Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
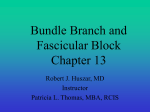
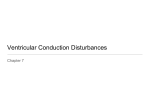
JOURNAL OF INSURANCE MEDICINE VOLUME 25, NO. I SPRING 1993 T-WAVE ABNORMALITIES IN BUNDLE BRANCH BLOCK John R. Iacovino, MD, FACP, FACC The purpose of this review is to familiarize the medical If pre-BBB T-wave negativity exists, when BBB develunderwriter with primary and secondary T-wave con- ops, the T-waves will not become secondary and revert figurations in right and left bundle branch block (RBBB, to upright; they will remain primary and negative.2 LBBB). In RBBB, secondary or normal T-waves in leads I, aVL, Whether the T-wave in bundle branch block is primary V4-5-6 are upright; in V1-2 they are usually inverted. A or secondary can have a major impact on the correct risk reverse of the T-wave axis in these or other leads where classification. T is in the same direction as the terminal QRS complex is a primary abnormality.2’3 (Figure 1) Following depolarization, the rate of repolarization throughout the myocardium should be uniform. Nor- Primazy and secondary changes are also seen in LBBB. mall~ this produces QRS complexes and T-waves that As in RBBB; the T-wave is normally oriented opposite are of equal area but opposite axial orientation. How- to the direction of the terminal portion of the QRS ever, for physiologic reasons beyond the scope of this complex. Primary changes in LBBB most commonly review, the heart has a ventricular gradient which include upright T-waves in leads I, aVL, V5-6.2 (Figure causes the electrocardiogram to record positive wave 2.) forms for both QRS and T.1 In both BBB, the magnitude of the T-wave (depth and Repolarization alternatives depend upon two factors: width) is proporUonal to the area of the widened QRS. Therefore, with a primm’y abnormality, the area of the 1. The direction of depolarization. T-wave has a greater relationship to the (~RS duration than to the underlying causative etiology." 2. Anatomic and physiologic variations in the myocardium. ST orientations can also be primary and secondary though less dramatic than T-wave changes. As with There are two forms of T-wave repolarizatioin- primary T-waves, the ST segments are also expected to be oriand secondary. 1,2 ented in the opposite direction as the terminal portion of the QRS.2 Often these are subtle and comparisons Erimazy_T-waves are associated with abnormalities with old ECGs are needed. in the myocardium and are independent of the order of depolarization. Therefore, primary T-waves imRBBB is commonly a benign electrocardiographic findply a fundamental change in the myocardium. ing not associated with underlying cardiac disease. ~ forms are dependent on the altered However, primary T-waves with RBBB must alert the underwriter to the possibility of coexistent heart discourse of depolarization and independent of the state of the myocardium; they are intrinsic to the ease. With LBBB, primary T-waves may have less sigblock itself. nificance since the conduction abnormality itself is usually a marker of underlying heart disease. However, Primary T-waves may be produced by diminished the risk may be compounded by the combination of a blood supply to the myocardium, metabolic abnormali- conduction system plus myocardial disease. P~ ties, tachycardia and drugs such as digitalis. In addition T-waves in LBBB may represent myocardial infarction. to BBB, secondary T-waves are commonly seen in premature ventricular contractions.1 1. Lipman BS, Massie E. Clinical Scalar Electrocardiography, 5th ed. Normally in BBB, T-waves are oriented in the opposite Chicago, IL, Year Book Medical Publishers Inc, 1965:70-76. direction of the terminal portion of the widened QRS 2. Constant J. Learning Electrocardiography - A Complete Course, 2nd Ed. Boston, MA, Little, Brown and Co, 1981: 135-37. complex (secondary changes).2 3. Elion JL. ECG changes in right bundle-branch block. Choices in CardiologySept/Oct 92; 6(5):170-171. When in BBB the T-wave is the same direction as the FJ, Lie KI, Koster DRM, Wellens I-IJJ. Assessment of the .t.e..nninal portion of the QRS complex, it is a primm’y 4.Wackers value of electrocardiographic signs of myocardial infarction in left 2 configuration. bundle branch block. In: Wellens HJJ, KCflbertus HE. What’s New in Vice President & Medical Director, New York Life Insurance Compan~ New York, New York. Electrocardiography. The Hague, Martinus Nijhoff Publishers, 1981:3754. 19 VOLUME 25, NO. I SPRING 1993 T-WAVE ABNORMALITIES Figure 1 Right Bundle Branch Block Showing Primary T-Wave Changes in Leads V1, V2, and V& Additionally, the applicant had an anterior myocardial infarct. 2o JOURNAL OF INSURANCE MEDICINE VOLUME 25, NO. 1 SPRING 1993 Figure 2 Left Bundle Branch Block Showing Primary T-Wave Changes Leads I, aVL, and Vs-V6. 21