Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
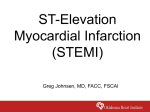
Archives of Cardiovascular Disease (2014) 107, 149—157 Available online at ScienceDirect www.sciencedirect.com CLINICAL RESEARCH Heart failure with systolic dysfunction complicating acute myocardial infarction — differential outcomes but similar eplerenone efficacy by ST-segment or non-ST-segment elevation: A post hoc substudy of the EPHESUS trial Insuffisance cardiaque systolique post-infarctus du myocarde — un pronostic différent mais une efficacité similaire de l’éplérénone chez les patients avec ou sans sus-décalage du segment ST : une sous-étude post hoc d’EPHESUS Sylvain Carillo a,∗, Yan Zhang b, Renaud Fay a, Michael Angioi c, John Vincent d, Santosh C. Sutradhor d, Ali Ahmed b, Bertram Pitt e, Faiez Zannad a a Inserm U961, cardiology, centre d’investigations cliniques CIC9501, institut Lorrain du cœur et des vaisseaux, CHU de Nancy, 2, avenue du Morvan, 54500 Vandoeuvre-Lès-Nancy, France b University of Alabama at Birmingham and VA medical center, Birmingham, AL, USA c Clinic Louis-Pasteur, 54270 Essey-Lès-Nancy, France d Pfizer Inc., New York City, NY, USA e University of Michigan, Ann Arbor, MI, USA Received 20 October 2013; received in revised form 18 January 2014; accepted 21 January 2014 Available online 11 March 2014 Abbreviations: ACS, Acute coronary syndrome; AMI, Acute myocardial infarction; CI, Confidence interval; EPHESUS, Eplerenone PostAcute Myocardial Infarction Heart Failure Efficacy and Survival Study; GRACE, Global Registry of Acute Coronary Events; HF, Heart failure; HR, Hazard ratio; LVEF, Left ventricular ejection fraction; LVSD, Left ventricular systolic dysfunction; NSTEMI, Non-ST-segment elevation myocardial infarction; PS, Propensity score; STEMI, ST-segment elevation myocardial infarction. ∗ Corresponding author. E-mail address: [email protected] (S. Carillo). 1875-2136/$ — see front matter © 2014 Elsevier Masson SAS. All rights reserved. http://dx.doi.org/10.1016/j.acvd.2014.01.010 150 KEYWORDS NSTEMI; STEMI; Heart failure; Eplerenone MOTS CLÉS IDM ST— ; IDM ST+ ; Insuffisance cardiaque ; Éplérénone S. Carillo et al. Summary Background. — Differential outcomes in patients with acute systolic heart failure (HF) complicating acute myocardial infarction (AMI) and the efficacy of mineralocorticoid receptor antagonists according to non-ST-segment and ST-segment elevation myocardial infarction (NSTEMI, STEMI) status has not been specifically investigated. Methods. — In the EPHESUS study, 6632 patients with acute HF and left ventricular ejection fraction < 40% were randomized 3—14 days post-AMI (median 7.3 ± 3.0 days) to receive eplerenone (n = 3319) or placebo (n = 3313). Among them, 6392 patients with available data on baseline STsegment status (4634 STEMI; 1758 NSTEMI) were compared using a Cox model analysis stratified according to quintiles of propensity score (PS), taking into account major baseline risk factors, including revascularization. Results. — STEMI and NSTEMI patients differed significantly across a large variety of baseline characteristics. During 30 months of follow-up, all-cause death occurred in 19% and 13% (P < 0.0001), cardiovascular death in 16% and 12% (P < 0.0001), cardiovascular death and hospitalization in 33% and 26% (P < 0.0001) and death from progression of HF in 5% and 3% (P < 0.0001) of unadjusted NSTEMI and STEMI patients, respectively. After Cox model PS adjustment without revascularization, NSTEMI status still proved to be a risk factor for all-cause death, cardiovascular death and death from progression of HF. After Cox model PS adjustment including revascularization, none of the outcomes differed between STEMI and NSTEMI patients. Eplerenone morbidity and mortality benefits were consistent in the STEMI and NSTEMI subgroups. Conclusion. — In patients with acute systolic HF complicating AMI, eplerenone improves outcomes equally in STEMI and NSTEMI patients. Worse outcomes associated with NSTEMI could be explained by more co-morbidities, less aggressive therapies and, mainly, less frequent revascularization. © 2014 Elsevier Masson SAS. All rights reserved. Résumé Contexte. — Le pronostic des patients en insuffisance cardiaque (IC) systolique aiguë postinfarctus du myocarde (IDM), ainsi que l’efficacité des antagonistes des récepteurs aux minéralocorticoïdes en fonction de l’élévation (ST + ) ou non (ST—) du segment ST n’a pas encore été étudiée de manière spécifique. Méthodes. — Dans l’étude EPHESUS, 6632 patients en IC aiguë avec une fraction d’éjection < 40 % ont été randomisés entre j3 et j14 post-IDM (médiane de 7,3 ± 3,0 jours) pour recevoir de l’éplérénone (n = 3319) ou un placebo (n = 3313). Parmi eux, les 6392 patients ayant des données exploitables sur l’état du segment ST à la phase aiguë de l’IDM (4634 ST+ et 1758 ST—) ont été analysés selon le modèle de Cox stratifié par quintiles de score de propensité prenant en compte les principales données, y compris le taux de revascularisation, différent de manière significative entre les groupes ST+ et ST—. Résultats. — Au terme des 30 mois de suivi de l’étude, l’analyse sans ajustement par score de propensité retrouve un pronostic plus péjoratif pour les ST—, avec des taux de décès toute cause de 19 % vs 13 % (p < 0,0001), de décès cardiovasculaire de 16 % vs 12 % (p < 0,0001), de décès cardiovasculaire/hospitalisation cardiovasculaire de 33 % vs 26 % (p < 0,0001) et de décès par IC de 5 % vs 3 % (p < 0,0001) observés respectivement chez les ST— et les ST+. Après ajustement par quintiles de score de propensité sans tenir compte du taux de revascularisation, le statut ST— demeure plus péjoratif puisqu’il est un facteur de risque de décès toute cause, décès cardiovasculaire et décès par insuffisance cardiaque. Le fait d’inclure le taux de revascularisation à l’analyse précédente abolit totalement la différence de pronostic entre les patients ST— et ST+. Par ailleurs, les bénéfices de l’administration d’éplerénone mesurés en termes de morbidité et de mortalité sont identiques chez les patients ST— et ST+. Conclusions. — Chez les patients en IC systolique aiguë post-IDM, le bénéfice lié à l’administration d’éplérénone est identique chez les ST— et les ST+. Le pronostic plus défavorable observé chez les ST— s’explique par des comorbidités plus importantes, des traitements médicamenteux moins agressifs, mais surtout un taux de revascularisation plus faible. © 2014 Elsevier Masson SAS. Tous droits réservés. NSTEMI, eplerenone and outcomes Background Nearly half of all patients with acute myocardial infarction (AMI) present left ventricular systolic dysfunction (LVSD) and one quarter show symptoms of heart failure (HF), both of which are associated with poor outcomes [1—6]. Nevertheless, the Global Registry of Acute Coronary Events (GRACE) has shown that the spread of evidence-based therapies and myocardial revascularization has halved the rate of HF during AMI [2]. Still, this complication remains challenging, as 80% of morbidity and mortality in the acute phase of myocardial infarction is to be found in this subgroup [7,8]. Regardless of LVSD or HF, there are clear prognostic differences between patients with non-ST-segment elevation myocardial infarction (NSTEMI) and those with ST-segment elevation myocardial infarction (STEMI). Indeed, hospital prognosis is known to be better for NSTEMI patients [9—11], whereas long-term prognosis is described as better for STEMI patients [10,12,13]. Aldosterone is a mediator of the renin-angiotensinaldosterone system, which is known to produce adverse cardiovascular effects in post-AMI patients, such as left ventricle remodelling and endothelial dysfunction [14]. The Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) [15] conducted in post-AMI patients complicated by acute HF and LVSD, showed that the mineralocorticoid receptor antagonist eplerenone improved morbidity and mortality outcomes. Different outcomes in patients with acute HF and LVSD complicating AMI and the efficacy of mineralocorticoid receptor antagonists depending on NSTEMI and STEMI status has not been specifically investigated. In EPHESUS, AMI patients complicated by LVSD and receiving standard medical therapy were randomized to eplerenone versus placebo. In the current analysis, we compared outcomes and eplerenone benefits depending on NSTEMI and STEMI status, using a propensity score (PS)-adjusted Cox model. Methods Study design EPHESUS was an international randomized double-blind placebo-controlled clinical trial, the design and results of which have been previously reported [15]. Briefly, 6632 hospitalized post-AMI patients with left ventricular ejection fraction (LVEF) ≤ 40% were randomized within 3 to 14 days (median 7.3 ± 3.0 days) post-AMI to receive either eplerenone (mean dose 43 mg/day) or placebo during the 2000—2001 period. LVEF was measured and analysed at the study site by echocardiography, radionuclide angiography or left angiography. Revascularization was performed using thrombolysis, percutaneous coronary angioplasty and/or coronary artery bypass grafting. All patients received standard medical therapy and most had HF symptoms, diagnosed clinically by the presence of pulmonary rales, a third heart sound or pulmonary vascular congestion on chest radiography. However, patients without HF symptoms could be enrolled if they had diabetes. Overall, 2142 (33%) patients had diabetes, among whom 659 (10% of all patients and 31% of all diabetics) had no HF symptoms. Patients were 151 followed for up to 2.5 years, with a mean 16-month followup. Study patients Of the 6632 EPHESUS participants, 6510 (98%) had data on ST-segment status. These patients were classified as having NSTEMI or STEMI by the study investigators, based on their interpretation of the electrocardiogram; 118 were excluded from the analysis due to missing values for the 20 selected baseline variables used for PS-matching. Therefore, observations from 6392 subjects (1758 [27%] NSTEMI; 4634 [73%] STEMI) were used for the analysis. Data on sociodemographic, clinical, subclinical and laboratory variables were collected at baseline and have been reported previously [15]. Study outcomes Primary outcomes of interest for the current analysis were all-cause death, cardiovascular death, cardiovascular death or hospitalization and death from progression of HF during the 2.5 years of follow-up. These events were adjudicated by a blinded EPHESUS critical events committee [15]. We examined the association of eplerenone treatment with primary outcomes of interest, depending on STsegment status. Statistical analyses All analyses were performed using SAS 9.2 (SAS Institute Inc., Cary, NC, USA). The two-tailed significance level was set at P < 0.05. Continuous variables are expressed as means ± standard deviations, categorical variables as frequencies and percentages and hazard ratios (HRs) as estimates and 95% confidence intervals (CIs). Comparisons of baseline characteristics were carried out using the MannWhitney U test and Pearson’s Chi2 test, as appropriate. The association of eplerenone and NSTEMI with four selected outcomes (all-cause death, cardiovascular death, cardiovascular death or cardiovascular hospitalization and death from progression of HF) was analysed using the Cox proportional hazards model. STEMI and NSTEMI patients differed significantly in a number of features: using logistic regression, a PS was constructed as the probability of an individual to present NSTEMI based on the 20 selected baseline characteristics presented in Table 1. Two separate PSs were computed separately, including or not including revascularization, in order to investigate its effect on prognosis. A sensitivity analysis was done using PS-matching, according to all 64 available baseline characteristics. Time-to-event analyses were then carried out with eplerenone and NSTEMI as exposition factors and PS quintiles as stratification variables, which allowed the number of factors in the model to be reduced and prevented any issue of log-linearity between PS and outcomes. The validity assumptions of the Cox models (proportionality of hazards, absence of interaction and co-linearity) were thoroughly checked and any violation was ruled out. The association of eplerenone with outcomes according to ST-segment status was illustrated using Kaplan—Meier curves. 152 Table 1 S. Carillo et al. Baseline characteristics. NSTEMI (n = 1758) n Region North America Western Europe Eastern Europe Latin America Other 403 428 669 100 158 Pa STEMI (n = 4634) Mean ± SD or % n Mean ± SD or % 23 24 38 6 9 384 1198 2210 456 386 8 26 48 10 8 < 0.0001 Demographics Men Age (years) 1194 1758 68 66.9 ± 11.1 3350 4634 72 62.6 ± 11.4 0.0006 < 0.0001 Risk factors Body mass index (kg/m2 ) History of hypertension Diabetes Prior history of AMI Prior episode of HF 1758 1196 714 775 496 27 ± 5 68 41 44 28 4634 2661 1330 928 394 27 ± 4 57 29 20 9 0.86 < 0.0001 < 0.0001 < 0.0001 < 0.0001 Haemodynamics Systolic blood pressure (mmHg) Heart rate (bpm) LVEF (%) 1758 1758 1758 122.5 ± 17.0 73 ± 12 32.5 ± 6.5 4634 4634 4634 117.7 ± 16.0 75 ± 12 33.5 ± 7.7 < 0.0001 < 0.0001 < 0.0001 Biology Haemoglobin (g/dL) Serum creatinine (mmol/L) 1758 1758 13.3 ± 1.8 104.2 ± 31.7 4634 4634 13.3 ± 1.7 97.6 ± 27.4 0.67 < 0.0001 Treatments Revascularization ACEI ARB Beta-blocker Aspirin Statin 464 1473 72 1281 1519 815 26 84 4 73 86 46 2463 3945 128 3510 4143 2146 53 85 3 76 89 46 < 0.0001 0.18 0.006 0.018 0.0008 0.97 839 48 2365 51 0.018 Study drug Eplerenone ACEI: angiotensin-converting enzyme inhibitor; AMI: acute myocardial infarction; ARB: angiotensin II receptor antagonist; bpm: beats per minute; HF: heart failure; LVEF: left ventricular ejection fraction; NSTEMI: non-ST-segment elevation myocardial infarction; SD: standard deviation; STEMI: ST-segment elevation myocardial infarction. a P value from Mann-Whitney and Chi2 tests for continuous and categorical variables, respectively. Results revascularized. (Table 1). NSTEMI patients received eplerenone Patient characteristics A significant proportion of the patients had NSTEMI (1758 of 6392 patients, 27%). Before matching, compared with STEMI patients, those with NSTEMI came from different regions, were older, were more frequently women and had a higher burden of co-morbidities, such as hypertension, diabetes, prior history of AMI and prior episode of HF (Table 1). NSTEMI patients had a lower heart rate, higher systolic blood pressure and a lower LVEF and more frequently had impaired renal function (Table 1). Concerning therapies, NSTEMI patients less frequently received aspirin and beta-blockers, were more frequently given angiotensin receptor therapy and were far less frequently Outcomes according to ST segment status Over the 30-month follow-up period, compared with STEMI patients, NSTEMI patients experienced more adverse outcomes (all-cause death, 19% vs 13%; cardiovascular death, 16% vs 12%; cardiovascular death/hospitalization, 33% vs 26%; and death from progression of HF, 5% vs 3%) (Table 2). After Cox model PS adjustment without revascularization, NSTEMI status still proved to be a risk factor for all-cause death (HR 1.18, 95% CI 1.03—1.37; P = 0.022), cardiovascular death (HR 1.17, 95% CI 1.00—1.37; P = 0.048) and death from progression of HF (HR 1.36, 95% CI 1.01—1.82; P = 0.042) (Table 3). NSTEMI, eplerenone and outcomes Table 2 153 Outcomes. NSTEMI (na = 1758) All-cause death Cardiovascular death Cardiovascular death or hospitalization Death from progression of HF STEMI (na = 4634) Pb nc % nc % 340 290 583 92 19 16 33 5 621 538 1188 122 13 12 26 3 < 0.0001 < 0.0001 < 0.0001 < 0.0001 HF: heart failure; NSTEMI: non-ST-segment elevation myocardial infarction; STEMI: ST-segment elevation myocardial infarction. a Total frequency. b P value from Chi2 test. c Outcome frequency. After Cox model PS adjustment including revascularization, none of the outcomes differed between STEMI and NSTEMI patients (Table 4). Eplerenone efficacy The beneficial effect of eplerenone was constant among all primary outcomes of interest (Table 5) and was observed whatever the ST segment status (Fig. 1). Table 3 Association of ST-segment status with outcomes (propensity score without revascularization). NSTEMI All-cause death Cardiovascular death Cardiovascular death or hospitalization Death from progression of HF Pa HR (95% CI) 0.022 0.048 0.29 1.18 (1.03—1.37) 1.17 (1.00—1.37) 1.06 (0.95—1.18) 0.042 1.36 (1.01—1.82) CI: confidence interval; HF: heart failure; HR: hazard ratio; NSTEMI: non-ST-segment elevation myocardial infarction. a P value from Cox regression. Table 4 Association of ST-segment status with outcomes (propensity score with revascularization). Discussion To our knowledge, this study is the first to focus on the prognostic differences between NSTEMI and STEMI specifically in patients with systolic acute HF complicating AMI, a subset of patients at the highest risk of short- and long-term death [5,6,8]. Consistent with the main findings of previous reports in non-HF patients [8,10,13,16,17], worse outcomes associated with NSTEMI could mainly be explained by more frequent co-morbidities, less aggressive therapies and, most importantly, less frequent revascularization. A second major finding of our analysis is that eplerenone improved outcomes in both STEMI and NSTEMI patients. Although STEMI and NSTEMI go through the same pathophysiological process, namely acute atherothrombosis [18—20], there are differences between the two presentations. STEMI is the consequence of complete thrombotic occlusion of a major coronary artery, mainly by plaque disruption [21], whereas NSTEMI is a subtotal coronary occlusion, mainly by plaque erosion [22]. Thrombus is described as fibrin rich in STEMI and platelet rich in NSTEMI. Thrombotic load is often higher in STEMI than in NSTEMI [23,24]. Regarding HF, myocyte loss leading to acute contractile dysfunction is not the only mechanism leading to acute HF in acute coronary syndrome (ACS) patients, as the GRACE registry showed that 11.2% of patients with unstable angina also showed signs of HF [3]. Thus, myocardial stunning/hibernation [6], ventricular remodelling, acute mitral regurgitation and ischaemia-induced impairment in Table 5 Association of study drug with outcomes. NSTEMI P All-cause death Cardiovascular death Cardiovascular death or hospitalization Death from progression of HF a Eplerenone HR (95% CI) 0.28 0.45 0.79 1.08 (0.94—1.25) 1.06 (0.91—1.24) 1.02 (0.91—1.13) 0.15 1.25 (0.93—1.68) CI: confidence interval; HF: heart failure; HR: hazard ratio; NSTEMI: non-ST-segment elevation myocardial infarction. a P value from Cox regression. All-cause death Cardiovascular death Cardiovascular death or hospitalization Death from progression of HF Pa HR (IQR) 0.004 0.003 0.004 0.83 (0.73—0.94) 0.81 (0.71—0.93) 0.87 (0.79—0.96) 0.049 0.76 (0.58—1.00) HF: heart failure; HR: hazard ratio; IQR: interquartile range. a P value from Cox regression. 154 Figure 1. S. Carillo et al. Association of eplerenone with outcomes according to ST-segment status. myocardial relaxation [5] have been reported to cause HF in acute ischaemic conditions. Poor prognosis of post-AMI patients with acute systolic HF HF complicating AMI is known to increase cardiovascular risk in equal proportions among STEMI and NSTEMI patients, while HF AMI patients are known to benefit from revascularization less frequently than non-HF patients [3]. In the GRACE [3], NRMI-2 [8], Euro Heart Survey [11] and Gulf RACE [25] registries, conducted in unselected ACS patients, the death rate in patients with HF was 2—4 times higher than in those without HF. Our results obtained in acute systolic HF patients show once again that acute HF seriously compounds the prognosis of AMI patients and illustrates very well the concept of ‘‘deadly intersection’’ between ACS and HF mentioned by Velasquez and Pfeffer [5]. Acute clinical HF and LVSD are two phenomena that do not necessarily co-exist in post-AMI patients. Indeed, in the SAVE study [26], 60% of LVSD patients showed no HF, whereas in the VALIANT study [27], 42% of patients with acute HF did not have LVSD. In our study, post-AMI patients with both clinical signs of HF and LVSD were enrolled, thus we targeted the highest risk patients. As could be expected, the prognosis of our post-AMI patients with acute systolic HF was very poor, with a 19%rate of all-cause death for NSTEMI patients and a 16%-rate for STEMI patients over the 2.5-year follow-up period. The majority of these deaths were due to cardiovascular causes. Given that the patients in our study had a poor outcome, we must wonder about the medical and reperfusion therapies that could have improved their prognosis. Concerning medical therapies, both our NSTEMI and STEMI groups were quite adequately treated, in compliance with the guidelines at the time of the study: 73—86% were treated with beta-blockers, angiotensin-converting enzyme inhibitors and aspirin. The relatively low use of statins is consistent with their low level of evidence in post-AMI HF patients at the time of the trial. Indeed, so far, all statin trials in ACS patients have excluded those with HF and/or LVSD. Although at the time of the study NSTEMI and STEMI with HF were both a class 1 indication for urgent revascularization [28,29], only 26% and 53%, respectively, received NSTEMI, eplerenone and outcomes reperfusion therapy — a low rate in line with a worldwide study and with clinical practice in the early 2000s [13,30]. The recent spread of reperfusion therapies is the main factor associated with the recent improvement in outcomes among AMI patients [2]. In comparison, the latest registry in Europe has shown that 90% of STEMI patients and 70% of NSTEMI patients benefit from revascularization nowadays [31]. Consequently, more frequent use of reperfusion therapies among our high-risk AMI HF patients would have improved outcome in both our NSTEMI and STEMI subgroups. Differences between NSTEMI and STEMI among HF patients Although in unselected ACS patients NSTEMI is as common as STEMI [11], our study enrolled fewer NSTEMI patients than STEMI patients, probably because of the per-protocol selection criterion of LVSD and HF, which is indeed more frequent in STEMI patients [9,12,13]. Previous studies have already shown that although NSTEMI causes less severe ischaemia and myocardial damage, it is usually associated with a worse outcome than STEMI [10,12,13]; a combination of five factors may account for this. First, as shown in Tables 1 and 4, revascularization is the most discriminating factor between STEMI-HF and NSTEMIHF patients, with twice as many reperfusion therapies in STEMI patients. Indeed, our analysis showed that the prognostic difference between the two groups was no longer statistically significant when revascularization was taken into account in the adjustment strategy. However, even if NSTEMI patients benefit more frequently from revascularization nowadays, they still are more unlikely to be reperfused than STEMI patients (70% vs 90%) [31]. This persistent difference is probably due to a combination of technical and individual factors. Indeed, a significant proportion of NSTEMI patients are not technically suitable for revascularization, as they more frequently present a diffuse coronary disease with fewer fresh thrombi and more calcified lesions than STEMI patients. Moreover, NSTEMI patients are still less frequently revascularized than STEMI patients because of a perceived lower benefit in such patients. A more frequent use of revascularization among our specific very-high-risk NSTEMI-HF patients at the time of the study might have improved their prognosis [2] and decreased the difference in outcomes between NSTEMI and STEMI. Second, due to study design, patients who died within 3 days after AMI (i.e. before enrolment in the trial) were not included in our study. Unlike NSTEMI patients, > 50% of deaths in STEMI patients occur very early after the onset of symptoms, especially during the first 2 hours [33]. The selection bias related to enrolment time might have underestimated the mortality rate in the STEMI subgroup, which partly explains the mortality difference between NSTEMI and STEMI patients in our report. Third, our NSTEMI patients were less likely to receive appropriate medical therapies, such as aspirin and betablockers, when hospitalized for AMI. This less rigorous medical treatment of NSTEMI patients has been consistently reported in previous studies as a factor that might explain their worse prognosis compared with STEMI patients [34]. 155 Fourth, compared with STEMI patients, those with NSTEMI had a greater burden of co-morbidities, such as old age, diabetes and hypertension. Studies carried out regardless of HF status, such as EHS-ACS II [11] and the series reported by Terkelsen et al. [13], came to strictly similar findings. Fifth, compared with STEMI patients, our NSTEMI patients were three times more likely to have a history of HF, a condition that is known to triple the long-term risk of death after myocardial infarction [13] and inevitably affected the prognosis of NSTEMI patients in our series. Consequently, as can be seen in unselected AMI patients [35], it seems that the poor long-term outcome in our NSTEMI-HF patients can be explained by more frequent co-morbidities and less aggressive treatment (mainly less frequent revascularization), rather than by the type of acute ST-segment variation per se. Thus, the imbalances in baseline characteristics mentioned above account for the less favourable unadjusted prognosis among NSTEMI patients, as illustrated by the results of our PS-matching analysis, which abolished all differences in primary outcomes between NSTEMI and STEMI patients. Eplerenone efficiency In the EPHESUS study, eplerenone benefited patients with NSTEMI and STEMI equally. Indeed, whatever the ST-segment status, high-risk AMI survivors with LVSD or HF, receiving optimal treatment with angiotensin-converting enzyme inhibitors or angiotensin receptor blockers and a betablocker benefit from further neurohormonal blockade with eplerenone. Although post hoc, this new subgroup analysis extends the findings of previous reports of prespecified or post hoc subgroup analyses, such as diabetics [36], hypertensives [37] and patients with LVEF < 30% [38], which consistently showed a marked clinical benefit for eplerenone across a variety of AMI presentations. Study limitations Several limitations to our study must be acknowledged. Baseline electrocardiographical findings of STEMI or NSTEMI were reported by investigators and were not centrally adjudicated, therefore misclassification is possible. It is also possible that patients with STEMI developed NSTEMI, or vice versa, during follow-up. However, this phenomenon, also known as regression dilution, is known to underestimate true associations [39]. Based on pathophysiological hypothesis and prognostic literature data, we selected 20 baseline characteristics that differed most between the two groups to run our PS adjustment. Using all available characteristics would have eliminated all identifiable baseline confounders, but would have seriously lowered the power of our analysis. A sensitivity analysis using PS-matching all 64 available baseline variables yielded similar results. We had no data on death during the first 48 hours nor on delay to reperfusion after index AMI. These data would have helped us to better fine-tune the difference in prognosis between NSTEMI and STEMI. 156 Conclusion In conclusion, as far as we know, our study is the first report comparing outcomes and eplerenone efficiency among postAMI acute systolic HF patients with STEMI and NSTEMI. The study shows that in that specific high-risk populations, NSTEMI remains a useful marker for identifying a group of patients with more adverse long-term outcomes. Among those patients, eplerenone improves outcomes equally in STEMI patients and NSTEMI patients. However, because NSTEMI carries a worse prognosis, additional therapeutic interventions must be carried out in such high-risk LVSD patients, including more aggressive medical therapies and more frequent revascularization. Disclosure of interest Sylvain Carillo, Renaud Fay and Mickael Angioi: none. Yan Zhang: affiliation with UAB. John Vincent and Santosh C. Sutradhor: Pfizer Inc. employees. Ali Ahmed: affiliation with UAB and VA. Bertram Pitt: consultant for Pfizer, Merck, Novartis, Bayer, Takeda, AstraZeneca, Lilly, BMS, BG Medicine (stock options), Relypsa (stock options), Cytopherx, Amorcyte, Aurasence (stock options) and Ardelyx; grants from Novartis, Medtronic and Forrest Laboratories. Faiez Zannad: grants to institution from BG Medicine and Roche Diagnostics; consultant/member of steering committees, event committees and data safety monitoring boards for Bayer, Biomérieux, Biotronik, BostonScientific, CVCT, Novartis, Pfizer, Resmed, Servier and Takeda. References [1] Chin CT, Chen AY, Wang TY, et al. Risk adjustment for in-hospital mortality of contemporary patients with acute myocardial infarction: the acute coronary treatment and intervention outcomes network (ACTION) registry-get with the guidelines (GWTG) acute myocardial infarction mortality model and risk score. Am Heart J 2011;161:113e2—22e2. [2] Fox KA, Steg PG, Eagle KA, et al. Decline in rates of death and heart failure in acute coronary syndromes, 1999—2006. JAMA 2007;297:1892—900. [3] Steg PG, Dabbous OH, Feldman LJ, et al. Determinants and prognostic impact of heart failure complicating acute coronary syndromes: observations from the Global registry of acute coronary events (GRACE). Circulation 2004;109:494—9. [4] Steg PG, Kerner A, Van de Werf F, et al. Impact of in-hospital revascularization on survival in patients with non-ST-elevation acute coronary syndrome and congestive heart failure. Circulation 2008;118:1163—71. [5] Velazquez EJ, Pfeffer MA. Acute heart failure complicating acute coronary syndromes: a deadly intersection. Circulation 2004;109:440—2. [6] Weir RA, McMurray JJ, Velazquez EJ. Epidemiology of heart failure and left ventricular systolic dysfunction after acute myocardial infarction: prevalence, clinical characteristics, and prognostic importance. Am J Cardiol 2006;97:13F—25F. [7] Velazquez EJ, Francis GS, Armstrong PW, et al. An international perspective on heart failure and left ventricular systolic dysfunction complicating myocardial infarction: the VALIANT registry. Eur Heart J 2004;25:1911—9. S. Carillo et al. [8] Wu AH, Parsons L, Every NR, et al. Hospital outcomes in patients presenting with congestive heart failure complicating acute myocardial infarction: a report from the Second National registry of myocardial infarction (NRMI-2). J Am Coll Cardiol 2002;40:1389—94. [9] Abbott JD, Ahmed HN, Vlachos HA, et al. Comparison of outcome in patients with ST-elevation versus non-ST-elevation acute myocardial infarction treated with percutaneous coronary intervention (from the National Heart Lung, and Blood Institute Dynamic Registry). Am J Cardiol 2007;100:190—5. [10] Fox KA, Carruthers KF, Dunbar DR, et al. Underestimated and under-recognized: the late consequences of acute coronary syndrome (GRACE UK-Belgian Study). Eur Heart J 2010;31:2755—64. [11] Mandelzweig L, Battler A, Boyko V, et al. The second Euro Heart Survey on acute coronary syndromes: characteristics, treatment, and outcome of patients with ACS in Europe and the Mediterranean basin in 2004. Eur Heart J 2006;27:2285—93. [12] Goodman D, Huang W, Gore JM, et al.The late consequences of acute coronary syndromes: 2-year follow-up outcomes, procedures and treatment of patients from the Global Registry of Acute Coronary Events (GRACE). Abstract 3963. 2011 [Available at: http://spo.escardio.org/abstract-book/ presentation.aspx?id=99444]. [13] Terkelsen CJ, Lassen JF, Norgaard BL, et al. Mortality rates in patients with ST-elevation vs. non-ST-elevation acute myocardial infarction: observations from an unselected cohort. Eur Heart J 2005;26:18—26. [14] Cohn JN, Colucci W. Cardiovascular effects of aldosterone and post-acute myocardial infarction pathophysiology. Am J Cardiol 2006;97:4F—12F. [15] Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 2003;348:1309—21. [16] Fox KA, Clayton TC, Damman P, et al. Long-term outcome of a routine versus selective invasive strategy in patients with nonST-segment elevation acute coronary syndrome a meta-analysis of individual patient data. J Am Coll Cardiol 2010;55:2435—45. [17] O’Donoghue M, Boden WE, Braunwald E, et al. Early invasive vs conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction: a meta-analysis. JAMA 2008;300:71—80. [18] Davies MJ. Acute coronary thrombosis — the role of plaque disruption and its initiation and prevention. Eur Heart J 1995;16(suppl. L):3—7, http://dx.doi.org/10.1093/eurheartj/ 16.suppl L.3. [19] Davies MJ. The composition of coronary-artery plaques. N Engl J Med 1997;336:1312—4. [20] Davies MJ, Richardson PD, Woolf N, et al. Risk of thrombosis in human atherosclerotic plaques: role of extracellular lipid, macrophage, and smooth muscle cell content. Br Heart J 1993;69:377—81. [21] Van de Werf F, Bax J, Betriu A, et al. Management of acute myocardial infarction in patients presenting with persistent STsegment elevation: the task force on the management of STsegment elevation acute myocardial infarction of the European Society of Cardiology. Eur Heart J 2008;29:2909—45. [22] Bassand JP, Hamm CW, Ardissino D, et al. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. Eur Heart J 2007;28:1598—660. [23] Goto K, Lansky AJ, Nikolsky E, et al. Prognostic significance of coronary thrombus in patients undergoing percutaneous coronary intervention for acute coronary syndromes: a subanalysis of the ACUITY (Acute Catheterization and Urgent Intervention Triage strategY) trial. JACC Cardiovasc Interv 2011;4:769—77. [24] Svilaas T, Vlaar PJ, van der Horst IC, et al. Thrombus aspiration during primary percutaneous coronary intervention. N Engl J Med 2008;358:557—67. NSTEMI, eplerenone and outcomes [25] Alsheikh-Ali AA, Al-Mallah MH, Al-Mahmeed W, et al. Heart failure in patients hospitalized with acute coronary syndromes: observations from the Gulf Registry of Acute Coronary Events (Gulf RACE). Eur J Heart Fail 2009;11:1135—42. [26] Pfeffer MA, Braunwald E, Moye LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med 1992;327:669—77. [27] Velazquez EJ, Pfeffer MA, McMurray JV, et al. VALsartan In Acute myocardial iNfarcTion (VALIANT) trial: baseline characteristics in context. Eur J Heart Fail 2003;5:537—44. [28] Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: executive summary and recommendations. A report of the American College of Cardiology/American Heart Association task force on practice guidelines (committee on the management of patients with unstable angina). Circulation 2000;102: 1193—209. [29] Ryan TJ, Antman EM, Brooks NH, et al. 1999 update: ACC/AHA guidelines for the management of patients with acute myocardial infarction. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Acute Myocardial Infarction). J Am Coll Cardiol 1999;34:890—911. [30] Hasdai D, Behar S, Wallentin L, et al. A prospective survey of the characteristics, treatments and outcomes of patients with acute coronary syndromes in Europe and the Mediterranean basin; the Euro heart survey of acute coronary syndromes (Euro Heart Survey ACS). Eur Heart J 2002;23:1190—201. 157 [31] Nieminen MS, Brutsaert D, Dickstein K, et al. EuroHeart failure survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J 2006;27:2725—36. [33] Tunstall-Pedoe H, Kuulasmaa K, Mahonen M, et al. Contribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA project populations. Monitoring trends and determinants in cardiovascular disease. Lancet 1999;353:1547—57. [34] Rogers WJ, Frederick PD, Stoehr E, et al. Trends in presenting characteristics and hospital mortality among patients with ST elevation and non-ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J 2008;156:1026—34. [35] Setoguchi S, Glynn RJ, Avorn J, et al. Improvements in longterm mortality after myocardial infarction and increased use of cardiovascular drugs after discharge: a 10-year trend analysis. J Am Coll Cardiol 2008;51:1247—54. [36] O’Keefe JH, Abuissa H, Pitt B. Eplerenone improves prognosis in postmyocardial infarction diabetic patients with heart failure: results from EPHESUS. Diabetes Obes Metab 2008;10:492—7. [37] Pitt B, Ahmed A, Love TE, et al. History of hypertension and eplerenone in patients with acute myocardial infarction complicated by heart failure. Hypertension 2008;52:271—8. [38] Pitt B, Gheorghiade M, Zannad F, et al. Evaluation of eplerenone in the subgroup of EPHESUS patients with baseline left ventricular ejection fraction < or = 30%. Eur J Heart Fail 2006;8:295—301. [39] Clarke R, Shipley M, Lewington S, et al. Underestimation of risk associations due to regression dilution in long-term follow-up of prospective studies. Am J Epidemiol 1999;150:341—53.