Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
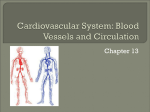
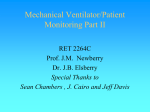
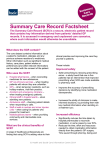
‘DEEP DIVE’ on HYPERTENSION FOR THE ARTERIAL LOCALITY A Joint Strategic Needs Assessment (JSNA) Product August 2012 Essex County Council Public Health Team Report Author: Ian Wake, Consultant in Public Health for Basildon and Brentwood CCG Project Team: Ian Wake, Consultant in Public Health Emma Sanford, Epidemiologist Tom Fowler, Senior Public Health Information Analyst Niall McDougall, Public Health Manager 1 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG Contents 1. INTRODUCTION ................................................................................................................................................... 3 2. BACKGROUND ..................................................................................................................................................... 3 3. CASE FINDING AND CLINICAL MANAGEMENT OF HYPERTENSION ..................................................................... 4 4. NATIONAL INSTITUTE OF CLINICAL EXCELLENCE (NICE) GUIDELINES ON HYPERTENSION PRESCRIBING ........... 8 5. THE IMPACT ON SECONDARY CARE COSTS OF PRESCRIBING COMBINED WITH IMPROVED CASE FINDING OF HYPERTENSIVE PATIENTS................................................................................................................................... 11 6. DISCUSSION, CONCLUSIONS and RECOMMENDATIONS ................................................................................... 14 2 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG ‘DEEP DIVE’ REPORT FOR HYPERTENSION WITHIN THE ARTERIAL LOCALITY 1. INTRODUCTION This report details a ‘deep dive’ exercise undertaken by the Essex County Council Public Health Team on behalf on the Basildon and Brentwood Clinical Commissioning Group (CCG) on the issue of Hypertension within the Arterial Locality. The report examines case finding, clinical management and emergency admission rates of Hypertension at locality and practice level. It also considers potential prescribing and secondary care events savings that could be made by the Arterial locality and its practices if the latest National Institute of Clinical Excellence (NICE) guidance (CG127) were followed by all practices, and case finding were increased to different levels. A more comprehensive report detailing the Deep Dive across all CCG localities can be accessed at www.essexinsight.org.uk. The report is under the ‘Themes’ and the ‘Health and Wellbeing’ sections. 2. BACKGROUND The JSNA CCG profiles for Basildon and Brentwood identified five key clinical priority areas for the CCG in terms of commissioning and QIPP; Circulatory Disease, Respiratory Disease, Diabetes, Lung Cancer and Lifestyles. At £180 per head of weighted population, Circulatory Disease is the programme that has the highest spend per head in NHS South West Essex (data not currently available at a level lower than PCT level), and spend is also significantly greater than the PCT’s Office for National Statistics (ONS) cluster, making it a key QIPP priority. (Figure 2.1). Figure 2.1 Programme budgeting spend on problems of circulation All PCT s expenditure per 100,000 population Programme category ONS Cluster level Primary Care Trust Population w eighting Care Setting Benchmark 1st quintile 2nd quintile 3rd quintile 4th quintile 5th quintile South West Essex Teac hing PCT PCTs within se lec ted cluste r level National average 10.0 5.0 West Essex PCT Sw indon PCT Havering PCT Peterborough PCT Bexley PCT 15.0 Medw ay Teaching PCT 20.0 Milton Keynes PCT Expenditure (£million per 100,000 population) 25.0 South West Essex Teaching PCT Note on interpretation: PCTs with large amounts of expenditure in category 23x for a given care setting may have less expenditure allocated to disease specific categories within that care setting. To aid comparison of expenditure on disease specific categories and within care settings the ‘All commissioner chart with 23x’ sheet shows the same information as the chart below with additional information on the amount of expenditure in 23x for the chosen care setting on the negative y axis. Notes on intepretation of data: budgeting returns to the Department of Health f or 2010/2011. services purchased f rom healthcare providers. PCTs f ollow st procedures and mappings w hen calculating programme budge or services can be classif ied directly to a programme budgetin setting. When it is not possible to reasonably estimate a progr category, expenditure is classif ied as ‘Other: Miscellaneous’. T expenditure to programme budgeting subcategories is not alw and subcategory level data should theref ore be used w ith cau be reasonably estimated at disease specif ic level, and is sepa subcategory of ‘Other’ expenditure. attendances a national split has been applied to PCT total A& apportion it across programme budgeting categories. f irst time in 2010/11. For this reason, programme budgeting da care settings should be interpreted w ith caution. to make direct comparisons w ith programme budgeting data f r 0.0 National Rank Lowest to Highest If the PCT (or the two CCGs within it) were to reduce spend on the Circulatory Disease programme so that it were in line with the ONS Cluster Average a potential QIPP saving of £11,847,304 would be released that could be reinvested into other areas of patient care. 3 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG The Circulatory System Programme Budgeting category covers all areas of Cardio-Vascular Disease (CVD), including hypertension and is closely linked to the programme covering Endocrine, nutritional and metabolic diseases (in relation to diabetes and blood lipids as risk factors). However, a separate ‘deep dive’ has been agreed for Diabetes, and this condition is not therefore covered in this report. 3. Case Finding and Clinical Management of Hypertension The clinical management of hypertension is one of the most common interventions in primary care, accounting for approximately £1 billion in drug costs alone in 2006. Although the earlier identification of patients at risk of Hypertension will further contribute to the rising circulatory diseases prevalence, early clinical intervention and good clinical management of patients with hypertension will reduce the incidence of more serious circulatory disease and overall healthcare costs associated with it. Figure3.1 identified inadequate case finding of patients with Hypertension as all but one practice fall below the 3SD line. Case finding ranges between 44.8% and 110.5% of expected numbers of hypertensives. Figure 3.1. Observed vs. Expected funnel plots for hypertension for all practices in the Arterial Locality Figures 3.2 and 3.3 show funnel plots for the two QOF clinical management indicators for hypertension at BBCCG practice level; BP4 – The Percentage of Patients with Hypertension for whom there is a record of blood pressure within the preceding 9 months and BP5 – The Percentage of Patients with Hypertension in whom the last blood pressure reading (measured in the preceding nine months) was 150/90 or less. Figure 3.2 Funnel Plot of QOF indicator BP4 The solid horizontal line in both figure 3.2 and 3.3 funnel plots represents the performance of the poorest performing PCT in the top quintile of performers in England. Whilst it could be argued that performance at this level is a challenging target for the CCG, achieving the aspiration of being in the top quintile of performance in the county across all areas of clinical practice will impact positively on secondary care costs and patient care quality. Six of the Arterial Locality practices fall within the 2SD funnels for the QOF indicator BP4 (figure 3.3) suggesting that the aspiration to perform within England’s top quintile is achievable and that almost half of all of the locality’s practices are reaching this excellent level of performance. The remaining seven fall below the 3SD funnel line suggesting considerable scope for improving blood pressure monitoring for patients on the hypertension register across the locality 4 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG Figure 3.3 Funnel Plot of QOF indicator BP5 For QOF indicator BP5, performance across the locality is largely excellent. Seven practices fall above lower 2SD line suggesting that their performance on this indicator falls within the top quintile of practices in England. A further three fall above the 2SD line, suggesting performance is significantly better than the poorest performer in the top quintile in England. However five practices fall below the 2SD line suggesting scope for improvement. Figure 3.4 Funnel Plot of non elective admissions rate Figure 3.4 shows a funnel plot of non-elective admissions per 100 on the hypertension register for each CCG practice. The mean emergency admission rate per 100 hypertensive patients for the BBCCG has been used in figure 3.4. This mean is less than that for England and the East of England and so represents a good clinical quality marker. All practices fall below the upper 2SD funnel showing that no practice within the locality has an emergency admission rate due to hypertension that is significantly greater than the CCG mean or that for either England or the East of England. This is clearly very positive. It is however worth noting that the funnels themselves are wide, due to the relatively small number of emergency admissions per practice, which generate large statistical confidence intervals. It is also worth remembering that inadequate case finding and/or clinical management of hypertension is likely to drive emergency admissions of other circulatory diseases. Table 1 summarises the results of this section by practice and makes recommendations for action at practice level. 5 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG Table 1: Summary of Results on Case Finding and Clinical Management of Patients with Hypertension by Practice F code F81104 Practice Dr. R. Rasheed Obs / Expected 0.64 Low(0.001) BP4 Conclusion 74.59 Low (0.001) 95.61 In top performing quintile in England 1.24 No sig. diff. to CCG mean 79.08 Low (0.001) 1.86 No sig. diff. to CCG mean 1 Ineffective Case Finding 81.67 Low (0.025) 1.87 No sig. diff. to CCG mean 1 Ineffective Case Finding 1.64 No sig. diff. to CCG mean 3 Low Underlying Risk 2.02 No sig. diff. to CCG mean 1 Ineffective Case Finding 3.54 No sig. diff. to CCG mean 1 Ineffective Case Finding F81080 Dr. H.J.Cockcroft and Partners 0.56 Low(0.001) 91.73 Low (0.001) 94.05 In top performing quintile in England 88.94 Low (0.001) 74.68 Low (0.001) F81045 Dr. C.P. Gupta 0.45 Low(0.001) 86.36 Low (0.001) Low Underlying Risk 87.86 In top performing quintile in England 91.36 Low(0.001) 3 1.36 Low(0.001) 0.64 1.Improve Case Finding 2.Improve monitoring of patients with Hypertension 3. Query Clinical Management 67.18 0.54 F81222 3 Low Underlying Risk No sig. diff. to CCG mean F81013 Dr. R Dasgupta Conclusions / Recommendations Low (0.001) Low (0.001) Low(0.001) Hypertension Quadrant on Boston Chart and meaning BP5 Conclusion Dr. A. Afifi and Partners 0.82 Non elective admissions per 100 on disease register conclusion BP5 Dr. J.O. Araymoi F81651 Low(0.001) BP4 Y00758 Dr. Sarfraz M U H & Partner 0.70 Obs / Expected Conclusion Nonelective admissions per 100 on disease register 85.95 82.37 In top performing quintile in England In top performing quintile in England F81150 Dr. A.J. Mitchell & Partner 0.54 Low(0.001) 91.44 Low (0.001) 80.43 Low (0.001) 2.51 No sig. diff. to CCG mean 1 Ineffective Case Finding F81151 Dipple Medical Centre 0.76 Low(0.001) 81.15 Low (0.001) 65.14 Low (0.001) 1.76 No sig. diff. to CCG mean 3 Low Underlying Risk 95.31 In top performing quintile in England 88.52 High (0.001) 1.85 No sig. diff. to CCG mean 4 Effective Case Finding, Well Managed Y00469 Dr. M. Sims 6 1.11 High(0.001) ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG 1.Improve Case Finding 1.Improve Case Finding 2.Improve monitoring of patients with Hypertension 3. Query Clinical Management 1.Improve Case Finding 2.Improve monitoring of patients with Hypertension 3. Query Clinical Management 1.Improve Case Finding 1.Improve Case Finding 2.Improve monitoring of patients with Hypertension 1.Improve Case Finding 2.Improve monitoring of patients with Hypertension 3. Query Clinical Management 1.Improve Case Finding 2.Improve monitoring of patients with Hypertension 3. Query Clinical Management 1.Improve Case Finding 2.Improve monitoring of patients with Hypertension 3. Query Clinical Management No action needed F code F81158 F81648 F81711 Practice Dr. T.F. Nasah Dr. H.U. Din Dr. A.J.L. Holman 7 Obs / Expected Obs / Expected Conclusion BP4 0.48 Low(0.001) 95.69 0.78 Low(0.001) 94.14 0.66 Low(0.001) 94.75 BP4 Conclusion In top performing quintile in England In top performing quintile in England In top performing quintile in England Non elective admissions per 100 on disease register conclusion Hypertension Quadrant on Boston Chart and meaning BP5 BP5 Conclusion Nonelective admissions per 100 on disease register 90.30 High (0.001) 3.20 No sig. diff. to CCG mean 1 Ineffective Case Finding 92.33 High (0.001) 2.66 No sig. diff. to CCG mean 1 Ineffective Case Finding In top performing quintile in England 3.49 No sig. diff. to CCG mean 1 83.18 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG Ineffective Case Finding Conclusions / Recommendations 1.Improve Case Finding 1.Improve Case Finding 1.Improve Case Finding 4. National Institute of Health and Clinical Excellence (NICE) Guidelines on Hypertension Prescribing NICE Guidance of Hypertension (CG127) sets out an antihypertensive drug treatment schedule based on the latest evidence of best of practice (figure 3.5) http://guidance.nice.org.uk/CG127/NICEGuidance/doc Figure 3.5 Summary of antihypertensive drug treatment schedule Aged over 55 years or black person of African or Caribbean family origin of any age Aged under 55 years First Line 41% of cohort Key A or B 70% or 30% C A – ACE inhibitor Rampril £20.98 Second Line 41% of cohort B- Angiotensin II receptor blocker (ARB)12 (A or B) + C Losartan (generic) £15.00 Candesartan £165 (off patent next 6 months) Third Line 18% of cohort (Aor B) + C + D C – Calcium-channel blocker (CCB)13 Amlodipine £13.00 D – Thiazide-like diuretic Resistant hypertension A + C + D + consider further diuretic beta-blocker16 14, 15 Consider seeking expert advice or alpha- or Indapamide 1.5mg modified release £44.50 Indapamide 2.5mg £13.80 12 Choose a low-cost ARB. A CCB is preferred but consider a thiazide-like diuretic if a CCB is not tolerated or the person has oedema, evidence of heart failure or a high risk of heart failure. 14 Consider a low dose of spironolactone 15 or higher doses of a thiazide-like diuretic. 15 At the time of publication (August 2011), spironolactone did not have a UK marketing authorisation for this indication. Informed consent should be obtained and documented. 16 Consider an alpha- or beta-blocker if further diuretic therapy is not tolerated, or is contraindicated or ineffective . 13 8 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG The NICE costing template for Hypertension suggests that of the cohort of patients who are hypertensive and do not have Heart Failure, 41% should be on first line treatment, 41% on second line treatment and 18% on third line treatment.1Fourth line treatment is not used within the model as numbers are likely to be very small. This is shown in figure 3.5 above. Figure 3.5 also shows the costs of the most cost effective anti-hypertensive drugs to be used at each stage of the prescribing pathway. Public Health have compared the prescribing behaviour of practices within the BBCCG against that recommended in the NICE prescribing pathway (figure 3.5), to ascertain the potential for cost savings and improved patient outcomes. By running SystmOne reports remotely, we have extracted the number of patients on each CCG Practice’s Hypertension register who are not on the Heart Failure register. Heart Failure patients have been excluded as they are also likely to be being prescribed and ACE inhibitor or ARB, which feature in in the pathway. Through liaison with the PCT’s Medicines Management Team, we have also obtained the total current annual prescribing cost for each CCG practice resulting from patients with Hypertension who do not have heart failure. We then calculated the expected prescribing cost for the number of Hypertensive patients who do not have heart failure by practice, if NICE prescribing guidance were being followed, and the most cost effective drugs were being used, making the assumption suggested by NICE that 41% of patients should be on first line treatment, 41% on second line and 18% on third line treatment. We also obtained the percentage of Hypertensive patients under 55 on each practice register and applied this to our model. Using this model, we are able to calculate the total potential cost saving (or increase) if each practice within the CCG were to follow NICE prescribing guidance and prescribe the most cost effective hypertensive drugs. We appreciate that this is a theoretical model and there may be good clinical reasons in some cases why a GP may decide to adopt a slightly different prescribing regime. Savings are also not necessarily immediate as they will require GP practice time to review patients’ current drug regimens with a view to a potential change. Table 2 summarises the results for each practice within the Arterial Locality. As Table 2 shows, there is a potential for the Arterial Locality to save almost £589K by changing prescribing of anti-hypertensive drugs to meet NICE guidelines and using the most cost effective drugs. 1 NICE Guidance CG127 Costing Template 9 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG Table 2 Potential Savings in Prescribing Costs using NICE prescribing guidelines – Arterial Locality Practice Current Prescribing Prescribing Cost Potential for Savings Costs if NICE guidance in Prescribing followed Potential for Savings in Prescribing per diagnosed Hypertensive patient Arterial F81711 £54,220.45 £7,908.55 -£46,311.90 -£142.50 Arterial Y00758 £40,102.95 £8,015.72 -£32,087.23 -£100.92 Arterial F81222 £72,600.10 £16,500.64 -£56,099.46 -£85.68 Arterial F81151 £81,082.84 £19,384.58 -£61,698.25 -£80.97 Arterial F81104 £78,023.83 £19,783.31 -£58,240.52 -£73.22 Arterial F81045 £38,440.64 £9,810.06 -£28,630.58 -£72.30 Arterial F81648 £27,330.13 £7,165.74 -£20,164.39 -£69.29 Arterial F81158 £40,021.99 £11,418.56 -£28,603.43 -£62.91 Arterial F81150 £78,852.18 £22,694.51 -£56,157.67 -£62.60 Arterial F81651 £48,299.02 £16,857.88 -£31,441.13 -£46.72 Arterial F81013 £95,826.46 £33,462.32 -£62,364.14 -£46.62 Arterial Y00469 £92,066.44 £33,015.72 -£59,050.72 -£44.81 Arterial F81080 £82,568.07 £34,757.17 -£47,810.90 -£33.48 Arterial Total 10 -£588,660.33 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG 5. The Impact of Prescribing Combined with Improved Case Finding of Hypertensive Patients on Secondary Care Costs Figure 3.1 (page 4) identified inadequate case finding of hypertensive patients within the Arterial Locality. Failing to identify and therefore clinically manage hypertensive patients within primary care will inevitably drive increased secondary care costs. The project team wished to model the potential impact that improved case finding of hypertensive patients would have on secondary care costs at a CCG, locality and practice level. Current prescribing, although not 100% compliant with the latest NICE guidance will be having an impact on preventing secondary care costs. However, this is impossible to quantify accurately. However, by adapting the NICE costing template for Hypertension we have been able to model the potential savings that would result in current secondary care costs related to hypertension, if case finding were improved from current levels. We have therefore used as a baseline, the current savings resulting from clinical management of hypertension within primary care if current NICE prescribing guidance were adhered to, but case finding did not improve, and then applied the model to an increased ratio of observed/expected number of hypertensive patients at 70%, 80%, 90% and 100%. At no change in increased case finding we have therefore assumed a £0 saving in secondary care events. This is likely to result in an under-estimation of increased secondary care saving costs, as we know current prescribing behaviour of individual practices does not follow NICE guidelines in every case Figure 5.1 and table 3 show the results of this health economic modeling for the Arterial Locality. Table 4 breaks savings down to practice level. Significant additional savings are delivered to the locality as case finding increases. Even though prescribing savings reduce as case finding increases, saving in secondary care events increase at a much greater rate. The difference between the secondary care savings baseline figure (which we have treated as £0 at no increase in case finding) and the secondary care events savings at 100% case finding is a net overall saving of £738,687. However this figure is likely to be an under estimation of potential savings as it assumes that current savings in secondary care events equal that which would have been obtained if current prescribing practice is 100% compliant with current NICE guidelines on prescribing for hypertension, which we know not to be true. Please note also, that the secondary care events savings look only at circulatory conditions and do not consider savings that may derive from other conditions such as diabetes, so in this sense are likely to be an underestimation. Figure 5.1 Summary of Potential Cost Savings for Arterial Locality through implementation of NICE Guidance CG127- Hypertension plus improved case finding 11 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG Table 3 Summary of Potential Cost Savings for the Arterial Locality through implementation of NICE Guidance CG127- Hypertension plus improved case finding Current Prescribing Cost Arterial Locality Prescribing Change Only Prescribing Change Plus 70% Case Finding Prescribing Change Plus 80% Case Finding Prescribing Change Plus 90% Case Finding Prescribing Change Plus 100% Case Finding Prescribing Costs if NICE Guidance Followed Change In prescribing cost Secondary Care Events Cost if NICE prescribing and guidance followed (allows for increased prescribing costs) Net Overall Savings (Prescribing plus secondary care events) £829,435 £240,775 -£588,660 £0 -£588,660 £829,435 £263,516 -£565,919 -£48,196 -£614,115 £829,435 £301,162 -£528,273 -£127,365 -£655,639 £829,435 £338,807 -£490,628 -£206,534 -£697,163 £829,435 £376,452 -£452,983 -£285,704 -£738,687 Table 4 - Summary of Potential Cost Savings for the Arterial Locality through implementation of NICE Guidance CG127- Hypertension plus improved case finding by Practice Current Prescribing Costs If NICE prescribing guidelines followed and no improvements to disease register Change in spend on secondary care events Total Change avoided in spend Prescribing (Stroke and (Prescribing Costs if NICE Net Savings in Ischeamic plus events Guidance Prescribing - Heart avoided) Followed [A] Disease) [B] [A]+[B]) If NICE prescribing guidelines followed and 70% Disease register completeness Change in spend on secondary care events Total Change in avoided Spend Prescribing (Stroke and (Prescribing Cost if NICE Net Savings in Ischeamic savings plus Guidance Prescribing Heart events avoided Followed [C] Disease) [D] [C]+[D]) If NICE prescribing guidelines followed and 80% Disease register completeness Change in spend on secondary Total Change care events in Spend avoided (Prescribing Prescribing (Stroke and savings plus Cost if NICE Net Savings in Ischeamic events Guidance Prescribing Heart avoided Followed [E] Disease) [F] [E]+[F]) Locality Practice Arterial F81080 82568.07125 £34,757.17 -£47,810.90 £0.00 -£47,810.90 £43,546.56 -£39,021.51 -£18,934.14 -£57,955.65 £49,767.50 -£32,800.57 -£32,335.30 -£65,135.87 Arterial F81045 38440.64 £9,810.06 -£28,630.58 £0.00 -£28,630.58 £15,329.46 -£23,111.18 -£11,682.03 -£34,793.21 £17,519.38 -£20,921.26 -£16,317.08 -£37,238.35 Arterial F81013 95826.45732 £33,462.32 -£62,364.14 £0.00 -£62,364.14 £43,140.53 -£52,685.93 -£20,286.47 -£72,972.40 £49,303.47 -£46,522.99 -£33,204.57 -£79,727.57 Arterial F81222 72600.09815 £16,500.64 -£56,099.46 £0.00 -£56,099.46 £17,973.20 -£54,626.90 -£3,063.62 -£57,690.53 £20,540.80 -£52,059.30 -£8,405.46 -£60,464.76 Arterial F81104 78023.83176 £19,783.31 -£58,240.52 £0.00 -£58,240.52 £21,631.56 -£56,392.28 -£3,896.58 -£60,288.86 £24,721.78 -£53,302.05 -£10,411.58 -£63,713.63 Arterial F81648 27330.13 £7,165.74 -£20,164.39 £0.00 -£20,164.39 £6,412.23 -£20,917.90 £1,604.44 -£19,313.45 £7,328.27 -£20,001.86 -£346.06 -£20,347.92 Arterial F81651 48299.01824 £16,857.88 -£31,441.13 £0.00 -£31,441.13 £14,401.52 -£33,897.50 £5,141.54 -£28,755.96 £16,458.88 -£31,840.14 £835.17 -£31,004.96 Arterial F81150 78852.17795 £22,694.51 -£56,157.67 £0.00 -£56,157.67 £29,389.39 -£49,462.78 -£13,875.01 -£63,337.80 £33,587.88 -£45,264.30 -£22,576.29 -£67,840.59 Arterial F81158 40021.99355 £11,418.56 -£28,603.43 £0.00 -£28,603.43 £16,485.55 -£23,536.44 -£10,579.03 -£34,115.47 £18,840.63 -£21,181.36 -£15,496.04 -£36,677.41 Arterial Y00469 92066.44187 £33,015.72 -£59,050.72 £0.00 -£59,050.72 £20,905.95 -£71,160.49 £25,341.35 -£45,819.15 £23,892.51 -£68,173.93 £19,091.56 -£49,082.37 Arterial Y00758 40102.95478 £8,015.72 -£32,087.23 £0.00 -£32,087.23 £8,058.17 -£32,044.78 -£88.28 -£32,133.07 £9,209.34 -£30,893.61 -£2,482.34 -£33,375.96 Arterial F81711 54220.45 £7,908.55 -£46,311.90 £0.00 -£46,311.90 £8,380.63 -£45,839.82 -£1,017.20 -£46,857.02 £9,577.86 -£44,642.59 -£3,596.89 -£48,239.48 Arterial F81151 81082.83675 £19,384.58 -£61,698.25 £0.00 -£61,698.25 £17,861.69 -£63,221.15 £3,138.84 -£60,082.31 £20,413.36 -£60,669.48 -£2,120.41 -£62,789.89 TOTALS 829435.1016 £0.00 -£588,660.33 £263,516.44 -£565,918.66 -£48,196.19 12 £240,774.78 -£588,660.33 -£614,114.85 £301,161.65 -£528,273.46 -£127,365.31 -£655,638.76 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG If NICE prescribing guidelines followed and 90% Disease register completeness Change in spend on secondary Total Change care events in Spend avoided (Prescribing Prescribing (Stroke and savings plus Cost if NICE Net Savings in Ischeamic events Guidance Prescribing Heart avoided Followed [G] Disease) [H] [G]+[H]) If NICE prescribing guidelines followed and 100% Disease register completeness Change in spend on secondary Total Change care events in Spend avoided (Prescribing Prescribing (Stroke and savings plus Cost if NICE Net in savings Ischeamic events Guidance in Prescribing Heart avoided Followed [I] Disease) [J] [I]+[J]) Locality Practice Arterial F81080 £55,988.44 -£26,579.63 -£45,736.47 -£72,316.10 £62,209.37 -£20,358.70 -£59,137.64 -£79,496.33 Arterial F81045 £19,709.30 -£18,731.34 -£20,952.14 -£39,683.48 £21,899.22 -£16,541.42 -£25,587.20 -£42,128.62 Arterial F81013 £55,466.40 -£40,360.06 -£46,122.67 -£86,482.73 £61,629.33 -£34,197.13 -£59,040.78 -£93,237.90 Arterial F81222 £23,108.40 -£49,491.70 -£13,747.30 -£63,239.00 £25,676.00 -£46,924.10 -£19,089.14 -£66,013.24 Arterial F81104 £27,812.00 -£50,211.83 -£16,926.57 -£67,138.40 £30,902.22 -£47,121.61 -£23,441.57 -£70,563.18 Arterial F81648 £8,244.30 -£19,085.83 -£2,296.56 -£21,382.39 £9,160.33 -£18,169.80 -£4,247.06 -£22,416.85 Arterial F81651 £18,516.24 -£29,782.78 -£3,471.19 -£33,253.97 £20,573.60 -£27,725.42 -£7,777.56 -£35,502.97 Arterial F81150 £37,786.36 -£41,065.82 -£31,277.57 -£72,343.39 £41,984.85 -£36,867.33 -£39,978.85 -£76,846.18 Arterial F81158 £21,195.71 -£18,826.28 -£20,413.06 -£39,239.34 £23,550.79 -£16,471.20 -£25,330.07 -£41,801.28 Arterial Y00469 £26,879.07 -£65,187.37 £12,841.76 -£52,345.60 £29,865.64 -£62,200.80 £6,591.97 -£55,608.83 Arterial Y00758 £10,360.51 -£29,742.45 -£4,876.40 -£34,618.85 £11,511.68 -£28,591.28 -£7,270.46 -£35,861.74 Arterial F81711 £10,775.10 -£43,445.35 -£6,176.58 -£49,621.94 £11,972.33 -£42,248.12 -£8,756.28 -£51,004.40 Arterial F81151 £22,965.03 -£58,117.81 -£7,379.66 -£65,497.47 £25,516.70 -£55,566.14 -£12,638.91 -£68,205.05 TOTALS 13 £338,806.85 -£490,628.25 -£206,534.42 -£697,162.67 £376,452.06 -£452,983.04 -£285,703.53 -£738,686.57 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG 6. DISCUSSION, CONCLUSIONS and RECOMMENDATIONS This report highlights the potential for cost savings in the Hypertension Care Pathway within the Arterial Locality, through improved case finding and changes in prescribing behaviour within CCG practices to match the latest NICE Guidelines on Hypertension (CG127). It is based on a NICE theoretical costing model which states that 41% on hypertensive patients are likely to be on first line treatment, 41% on second line treatment and 18% on third line treatment, and assumes that the most cost effective drug is prescribed in each case. It compares the costs of these drugs to the current prescribing costs of individual practices which have been derived from prescribing data obtained SystmOne remote reporting and applying PCT current drug costs obtained from the PCT’s Medicines Management Team. Several caveats need to be borne in mind when interpreting the results of contained within the report: Firstly, the prescribing and secondary care savings are based on a NICE health economic model that itself makes assumptions in terms of the percentages of patients at each part of the pathway. This may not completely accurately reflect the situation within the locality. Secondly the report is designed to scope the potential for savings and although savings are based on a costing model that calculates return over a year, does not pretend to conclude that such savings could be realised immediately. It assumes that every GP adopts the formulary recommended first choice most cost effective drug for every patient in every case. Individual patient responses to the same drug obviously differ on a case by case basis, and it may not be clinically practical to prescribe the first choice most cost effective drug for every patient in every case. Thirdly, it must be recognised that both improving case finding of hypertensive patients and changing current prescriptions of known hypertensive patients requires additional GP practice time, and this in itself will have a cost to the system. It is therefore important to recognise that achieving even a percentage of the potential savings highlighted within this report is likely to take time and a ‘step change’ process is more practical over a longer time period. For example, individual practices may want to consider whether to concentrate on improving monitoring of known hypertensive patients before looking to increase case finding, or equally to review current prescribing against the latest guidance. However practices should not attempt to increase register sizes without first committing to follow the new NICE prescribing recommendations. Failure to do so could result in a reduction in over-all savings. It is likely to be more difficult to shift a patient from one drug than to prescribe the cost effective drug(s) initially. Bearing the above caveats in mind, the report does make the following conclusions: - Modeling against NICE guidance on prescribing and using NICE assumptions of 41%, 41%, 18% of patients on first, second and third line treatment respectively, gives a potential of up to £588,680 worth of savings in prescribing costs if all practices prescribed to the latest NICE guidance and adopted the formulary recommended first choice drugs of NICE (although this may not be suitable for every patient). 14 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG - Case finding of hypertensive patients across the Arterial locality is generally low and there is considerable potential to improve this. The pay back in terms money saved in Ischaemic Heart Disease and Stroke secondary care costs more than out-weighs the additional prescribing cost. Practices within the locality should investigate ways to ‘systemise’ the recording of blood pressure in all patient consultations with patients over 40 where BP is not known, in order to improve case finding. Participating in the Local Enhanced Service for NHS Health Checks may be another mechanism to increase case finding. Other mechanisms for improving case finding should also be explored, for example commissioning blood pressure monitoring through community pharmacy for stable hypertensives which would free up practice time to concentrate on the more difficult cases. - There is a theoretical potential saving of just under £285,704 in reduced secondary care events costs if case finding were increased to 100% in all practices and a total potential saving of just under £738,687 if prescribing cost savings are added. - There is variation between different practices within the CCG in terms of QOF indicators BP4 and BP5 (monitoring of blood pressure in known hypertensives every 9 months and reducing it to 150/90) with many practices performing at levels that place them within the highest performing quintile of England, whilst others falling well below this level. There is therefore potential to improve clinical management of hypertension within primary care across the locality. Individual practices with poorer scores in BP4 and 5 should seek to learn from locality practices in the top quintile of performance in England. - The rate of non-elective admissions for hypertension remains lower than both England and regional averages for all practices which is positive. However, because the actual number of events on this indicator is very small, confidence intervals are wide. It is likely that improving case finding and clinical management of hypertension within primary care will reduce the rate of non-elective admissions for other circulatory disease. This will be explored in the next ‘deep dive’ report undertaken for the CCG. 15 ‘Deep Dive’ Report on Hypertension for Arterial Locality of the Basildon and Brentwood CCG