Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
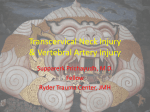
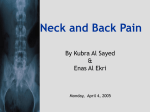
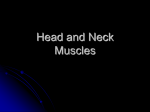
Be familiar with the mechanism of a instability / traumatic syndrome. To be familiar with the clinical presentation of a typical patient with acute instability syndrome. Be familiar with the most widely used medical as well as physiotherapy treatment protocols for a patient with a typical acute / sub-acute and chronic instability syndrome. Be familiar with the possible pathological changes associated with an instability syndrome. Be familiar with the clinical presentation of a typical patient with an instability syndrome. Be familiar with the associated symptoms experienced by a patient with a typical instability syndrome. Trauma as a result of a motor-vehicle accident or sport injury Degenerative in the articular complex Leads to irregular patterns of comparable signs and a variety of signs and symptoms Acceleration when a car is hit from behind The seat with the lower body accelerates forwards The neck is unstable and can not control the movement of the head The neck moves into sudden extension – reflex contraction of the neck flexors causes the neck to go into flexion Deceleration when a car is brought to a stand still due to the collision Head and neck continues to move forwards causing hyperflexion until the chin bumps against the chest Reflex contraction of the extensors causes extension If the neck is rotated when the collusion occurs an excessive amount of lateral flexion and rotation will take place Normal physiological ranges is exceeded and this leads to damage and anatomical changes of the soft tissue Ligaments Intervertebral disc Facet joints Surrounding muscles Haematoma of especially the m sternocleidomastoïd Pain during rest especially if the structures are placed on stretch Pain through entire range of movement Muscles are painful during stretch and contraction Ligaments are painful when placed on stretch (except the interspinal ligament which is painful during extension) Total bed-rest for first 2-3 days Supportive, soft neck support (when patient is in an upright position) Ice for first 24 hours Heat is contra-indicated for first 48 hours (Afterwards damp heat) Anti-inflammatory medication and muscle relaxants Careful, active non-weight bearing exercises (except rotation and lateral flexion) Gentle massage Symptoms become more specific Wean from neck support – still use support in a vehicle of when neck feels tired Ultrasound and damp heat/ice Mobilisations – short of pain Cautious isometric exercises Increase active exercises (introduce flexion and extension into exercise programme) Commence with PNF patterns if pain will allow Cautiously commence with distal neural mobilisations Treat according to signs and symptoms Pain at end of range (6-8 weeks after injury) Totally wean from neck support Isometric exercises are progressed into standing Evaluate for muscle imbalance and treat accordingly Make use of combined movements and neural mobilisation techniques for final rehabilitation Ligament injuries: Anterior longitudinal Posterior longitudinal Interspinal Disc herniation Fracture : Spinous process Vertebral bodies Tear of the capsule and facet joints with acute synovitis Tear of the neck muscles Tempomandibular joint injuries Retropharingeal heamatoma Oesophageal haemorrhage Sympatic chain injuries Concussion and minor head injuries Vertebral artery damage Thoracic outlet syndrome Pain and tenderness over affected structures Referred pain – irritation of nerve root miofascial trigger points scleretome referral (deep burning pain which feels like it is in the bone itself) Neck muscle spasm Headaches (experienced as a deep pressure with pounding , nausea , vomiting and photophobia) Normal range of movement restricted Dysphagia with hoarseness in the acute phase Sympathetic signs: Intermittent weak vision Headaches Horner’s syndrome Dizziness: Vertebral artery symptoms Middle ear injuries Oedema Miosis (constriction of the pupil) Pytosis (drooping eye) Enophthalmia (sunken eye) Anidosis (loss of perspiration on the one side of the face) Anterior chest pain: presents as angina becomes worse with exercise tender anterior nausea sleeps poorly becomes worse with coughing and sneezing Oedema Thoracic outlet syndrome Lower backache Head injuries such as concussion Tempromandibular joint injuries Fibromialgia (chronic pain and stiffness in muscles with local tenderness) Psychosis Depression Difficulty with acceptance Anxiety Rage Frustration (financial and family) Personality changes and interference in daily living Post-traumatic stress syndrome Analgesics Anti-depressants Surgery Psychiatric treatment