Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
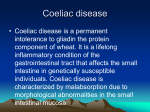
STATION MEDICAL GROUP Spring 2016 Inside This Issue News Staff update and news Fund raising activities Proposed merger of Station and Waterloo practices Patient satisfaction questionnaire Promoting Health Skin Cancer - Be Sun `Aware Meet our Team - Ryan Davies –Placement Student Emergency Health Care Plans It happened to me Personal patient Perspective Did you Know? ‘Going Online’ Prescriptions – The cost of unused prescribed drugs Healthy recipe ISSUE 8 Practice News In the 6 months since the last newsletter was published there have a number of developments at Station Medical Group. On the staffing side: Dr Pepper Atkinson went on maternity leave and is delighted to announce that she now has a beautiful baby girl called Georgia. During her absence, Dr John Waddell (known to many patients, and who retired as a Partner at the end of September) has kindly been providing locum cover for the last 5 months. Dr Helen Harman is also expecting her first child in June and as such will shortly be going on maternity leave from mid May. To help provide GP cover during this period we will have 2 new locum GP’s at the practice for the next 6 months, these will be Dr Rashmi Karle and Dr Anne-Marie Cole. Both GP’s have an excellent reputation and the Partners at Station Medical Group feel that they are an excellent addition to the Practice. Since the last Newsletter the staff at Station Medical Group have undertaken 3 fund raising activities to support both local and national charities. The charities they have provided donations for are: Help for Heroes, Cystic fibrosis and Text Santa. Proposed merger of Station Medical &Waterloo Medical Groups Due to the increased demands on Primary Care and problems with GP recruitment and retention, the doctors at Station Medical Group and Waterloo Medical Group are proposing to merge practices. We hope that this will enable us to continue to provide a high standard of health care in increasingly challenging circumstances . We would like to reassure patients that there will be no changes to the level of care you already receive. However, we do hope that by merging we are able to offer more GP appointments and offer more specialist care within the practice by potentially developing new services. The proposed merger would take place in April 2017. Full details and ‘Frequently Asked Questions’ are available on our website or at the surgery. Drop-in information sessions at the surgery are also planned. Practice Opening Hours: Main doors are open from 0830-1830. Appointments available 0830-1115; 1355-1745. The reception is open but there is Practice Opening Hours: Main doors are open from 0830-1230 and 1330-1800 no clinical cover between 12.30-1.30 – Friday.Telephone lines are open from 0830-1830 Monday to Friday – (includes Main telephone number:Monday 01670 542630. ctice Opening Main doors are open from 0830-1230 and 1330-1800 prescription line option - available from Hours: 0930-1200 and 1330-1600) Monday – Friday. Out of hours phone: for Medical Emergency 999; for routine medical assistance 111. Website: stationmedicalgroup-blyth.nhs.uk STATION MEDICAL NEWSLETTER Practice News (contd) PAGE 2 One of the questions anticipated would be about the Blyth Acute Centre eg: Q: Will Blyth Acute Service still run as it does now? A: Since the BAS first started in Feb 2015 it has proved a huge success with patients from both practices, with 95% of patients either very likely or likely to recommend the service to friends and family. As such, we will definitely be continuing this service. Patient Satisfaction Questionnaire A random survey of 120 patients - attempting to cover as diverse a population as possible, was held at the beginning of the year. We would like to thank everyone who participated for their time. The results have been reviewed and will be reported back to patients in due course. Promoting Health - Be Sun Aware In every issue we will highlight a particular health topic. This issue covers SUN AWARENESS Information on this topic is available in the waiting area Skin cancer is very common in the UJK. Finding skin cancer early can save lives. The main causes of skin cancer are too much ultraviolet radiation from the sun, and excessive exposure or the frequent use of sun beds. Basal Cell Carcinoma is the most common form of skin cancer. Fortunately it is slow growing and rarely spreads to other areas or organs in the body, Squamous Cell Carcinoma is the second most common form of skin cancer. Squamous cell carcinoma are fortunately slow–growing and usually remain in the outer layer of the skin. If left untreated it has the ability to spread to other organs in the body. Malignant Melanoma (also known as Melanoma) is the most serious form of skin cancer and is more likely to spread if not treated in the early stages. It is important that it is recognised early. What to look for: Get to know what your skin normally looks like. Notice any changes in how your skin looks or feels. Skin cancer may appear as a new mark or mole, or it can be something you have had for a while but has changed. See your Doctor if a mole or mark on your skin: Grows Bleeds Changes in appearance in any way. Never heals completely If any existing moles change shape, colour or texture. Spring - April 2016 STATION MEDICAL NEWSLETTER PAGE 3 Risk Factors SUN AWARENESS Anyone can develop skin cancer, but some people are more at risk than others and can include the following: More information on Skin Cancer will be displayed in the practice waiting area during the summer months . Please take the information leaflets and booklets, which will be available. Fair skin. Light coloured eyes. Natural blonde or red hair. An outdoor occupation and being exposed to the sun without the use of sunscreen. Have been sunburnt in the past Numerous freckles. Outdoor hobbies without use of sunscreens. A history of skin cancer. Taking medication that suppresses the immune system, Avoiding Skin Cancer Skin cancer can occur on any part of the body, but most frequently on sun exposed areas such as the face, neck, lips, ears, hands, shoulders and limbs. Check your skin regularly Report any changes to your doctor Do not use sunlamps or sunbeds Always protect yourself from the sun by applying a high factor sunscreen and reapply regularly. Cover-up: wear a T-shirt, a wide brimmed hat and wraparound sunglasses. Stay in the shade between 11.00 am and 3.00 pm. Keep young babies out of the sun. Did you know? Going Online Medical Records Prescriptions Sun awareness information will be displayed on the notice board in the patient waiting area during the summer months. Please take the information/advisory leaflets and cards available. The above information was taken with permission from the British Association of Dermatologists, The Wessex Cancer Trust and Cancer Research UK. Online Access Appointments What is online access? ___________________ Station Medical have the facility for patients to use their website www.stationmedicalgroup-blyth.nhs.uk via your own home computer or tablet, to communicate with the practice, instead of/or as well as using the phone or calling in in person. Once registered, you will be able to access parts of your medical record including medications, allergies and immunisations. You will also have the option to order repeat medications and book appointments online. Spring - April 2016 STATION MEDICAL NEWSLETTER Did you know? Going Online Medical Records Prescriptions Appointments ___________________ PAGE 4 How do I register? You will need to come down to the surgery with photographic ID to verify your identity. If you do not have any photographic ID (eg passport or driving license with photograph) please bring a recent utility bill showing your name and home address (bank statement etc). You will then be given a registration document containing your pin key and account ID, this is the information you need to register online. You would do this by visiting our website at www.stationmedicalgroupblyth.nhs.uk and clicking on the online appointments or repeat prescription ordering button on the main page. You will then be taken to the registration page where you can enter all your details and create your account. What are the benefits of online access? Repeat prescriptions Saves you time as you can order your repeat medications 24hrs a day at your convenience. order prescriptions when the prescription line is closed (helpful if you can’t find the time to ring during opening hours). add messages to your order. have your repeat medications sent directly to a pharmacy - this saves a trip down to the GP surgery. Online Appointments A percentage of appointments will be available to book online, again this can be accessed 24hrs a day (please note only one appointment per person can be booked). The appointments are released in the same way as our current appointment system. Other parts of medical record No need to ring the surgery to find out immunisation and allergy details as these will be displayed in your online access account. In the future there will be more online access medical records available. Spring - April 2016 STATION MEDICAL NEWSLETTER Meet our team Ryan Davies, Placement Student This section is used to get to know members of the practice team; about them personally or their work and interests. This article was provided by a Medical Student on secondment to the practice, to gain invaluable first-hand experience of working in general practice – mentored and supported by our GPs. PAGE 5 Emergency Health Care Plans and why they should matter to you – Ryan Davies, Newcastle University Medical Student Emergency Health Care Plans (EHCPs If you’re reading this and you or a family member have a long term medical condition, read on. If that condition deteriorated and possibly required a hospital admission, GP home visit or access to the Blyth Acute Service, would you know which option to choose? Well; Emergency Health Care Plans (EHCPs) are documents designed to do this. They also help reduce unplanned hospital admissions and are for specifically identified high risk patients. They are not produced to stop anyone from going to hospital when needed and the potential reduction in admissions will actually equate to a better standard of care overall in other services. They are also important in allowing patients more ownership and decision making with regards to their own treatment. EHCPs should be completed by a health care professional in conjunction with the patient and/ or their family or carer. It outlines medical history, current health issues and medication. It also states the patient’s wishes and what to do in specific anticipated emergencies. It should be kept by the patient at their home and referred to in the event of an emergency by themselves, their family/ carers or ambulance staff. Sound useful? This is the theory at least. As a medical student recently attached to Station Medical Group, I was tasked with assessing how well these documents were actually used by their target cohort – you the patients. The results showed that we needed to raise more awareness of these so a follow up and review programme has begun. Many patients who may require an EHCP also have a carer or family member who is actually the one who takes much of the responsibility for their well-being. For instance, 21% of patients with an EHCP also had a diagnosis of dementia and 36% were care home residents. Therefore, their carers should also ideally be present when the document is agreed and the plan put in place, or at least alerted to its existence thereafter. Finally, if you have or look after someone who has an EHCP – remember to have it handy should you need to call an ambulance or go to hospital. It can save a lot of time to have a document with all relevant medical details to give to them. If it’s not an emergency, but you’re worried about a condition deteriorating – remember to refer to it. When done well, it should help you make decisions about what to do; whether this is starting to take a rescue pack for COPD or Asthma, changing medication dose or what symptoms/ situations may require either a call to the GP surgery or an ambulance. If this applies to you or someone you care for, please find out more. Spring - April 2016 STATION MEDICAL NEWSLETTER PAGE 6 It happened to me …. It happened to me… It could happen to you? A personal perspective from one of our patients As a regular topic we include an anonymous article from one of our patients about their own very personal experience with an illness. This is their own experience, in their own words and not a professional view, but it might be of interest to help fellow sufferers or their carers. COELIAC DISEASE I was a teenager when I first noticed some of the symptoms of Coeliac Disease. Like lots of teenagers, I was often tired, but I also kept getting sore tummies. On evenings out with friends I often had a bod stomach, felt faint and had to go home early. It gradually got worse and eventually when I was feeling generally unwell, I went to see the doctor. After visiting the doctor I had blood tests taken – they came back showing low white blood cell count. Further biopsies and an endoscopy (a camera down into my stomach) came back with results showing signs of coeliac. I had to change my diet, but noticed a huge improvement. I was more alert, less bloated and gradually had an increase of energy. It was quite difficult at times to accept my new diet, but I felt so much better. I miss bread and the convenience of fast food – ie. MacDonalds. After a night out with friends, often they fancy a McD or a takeaway, but I can’t – which is a bit of a drag. My mum has been able to source gluten free flour and bread and fortunately manages to even make gluten-free cakes and other nice recipes which everyone can eat so I don’t always need to eat differently from the rest of the family. Now I am 25 and have become used to this way of life. I don’t really have a choice because Coeliac Disease cannot be cured – it has to be managed by following a strict, lifelong gluten-free diet. I am actually eating a much better and healthier diet, as you eat more fresh food. But you do get used to it and I go out with my friends anyway and join in the fun. The most difficult thing is when eating out. Even when there are items marked gluten-free you have to be careful as it is easy for there to be cross contamination. At least now it is much easier to find gluten-free products than it used to be and you can find quite a good range in most supermarkets as well as specialist shops. What is coeliac Disease? Coeliac disease (pronounced’ see-liac’) is a serious illness where the body’s immune system attacks its own tissues when gluten is eaten. This causes damage to the lining of the gut and means that the body cannot properly absorb nutrients from food. It is not an allergy or simple food intolerance. Gluten is a protein found in wheat, barley and rye. Some people may also be sensitive to oats. Around 1 in 100 people have coeliac disease, although it remains underdiagnosed. Coeliac disease does run in families, but not in a predictable way. Overall, about 1 in 10 close relatives of people with CD may be susceptible. I am a member of Coeliac UK who support sufferers and campaign and research this disease. They also publish latest information on new food products and suppliers. For more information they can be contacted on Tel: 0333 332203; www.coeliac.org.uk; www.facebook.com/Coeliac.uk Spring - April 2016 STATION MEDICAL NEWSLETTER PAGE 7 MEDICINES WASTE Did you know Medicines Waste and the cost to the NHS HOW DOES IT OCCUR AND HOW CAN YOU HELP? Sometimes patients receive medicines they don't actually use, or use only occasionally. This means that they can lose out on the intended health benefits of their prescription. And that can be a major headache in more ways than one. Not only does it meanthat their symptoms can get much worse if left untreated - the latest Department for Health report suggests this can cost the NHS many, many millions in avoidable extra treatment costs - it also means that these medicines cannot be used again and need to be incinerated. The reasons why patients don’t take all their medication can vary and audits have shown that around half of all the medication returned had not even been opened. This means that patients are ordering and receiving medication that they don’t even start to use. It is estimated that as much as £300 million is wasted every year on unused or partially used medication. That's money which could be reinvested into more front line care and services for the benefit of all. To put this into context, here's what £300 million could buy: 80,906 MORE hip replacements* 101,351 MORE knee replacements* 19,799 MORE drug treatment courses for breast cancer* 11,778 MORE community nurses* 300,000 MORE drug treatment courses for Alzheimer's* *Based on average costs How can you help? Please only order the medicines that you need Do not stockpile medication If you STOP taking a medication please inform the surgery or your pharmacist as soon as possible Double check your prescription order before placing it and when you receive it to ensure you have the correct items. Visit http://www.medicinewaste.com/ for more information Comment: Do you have a pile of unused medications, tablets etc. in your bathroom cupboards/a drawer? If so , why? Do not put them down the toilet, give them to someone else or put them in the bin. Return them to any pharmacy who will dispose of them safely, no questions asked. Do not re-order these meds. Cancel them from your prescription, and tell your GP you no longer need them. The money saved could go towards something important. Spring - April 2016 STATION MEDICAL NEWSLETTER Tasty and inexpensive recipe Tested and recommended by one of our patients PAGE 8 Ham and Cheese Bake ( or savoury bread pudding!) Serves 4 people Ingredients Butter for greasing 1 baguette (I used wholemeal bread cut into pieces) 90gm sliced ham torn into small pieces (I used some cooked bacon and some boiled ham) 150gm/5oz. Gruyere cheese grated. (I used strong cheddar) 5 eggs half pint milk 284 pot single cream (I used Elmlea light single cream) 1 tblsp Dijon mustard. Method Delivering a service for approximately 10,000 patients in the Blyth area Please use the Suggestion Box on Reception and PPG to voice your views. Newsletter: We welcome ideas for topics of interest from all ages, and would especially like to hear from young people. PPG Grease the bottom of a deep 20x30cm baking dish with a little butter. Tear or cut the baguette into bite sized pieces then arrange over the bottom of the dish. Tuck the ham pieces and grated cheese in between the gaps. Whisk together the eggs, milk, cream and mustard and pour over the bread. Cover and chill for at least 3 hours or preferably overnight (in fridge). Heat oven to 180c/fan160c/gas 4. Bake for 40-45 minutes until the top is crisp and golden and the egg mix is cooked through. If the topping browns a little too quickly, cover with foil for the remainder of the cooking time. Serve immediately. Note: I used the bread as I would when making a sweet bread pudding but in layers with ham and cheese between them. The Patient Participation Group is made up of volunteer patients who attend meetings every two months with practice staff to give feedback from/represent all patients and to take a proactive role in building the relationship between the SMG and their patients. We would like to represent all member s of the community and all ages. If you would like to be involved, particularly if you are 18-30, we would like to hear from you. Ask at reception. Spring - April 2016