 0 29.94 210.62 28.14 SD 0 4.50 4.96 3.88 CRAN CCC 0.82 1 0.93 0.93 Pearson 0.84 1 0.95 0.93 CRAN 1.20 1 0.21 0.33 CCC 0.29 1 CI 95% UL 11.04 0 5.20 6.52 Pearson 0.48 1 0.47 CI 95% LL 28.64 0 24.79 25.86 20.39 0 21.04 5.02 0 2.55 3.16 CI 95% UL 2.84 0 20.04 CI 95% LL 23.62 0 22.04 1.65 0 0.51 CCC 0.08 0.12 1 Pearson 0.21 0.47 1 BIAS 0.28 1.04 0 BIAS SD VES CCC 0.69 0.91 1 0.84 Pearson 0.82 0.95 1 0.95 0.90 20.21 BIAS 0 20.27 CI 95% UL 11.27 4.592 0 5.18 CI 95% LL 29.47 25.012 0 25.72 2.45 0 2.78 SD 5.29 OES BIAS SD VES CI 95% UL 3.87 3.02 0 CI 95% LL 23.31 20.94 0 1.83 1.01 0 CCC 0.89 0.93 0.84 1 SD Pearson 0.89 0.93 0.95 1 OES BIAS 0.54 20.33 0.27 0 CI 95% UL 8.63 5.56 5.39 0 CI 95% LL 27.55 26.23 24.85 0 4.13 3.01 2.61 0 CCC 1 0.53 0.46 Pearson 1 0.53 0.31 BIAS 0 0.39 20.28 CI 95% UL 0 5.15 2.82 CI 95% LL 0 24.37 23.38 SD 0 2.43 1.58 CCC 0.53 1 0.52 Pearson 0.53 1 0.64 SD OES Moderate (n¼3) AMO the normothermic group, between 33.68C (SD 2.9) and 34.18C (SD 1.98C) in the mildly hypothermic group, and between 25.38C (SD 8.6) and 27.58C (SD 8.2) in the deep hypothermic group. Of the nine deep hypothermia patients, five had a temporary circulatory arrest with an average duration of 32.8 min. It should be noted that some of the patients in the normothermic group were not within the defined limits, but were included in this category as active cooling was not a part of the surgical procedure. CRAN BIAS 20.39 0 21.04 CI 95% UL 4.71 0 1.80 CI 95% LL 25.49 0 23.88 2.60 0 1.45 SD Correlations among sensor positions, using linear and non-linear modelling Continued 772 To compare the two methods against each other, Bland–Altman plots were used as a standard analysis. Figure 2 depicts Bland– Altman plots of all sensors compared with the membrane oxygenator sensor in normothermia, mild hypothermia, and deep hypothermia. Pearson’s R and Lin’s CCC, and also the 95% confidence intervals (CIs) are reported in Table 1. BJA Non-linearity of physiological recordings Discussion 36 TCRAN (°C) 33 30 f(x)=–6.1+3.3x–0.07x2 R 2=0.99 SEE=0.52 27 24 21 f(x)=36–2x+0.05x2 R 2=0.99 SEE=0.53 18 15 12 15 18 21 24 27 30 33 36 TAMO (°C) Fig 3 Single case of a quadratic fitting of the split up process-loop. The blue line shows the cranial sensor vs the AMO during the cooling phase, whereas the red one shows the re-warming. R 2, Coefficient of determination; SEE, standard error of the estimate. Table 2 Quadratic fitting of warming and cooling phases. Mean coefficients of determination (R 2) during cooling (P2) and warming (P4) between the temperature of the arterial membrane oxygenator outlet (AMO) and cranial (CRAN), vesical (VES), and oesophageal (OES) temperature, and also the standard errors of the estimates (SEE). SDs in parentheses. P2 P4 R2 SEE R2 SEE CRAN 0.97 (0.04) 0.69 (0.55) 0.96 (0.04) 1.12 (0.56) VES 0.97 (0.05) 0.77 (0.66) 0.97 (0.07) 0.84 (0.44) OES 0.96 (0.05) 0.90 (0.68) 0.98 (0.02) 0.94 (0.47) As the relationship of measured temperatures did not appear to be linear, each patient’s data in deep hypothermia were divided into five phases, according to the cooling or warming status of the CPB. Each patient’s phase of cooling (P2) and warming (P4) was fitted separately, using a quadratic regression model as shown in Figure 3, visualizing a single case example. P2 and P4 were selected as they represent the dynamic aspect of induced hypothermia. Moreover, during P3 cardiac arrests of different durations were induced in some hypothermic patients, which changed the dissipation of temperature via the circulatory system. The non-linear correlation coefficients and the range of standard errors of both phases are given in Table 2. One significant correlation was found regarding the measurement differences of head and arterial sensor position vs the temperature change slopes (R¼0.7; P¼0.036). All other measurement errors did correlate with the speed of arterial blood temperature change. The temporal relationships of measured temperatures in different tissues of the human body display a directional or path dependency. Such hysteretic processes can be found in many technical, economic, and biological systems. They imply that the measured output is also dependent on the state of the system. Thus, they are a type of memory function of a biological process. Which parameters exactly modulate the shape of the hysteretic curves is subject to inter-individual variability and remains unclear in the current study. Thus, the time lag between sensor positions is not constant, but individual for each patient. Parkhurst19 described a hysteresis model for heat exchange in cattle during changes in environmental temperature. He states that ‘the area inside the hysteretic loop indicates the amount of work done in absorbing and dissipating heat’. Thus, the extent of inertia of temperature exchange between two locations is correlated to the width of the hysteretic loop. Under physiological conditions, the gradient among different sensor positions is also influenced by vasomotor effects. Ozaki and colleagues20 described that during anaesthesia the thermoregulatory vasomotor response is direction dependent. During operations in deep hypothermia, it should be noted that this vasomotor response might be suppressed by either anaesthetic agents or i.v. application of nitroglycerine.21 – 23 TOE can influence the measurement of oesophageal temperature. In this study, TOE measurements during deep hypothermia were carried out intermittently. During the TOE measurements, the temperature sensor stayed at its place. The TOE probe was introduced only when needed. Thus, there was only minor influence on the temperature measurements. TOE was only recorded continuously during valve replacement surgery (under normothermia and mild hypothermia). Hence, reliable oesophageal temperature monitoring was not feasible in these patients. As ice packs were used for external cooling, this might influence measurements of the heat flux system, on the one hand, by heat conduction to the direct vicinity and by local vasoconstriction, on the other hand. Nevertheless, the distance between ice packs and sensors was maximized (within clinical limits) to ensure a negligible interaction. Body temperature and specific temperatures of organ systems are determined by the isolative properties of the heatconducting tissues, the flow of the CPB, and the blood perfusion temperature. Previous studies in this field have reported considerable differences in measured correlations of organ temperatures.9 – 12 21 On a technical level, most of the clinically used thermosensors are fairly sensitive. It can be deducted that differences are attributed to inter-individual variations in body mass and body composition and also vascularization and blood flow. Compared with Kimberger and colleagues,13 who validated a cranial heat flux sensor in intensive care, referenced by oesophageal temperature, deviations (CI) were greater and a CCC showed little agreement during stationary normothermic 773 BJA measurements. This might be attributable to the distance between sensor positions. Moreover, these measurements were not performed during open-heart surgery. Because of the thoracotomy procedure, the oesophageal temperature is not always considered a reliable method in cardiac surgery24 as an isolated approach. Thus, in combination with the temperature of the membrane oxygenator,12 the vesical temperature is often regarded sufficiently accurate to provide a monitoring method for the dissipation of temperature throughout the body.24 – 27 Although there has been doubt about the responsiveness of vesical sensors in the literature regarding a changed heat exchange because of changes in urine production,26 – 30 no significant change in the correlation coefficients was observed (P≥0.05). It should be further investigated whether peripheral perfusion and differences in organ perfusion are significant modulators of the shape of the hysteretic loops. During extensive operations, temperature should be monitored in the vicinity of the organ of interest (brain and heart), as it seems to be obvious that the more remote the sensor position, the greater the effect of non-linearity. For correlations of different sensors and sensor positions, a non-linear model should be considered, as it displays a more accurate representation of the heat memory of specific tissues. Clinically, it is of vital interest to respect the direction dependence of the thermoregulatory system, when interpreting measured body temperatures. Acknowledgements We wish to express our gratitude to the whole team responsible for measurements in the German Heart Institute. Furthermore, we acknowledge and thank all patients for their participation to help make temperature measurement more reliable. Declaration of interest H.C.G. has been serving as a consultant to the Draegerwerk AG & Co. KGaA. The other authors do not have any financial interest in any company related to this manuscript. Funding This investigation was supported by grant 50WB1030 from the German Aerospace Agency (DLR). References 1 Wunderlich CRA. Das Verhalten der Eigenwärme in Krankheiten, 1st Edn. Leipzig, Germany: Verlag von Otto Wigand, 1870 2 Kurz A. Thermal care in the perioperative period. Best Pract Res Clin Anaesthesiol 2008; 22: 39 –62 3 Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA 1997; 277: 1127–34 4 Connolly E, Worthley LI. Induced and accidental hypothermia. Crit Care Resusc 2000; 2: 22– 9 5 Polderman KH. Mechanisms of action, physiological effects, and complications of hypothermia. Crit Care Med 2009; 37: S186– 202 774 Opatz et al. 6 ECC Committee SaTFotAHA. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2005; 112: IV1–203 7 Holzer M, Behringer W, Schorkhuber W, et al. Mild hypothermia and outcome after CPR. Hypothermia for Cardiac Arrest (HACA) study group. Acta Anaesthesiol Scand Suppl 1997; 111: 55 –8 8 Nolan JP, Morley PT, Vanden Hoek TL, et al. Therapeutic hypothermia after cardiac arrest: an advisory statement by the advanced life support task force of the International Liaison Committee on Resuscitation. Circulation 2003; 108: 118 9 Stone JG, Young WL, Smith CR, et al. Do standard monitoring sites reflect true brain temperature when profound hypothermia is rapidly induced and reversed? Anesthesiology 1995; 82: 344– 51 10 Washington GT, Matney JL. Comparison of temperature measurement devices in post anesthesia patients. J Perianesth Nurs 2008; 23: 36– 48 11 Zeiner A, Klewer J, Sterz F, et al. Non-invasive continuous cerebral temperature monitoring in patients treated with mild therapeutic hypothermia: an observational pilot study. Resuscitation 2010; 8: 861–6 12 Nussmeier NA, Cheng W, Marino M, et al. Temperature during cardiopulmonary bypass: the discrepancies between monitored sites. Anesth Analg 2006; 103: 1373– 9 13 Kimberger O, Thell R, Schuh M, Koch J, Sessler DI, Kurz A. Accuracyand precision of a novel non-invasive core thermometer. Br J Anaesth 2009; 103: 226–31 14 Gunga HC, Sandsund M, Reinertsen RE, Sattler F, Koch J. A noninvasive device to continuously determine heat strain in humans. J Thermal Biol 2008; 33: 297–307 15 Gunga H-C, Werner A, Stahn A, et al. The double sensor—a noninvasive device to continuously monitor core temperature in humans on earth and in space. Respir Physiol Neurobiol 2009; 169(Suppl. 1): S63–8 16 Lin LI. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989; 45: 255–68 17 Lin LI. Corrections. Biometrics 2000; 56: 324– 25 18 Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307– 10 19 Parkhurst AM. Model for understanding thermal hysteresis during heat stress: a matter of direction. Int J Biometeorol 2010; 6: 637– 45 20 Ozaki M, Sessler DI, McGuire J, Blanchard D, Schroeder M, Moayeri A. The direction dependence of thermoregulatory vasoconstriction during isoflurane/epidural anesthesia in humans. Anesth Analg 1993; 77: 811–6 21 Sessler DI. Perianesthetic thermoregulation and heat balance in humans. FASEB J 1993; 7: 638– 44 22 Kiyatkin EA. Brain temperature fluctuations during physiological and pathological conditions. Eur J Appl Physiol 2007; 101: 3–17 23 Sessler DI. Temperature monitoring and perioperative thermoregulation. Anesthesiology 2008; 109: 318– 38 24 Camboni D, Philipp A, Schebesch KM, Schmid C. Accuracy of core temperature measurement in deep hypothermic circulatory arrest. Interact Cardiovasc Thorac Surg 2008; 7: 922– 4 25 O’Grady NP, Barie PS, Bartlett JG, et al. Guidelines for evaluation of new fever in critically ill adult patients: 2008 update from the American College of Critical Care Medicine and the Infectious Diseases Society of America. Crit Care Med 2008; 36: 1330–49 26 Fallis WM. Monitoring bladder temperatures in the OR. AORN J 2002; 76: 467– 76, 81 –6, 88 –9 Non-linearity of physiological recordings 27 Erickson RS, Kirklin SK. Comparison of ear-based, bladder, oral, and axillary methods for core temperature measurement. Crit Care Med 1993; 21: 1528– 34 28 Horrow JC, Rosenberg H. Does urinary catheter temperature reflect core temperature during cardiac surgery? Anesthesiology 1988; 69: 986– 9 BJA 29 Langham GE, Maheshwari A, Contrera K, You J, Mascha E, Sessler DI. Noninvasive temperature monitoring in postanesthesia care units. Anesthesiology 2009; 111: 90– 6 30 Bone ME, Feneck RO. Bladder temperature as an estimate of body temperature during cardiopulmonary bypass. Anaesthesia 1988; 43: 181– 5 Handling editor: L. Colvin 775