Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
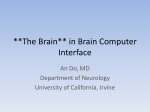
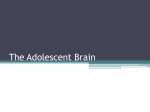
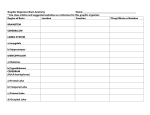
Chapter 2 Brain and Behaviour Dr. John Puxty Dr. Ken Le Clair Dr. Marie-France Rivard BPSD – Handbook for Family Physicians BPSD – Handbook for Family Physicians Chapter Index Overview .....................................................................................................1 Key Concepts .............................................................................................1 Understanding Brain and Behaviour: A Structural/Functional Approach .....................................................................................................2 The Frontal Lobe ............................................................................................ 3 The Temporal Lobe ........................................................................................ 5 The Parietal Lobe ........................................................................................... 6 The Occipital Lobe.......................................................................................... 7 The Cerebellum, Brain Stem and Sub-cortical Regions ................................. 8 The Limbic Region.......................................................................................... 9 The 7A’s of Dementia .............................................................................. 10 1. Anosognosia: No Knowledge of Illness or Disease .................................. 10 2. Amnesia: Loss of Memory ........................................................................ 11 3. Aphasia: Loss of Language ...................................................................... 12 4. Agnosia: Loss of Recognition ................................................................... 13 5. Apraxia: Loss of Purposeful Movement .................................................... 13 6. Altered Perception .................................................................................... 14 7. Apathy: Loss of Initiation .......................................................................... 15 Summary .................................................................................................. 16 Table: Summary of Brain Function and Behavior ......................................... 16 BPSD – Handbook for Family Physicians BPSD – Handbook for Family Physicians 1 of 16 Pages Overview This chapter explains the impairments and behaviours that are commonly seen in dementia through a structural/functional approach; that is, by an exploration of the regions of the brain and their functions. In addition, it introduces the “7 A’s of Dementia”, which is a handy tool for describing the losses in dementia and the associated behaviours. A summary chart of the brain regions, their functions and characteristic dysfunctions, appears at the end of the chapter. Key Concepts As a consequence of the impairments and losses caused by damage to the brain in dementia, the individual experiences a different “reality” than others around him or her. In addition, these deficits can precipitate a variety of negative emotional states such as frustration, fear, confusion or anger. Subsequently, the individual may express a variety of behaviours that are known as the “Behavioural and Psychological Symptoms of Dementia” (BPSD). Informal and formal caregivers are often challenged by these behaviours and may misinterpret them as being volitional or intentional. They may consequently respond in ways that are damaging to the individual with dementia. 1. The physician can play a key role in helping caregivers to understand that these “challenging” behaviours are not wilful or intentional, but rather occur as a result of an “illness” or “malfunction” of the brain, and represent an individual’s adaptive response to a negative stimulus in their physical or social environment. 2. Depending on the type and progression of dementia, different behaviours and impairments are expressed to a greater or lesser degree. For example, individuals with fronto-temporal dementia present with significant behavioural problems, perseverative behaviours and language difficulties early in the course of the disease. An awareness of the prominence and timing of the expression of certain behaviours assists the physician to: • detect the presence of dementia • determine the type of dementia • guide conversations about care planning with the individual, family, and collaborative care team. 3. A useful way to guide the understanding of common behaviour changes in dementia is to consider the functions of the three levels of the “Developmental Brain”: • cortex and/or forebrain (The Thinking Brain) • midbrain (Emotional Brain) • the lower brain or brain stem (Instinctual Brain) In Alzheimer’s disease, as the cortex or forebrain (Thinking Brain) becomes impaired, behaviours associated with the midbrain (Emotional Brain) and lower brain (Instinctual Brain) become more evident. Stressful situations are therefore more likely to evoke emotional responses such as irritability, emotional lability and sexual disinhibition or instinctual responses such as rummaging/hoarding, fight or flight, and territoriality. Appreciating these realities helps us to more meaningfully interpret the behaviours of a person with dementia as responsive rather than wilful, purposeful or perhaps even vengeful. This approach can also provide insights into predicting behaviours and exploring appropriate care strategies to prevent, or should they occur, to support the negative consequences of these behaviours for the person, his or her family and others. BPSD – Handbook for Family Physicians 2 of 16 Pages Understanding Brain and Behaviour: A Structural/Functional Approach © Copyright CSAH 2009 Figure 1: The lobes of the brain. BPSD – Handbook for Family Physicians 3 of 16 Pages The Frontal Lobe © Copyright CSAH 2009 The frontal lobe controls “executive functions” like planning and organization, initiation or changing activity, and insight. It also regulates emotional responses, personality and socially appropriate behaviour, and is responsible for “expressive language”. Frontal Lobe Dysfunction Planning and organization Difficulties in planning and organization lead to an inability to plan and complete basic tasks such as activities of daily living, or more complex tasks, such as planning a holiday or a dinner party. Way-finding may be challenging for the individual, even with familiar routes. Initiation An inability to initiate activity may be misconstrued by caregivers as laziness, uncooperativeness, or even depression. The person with dementia may appear uninterested in doing anything, even previously enjoyed activities and hobbies. This lack of initiation (apathy) can be a tremendous source of caregiver strain. Spouses or other family members may believe that the person is unwilling to contribute to household chores (as they no longer take the initiative to offer help) or pursue activities on his or her own (which would free the care provider to attend to his or her own activities). Perseveration In contrast to the inability to initiate an activity, perseveration may occur, which is the inability to stop an activity. Perseveration affects not only behaviour (rubbing hands together or tapping a table), but also language (perseverating on the same story or word) and emotions (a frustrating experience early in the day can lead to frustrated mood all day). Perseverative behaviours are often frustrating for caregivers. BPSD – Handbook for Family Physicians 4 of 16 Pages Caregivers can be encouraged to initiate activities that incorporate perseveration into a more appropriate or meaningful activity, such as folding laundry, flipping through a catalogue, magazine or photo album, or sanding a small toy. Similarly, triggering positive emotions at the beginning of the day through a pleasant demeanour (smiling caregiver), and engagement in positive and meaningful conversation (reminding the person of previous accomplishments, funny anecdotes, and important loved ones), will significantly increase the likelihood that this positive mood will persist throughout the day. Insight The frontal lobes provide feedback and insight about how a person is performing. Incorrect feedback may create a false belief that there is nothing wrong, and cause the individual to refuse assistance, where assistance is actually required. Often, refusal of assistance may be delivered in the form of a verbal outburst. Caregivers, understandably, are often hurt by these angry exchanges, and struggle to contain these emotions while providing care. Furthermore, apologies are usually not forthcoming since the person is unable to appreciate the impact of their actions on others. When the spouse is the main caregiver, he or she may have lost his or her long “confidante” and may not be able to vent such feelings to anyone for some time. This issue needs to be addressed with care providers. Suggestions to improve care providers’ wellness may include stepping back and taking a “time out” to deal with their emotions before pursuing care, finding an empathetic ear to vent those feelings on a regular basis, or using humour or relaxation techniques to diffuse these emotions. This lack of insight may cause an individual to be rather impulsive in thought, affect, and action. Regulation of emotions, personality, and socially appropriate behaviour Frontal lobe impairment can lead to socially challenging events, such as verbal outbursts or inappropriate sexual behaviours. These behaviours tend to occur in response to a stimulus where the individual is unable to hold back initial responses. For example, in a person with a “normal” frontal lobe, a stimulus that causes acute intense pain (e.g. stubbing one’s toe) may lead to an over-ride of the frontal lobe and cause use of uncharacteristic language or display of anger. In an individual with an impaired frontal lobe, a stimulus of much lower intensity such as discomfort or hunger may cause the same or more extreme behaviour. Emotional lability and mood changes with swings in emotions to quite mild stimuli are often present in frontal lobe dysfunction. Language expression With impairment in the frontal lobes, the individual loses vocabulary and has difficulty with expressing language and articulating speech, finding the right word, and word order (expressive aphasia). There is a poverty of language and it is non-fluent in flow. BPSD – Handbook for Family Physicians 5 of 16 Pages The Temporal Lobe © Copyright CSAH 2009 The temporal lobe controls language comprehension, and memory. Impairments in this region cause difficulties with expression and comprehension, an inability to learn new things, and a loss of long-term memory from most to least recent. Temporal Lobe Dysfunction Language comprehension Hearing is affected in temporal lobe damages, as is the ability to comprehend language and remember words (receptive aphasia). The individual has difficulty organizing verbal information and selectively attending to auditory and visual input. The person may forget what has been said and may repeat things or ask the same question over and over. Often the flow of language is fluent but it lacks meaningful content (gibberish). Persistent talking may be a behaviour associated with temporal lobe dysfunction. Memory Short-term memory impairments lead to an inability to learn new things, and, as a result, difficulty adjusting to new situations. For example, if the person moves to a new home or a long-term care home, he or she may have trouble orienting to new surroundings, and may encounter difficulties finding the correct bedroom or the bathroom. With progressive dementia loss of long-term memory may result in a person becoming disoriented in a setting that may have been familiar for a number of years. The individual may look for the familiarity of previous environments such as the home he or she grew up in, thereby asking to “go home” (to his or her parents) while in his or her own home. The loss of long-term memory and temporal lobe damage is also associated with the loss of ability to do familiar things (apraxia) such as use tools, the stove etc., which may present significant safety issues. Visual memory is affected as well, as the person may no longer recognize familiar faces (agnosia). More information on aphasia, amnesia, apraxia, and agnosia is found in the “7 A’s of Dementia” section further in this chapter. BPSD – Handbook for Family Physicians 6 of 16 Pages The Parietal Lobe © Copyright CSAH 2009 The parietal lobe is the analysis and perception center of the brain, integrating sensory information in order to formulate the meaning and relationships of language, numbers, people, objects, and places. Parietal Lobe Dysfunction Analysis and perception With damage to the parietal lobes, the individual has difficulty integrating sensory information in order to perform reading, writing, drawing, constructing, or calculating. In addition, the ability to recognize familiar places, objects and people is impaired (agnosia) because the person has difficulty integrating and interpreting the sensory information. The individual may be unable to appreciate the extent or existence of their deficits (anosognosia). Organization and sequencing of language and activities Parietal lobe damage results in an inability to perform activities in sequence. While the person may be able to complete individual steps, he or she may be unable to put all of the steps together to complete an activity (apraxia). Care providers may have to give ”step-by-step” directions to allow the person to complete tasks without direct assistance. Calculation and manipulation of numbers The parietal lobe is responsible for the ability to use numbers. When impaired, activities such as using the telephone, paying bills, or calculating financial transactions become difficult. Visuo-spatial perception and planning Spatial perception, the ability to know how close or how far one is from an object, becomes impaired. An abnormal “clock drawing test”, which is evidence of visuo-spatial planning difficulties, is often used to identify the deficit which has a number of functional consequence including affecting ability to drive safely. BPSD – Handbook for Family Physicians 7 of 16 Pages The Occipital Lobe © Copyright CSAH 2009 The occipital lobe controls vision and depth perception. A loss of peripheral vision, and an inability to focus or track movement results from damage to this area of the brain. Occipital Lobe Dysfunction Vision Peripheral vision may be lost leading to tunnel vision, only seeing things, objects or people that are directly in front the individual (visual field cuts). Persons approaching from the side are not seen until they may appear to have “jumped in front of the patient”, causing startling responses. The person may have difficulty focusing on or tracking a moving object. He or she may no longer be able to follow a television show or movie, “losing interest” as a result. Difficulties with reading, writing, and recognition of objects, words, colours result from damage to the occipital lobe. Depth perception The risk for falls increases due to the inability to judge distance on stairs. The individual may be fearful stepping into bathtub, as the water may appear very deep. Also, dark tiles in carpet or flooring may appear as holes. The individual may have frequent “spills” when pouring into cups or containers. BPSD – Handbook for Family Physicians 8 of 16 Pages The Cerebellum, Brain Stem and Sub-cortical Regions © Copyright CSAH 2009 In the previous discussion we have focused on functions of the cortex or outermost layers of the cerebrum that play a key role in memory, attention, perceptual awareness, thought, language, and consciousness. Beneath the cerebral cortex is the sub-cortex which links the cortex to structures such as the thalamus and the basal ganglia. The term sub-cortical dementia relates to specific clinical manifestations and neuroanatomical findings arising from lesions predominantly in the basal ganglia, brain stem nuclei and cerebellum. Cerebellum, Brain Stem, and Sub-cortical Dysfunction Voluntary movement, balance and coordination The cerebellum and brain stem control voluntary movement and balance functions; the brain stem controls all involuntary body systems, which include the heart, lungs, and digestive system. The cerebellum and brain stem are often not impaired until the late stages of the dementia. As coordination and balance functions are lost, the person often loses the ability to walk safely. The person becomes bedridden and, with increasing immobility, the body becomes more prone to pneumonia and pressure ulcers. Swallowing Swallowing difficulties may occur causing choking spells and increasing the risk for aspiration pneumonia, which can lead to death. Regulation of involuntary thought processes Sub-cortical deficits are a feature of vascular dementia, Parkinson’s Disease and Huntington’s Disease. They include slowing of thought processes (bradyphrenia), difficulty in memory retrieval, and problems with changing cognitive strategies (mindset). Sub-cortical dementia is also more likely to affect attention, motivation and emotionality. People with sub-cortical dementia often show early symptoms of depression, clumsiness, irritability or apathy. BPSD – Handbook for Family Physicians 9 of 16 Pages The Limbic Region © Copyright CSAH 2009 The limbic system connects the frontal and temporal lobes, linking behaviour with memories. It is responsible for storing new memories, for emotional control, and control of autoregulatory functions such as sleep-wake cycles, temperature, appetite and thirst. It is often affected early in Alzheimer’s Disease, particularly the hippocampus, which is responsible for storing new memories. Limbic Dysfunction Connection of behaviour with memory The limbic system connects the frontal and temporal lobes, linking behaviour with memories. When a person looks for a misplaced object, the first reaction (unfiltered by the frontal lobe) is to assume someone else has moved or taken it, before also considering the possibility that they may have misplaced it themselves or may have a faulty memory. Persons with dementia often have an impaired filtering and analysis of events and are likely to accuse others of stealing the object. As a result, poor memory leads to misinterpretations of events, anger, suspiciousness, and blaming others. Emotional control Damage in the limbic system can result in emotions that are extreme and change rapidly, including irritability, depression and anxiety. Blunting of emotions may also occur and the person may appear uninterested or unaffected emotionally by events in his or her immediate environment. Auto-regulatory functions – sleep, appetite, thirst, body temperature The limbic system also controls daily functions such as sleeping and appetite; so the person may lose track of when he or she would normally be awake or sleeping. This may result in the individual being awake through the night (day-night reversal). The hypothalamus, which is responsible for control of body temperature, thirst, and appetite, is also part of the limbic system. A person with damage in the hypothalamus may feel cold deep in the bones or feel extremely hot. The person may also experience extreme thirst or appetite. BPSD – Handbook for Family Physicians 10 of 16 Pages The 7A’s of Dementia The 7 A’s tool is a useful way to categorize and understand the most common losses of dementia. The 7 A’s are: 1. Anosognosia (no knowledge of illness or disease) 2. Amnesia (loss of memory) 3. Aphasia (loss of language) 4. Agnosia (loss of recognition) 5. Apraxia (loss of purposeful movement) 6. Altered Perception (loss of visual perception) 7. Apathy (loss of initiation) The 7 A’s is an effective tool to understand the way the person with dementia is experiencing the world. This insight helps us shape the way we interact with the individual and with the creation of individualized and supportive care strategies. It has been applied in P.I.E.C.E.S. training programs throughout Ontario over the last several years, and enables us to use a common language for dialogue and collaborative care planning. 1. Anosognosia: No Knowledge of Illness or Disease a = no; nosos = illness/disease; gnosia = knowledge of A person affected by dementia (with formerly intact functional abilities), living in the present but only accessing their past, may lack insight into their own deficits have and have difficulty appreciating his or her needs for assistance and may become angry with care providers. This is particularly likely to occur if parietal lobe pathology is present. Behaviours which may be associated with Anosognosia: • Overestimation of abilities, poor judgment, problem-solving, planning, leading to safety issues (e.g. attempting to self-transfer when not physically able, driving, doing finances). • Resistance to care which may include physical aggression (e.g. pushing away, slapping, kicking). • Uncharacteristic or inappropriate verbalizations or profanities (inability to control impulses). • Being unaware that they are in a hospital or long-term care home (they may think they are at home, at work, at school etc.). • Unaware of consequences of behaviour on others, i.e. “how it makes other people feel”. • Perseveration of thought, task, emotion, or phrase; like an “on-off” switch stuck in the “on” position. • Impaired attention and concentration. BPSD – Handbook for Family Physicians 11 of 16 Pages Effective care strategies for Anosognosia: • Understand that behaviours are not wilful or intentional. • When re-approaching the individual, smile, use positive words and a friendly and relaxed tone. This approach is crucial to the success of a second attempt if a caregiver needs to proceed with a task or activity. • Use a non-confrontational approach to resistive or aggressive behaviours. • Avoid punitive approaches that attempt to instil remorse, or belabour how the person’s behaviour makes other people feel. • Realize that negative interactions may provoke an angry or frustrated mood that persists all day. • If required, caregivers should “step back” and regain their composure prior to responding to the resistive or aggressive behaviour. 2. Amnesia: Loss of Memory The vast majority of information processing occurs outside of our conscious awareness. Only novel information is processed at a conscious level. For the person with dementia and memory loss, more and more information appears new and unfamiliar requiring increasing energy to process. This can lead to feeling overwhelmed or frustrated. Short-term memory is the most important aspect of memory, allowing information to be held long enough to get into long-term storage. Without access to short-term memory, the person with dementia can no longer consciously learn. Long-term memory is divided into two areas: declarative, for all information learned or experienced over time, and procedural for all tasks learned. Both are stored in layers. As a person proceeds through life, memories pile on top of each other, so that the first thing a person experienced or learned is at the bottom and the last thing learned is at the top of this pile. Memory is lost in reverse order, i.e. the last thing learned is the first thing lost (think of it like knitting a sweater, then beginning to unravel it row by row). A person with memory loss may not remember what happened this morning or last week, but still has intact memory for information that happened a long time ago. In effect, a person with cognitive impairment lives in the present, but only has access to information in the past. Their access to information (i.e. their reality) may be 30-40 years back, and they will therefore act based on that information. “The person’s reality is not our reality.” The phenomena of reversed memory lose applies also to recognition of caregivers and family member. If the individual has remarried later in life the spouse who is the main caregiver may be perceived as a stranger or imposter. BPSD – Handbook for Family Physicians 12 of 16 Pages Behaviours that may be associated with Amnesia: • Becoming anxious and overwhelmed by too much new information. • Accusing family and caregivers of being imposters. • Accusing others of withholding information, stealing items, not visiting, etc. • Becomes suddenly uncooperative with familiar tasks or activities. • Refusing assistance with care. • Repeating questions, comments or behaviours. • “Time Warp Delusions”, e.g. a past memory is triggered by a stimulus in the present, which can cause extreme emotional reactions or misinterpretation of events. Effective care strategies for Amnesia: Use memory aides or reminders such as: Keeping a diary or other visible written schedules for “bath days”. Using a “signing book” for visitors. Displaying pictures of loved ones, family and friends. Repeat information without pointing out that the information has been provided before and forgotten. • Validate experiences of the past while redirecting the individual to more pleasant and meaningful activities in the present. • Create a “memory trail” to enable new learning by doing important tasks the same way, every day. Routines are important. • Rather than confronting them it may be helpful to offer to look for the missing items. • • • • 3. Aphasia: Loss of Language The regions of the brain that control the expression and comprehension of speech are located in different areas of the brain. With receptive aphasia, which is usually associated with temporal lobe pathology, the person may be able to express him or herself but cannot understand what is being said. With expressive aphasia, which is usually associated with frontal lobe pathology, the individual may be able to comprehend speech, but is unable to express him or herself. Communication difficulties and misunderstandings between the person, the family, and the health care team are common and often attributable to some degree of aphasia. Care providers may assume that the person’s communication skills are intact because the failure to follow directions may be episodic or situational. It may be that some care providers use more nonverbal cues within their communications, and the individual performance may vary within a 24 hour time period. Despite impairment in the person’s expressive and receptive language functions, he or she often remains responsive to appropriate non-verbal communications of others (e.g. smiling, gestures and directly facing). Behaviours associated with Aphasia: • Difficulty following conversations, especially more than one (receptive aphasia). • Social withdrawal. • Word substitution, using the wrong word, leading to inappropriate statements or requests. • Reversion to first language (even if not used for number of years). BPSD – Handbook for Family Physicians 13 of 16 Pages Effective care strategies for Aphasia: • Suspect the presence of expressive and receptive aphasia. • Maintain a high index of suspicion for pain, discomfort, or other symptoms that the individual may not be able to express. • Use positive, supportive non-verbal communication that conveys calmness, reassurance and kindness, e.g. facial expressions, body postures, tone of voice, etc. 4. Agnosia: Loss of Recognition The individual with dementia and impaired parietal lobe sensory integration function can experience a loss of their ability to both recognize and respond appropriately to people (including self), objects and sounds. Confusion, suspicion, and inappropriate behaviour (e.g. sexual expression) can result from the individual’s progressively anachronistic self-perception and from the misidentification of others. Safety and care issues are likely to arise from the inappropriate use of objects, as a result of a loss of recognition of objects and their intended purpose. Behaviours associated with Agnosia: • Loss of recognition of people in the reverse order that they came into the person’s life (i.e. grandchildren are forgotten first). • Thinking of themselves as much younger than in actuality; becoming confused at having “older” spouse, adult children the same age as the individual, etc. • Delusions that a family member or care provider is an imposter. • “Inappropriate” sexual behaviour resulting from deluded self-perception and misidentification of others. • Disturbed by mirrors, especially when reflecting the person (and other caregivers) in their most personal space (e.g. bedroom/bathroom). May not recognize self or other caregivers, so the perception is of a stranger(s) watching him or her undress, bathe, toilet, etc. • Inappropriate use of objects, or forgetting what they are for (e.g. toothbrushes, faucets, and toilet). • Defensive reactions to care using “unfamiliar” objects (e.g. caregiver trying to brush teeth causes resistance). • Impaired auditory recognition (e.g. a cat meowing may be thought to be a crying baby). Effective care strategies for Agnosia: • Remove or reverse mirrors. • Mimic the use of an object (such as toothbrush or face cloth) prior to handing it to the person or administering care. • Provide reassurance that the person in the environment is a family member or a care provider who is there appropriately. 5. Apraxia: Loss of Purposeful Movement A person with cognitive impairment loses the ability to plan, sequence and execute the steps of particular tasks. Every task has a sequence and order. Even the simplest of tasks, such as brushing teeth or combing hair, consists of a number of steps. The individual with dementia loses the ability to discern what step comes where in the sequence. The person also has an impaired ability to attend to tasks, thus tending to shift from one task to another especially when distracted. BPSD – Handbook for Family Physicians 14 of 16 Pages Behaviours associated with Apraxia: • Dress apraxia, i.e. cannot sequence the layering of clothing or can’t coordinate movements to put on article of clothing. • Difficulty with push-button items, remote controls, microwaves, touch-tone phones (last learned is first lost). • Frustration and inappropriate behaviours if tasks are too difficult, unfamiliar, or have multiple steps and demands that may exceed the individual’s capabilities. • Apparent “refusal” to participate in care by saying ”no” to a suggested task or activity, despite the fact that they may appear physically able. It may not mean he or she does not want to do it, but rather that the person does not remember how. Effective care strategies with Apraxia: • Explain to care providers the impact that apraxia may have on the observed behaviours. • Set out clothes in the correct order, from top to bottom, to facilitate independent dressing. • Provide step-by-step instructions while allowing the person to proceed independently with each step, thereby preserving privacy and dignity. • Minimize distractions which compete for attention. • Whenever feasible, provide visual cuing by dressing at the same time as the person with dementia (e.g. a spousal care provider setting out clothes in the morning or a staff member demonstratively putting on a coat to go outside). 6. Altered Perception Depth perception may be altered during the course of dementia. Since loss of depth perception impacts greatly on the ability to mobilize freely through the environment, it changes the way the person walks and sits. As well, visual distortions are common and may cause misperceptions of objects, causing fearful behaviours. Behaviours associated with Altered Perception: • Verbal or physical resistance to bathing (water is perceived to be much deeper than it actually is; the individual may believe they are at risk of drowning). • Jumping over dark thresholds (looks like a crevasse) or dark tiles in floor (looks like a hole). • Avoids dark flooring (appears as body of water or ditch). • Avoids flooring with bold patterns (appears as obstacles). • The person may misinterpret clothing on a chair, pole lamps or other objects as people. • Misperceptions that people on TV are in the room, causing the person to talk to the TV or perhaps become very distressed by it. • When sitting, the person may cautiously put a hand on the edge of the seat, brush the edge of the seat with a lower leg, and then sit on the edge or even arm of the chair. Although the person may be encouraged to move to the middle, he or she may not be sure where the middle is or how far down, or how far over to go. • When walking, the person takes a more stooped pose, feet slightly apart, shoulders hunched, and knees bent a bit. The person ignores the peripheral visual fields because there is only so much information the brain can handle. The person focuses only on what is directly in front, therefore looking either straight ahead or down (mostly down). This may be a very adaptive way of mobilizing. BPSD – Handbook for Family Physicians 15 of 16 Pages • The person may be unable to relate to space and therefore bump him or herself or his or her wheelchair into objects and/or people. Effective care strategies for Altered Perception: • Identify an individual’s perceptual difficulties and understand how they may cause the behaviours. • Seek to minimize misperception by appropriate lighting, and use of colors. • Problem-solve around how to maintain safety for the person and others. 7. Apathy: Loss of Initiation Apathy occurs with damage to the medial frontal lobes. Over time, a person with cognitive impairment does not initiate conversation or activity. This is often interpreted as a symptom of depression. With dementia, the difference is that the person has lost the ability to initiate, but will participate if someone engages him or her. Conversely, someone who is depressed will not participate even if someone tries to engage him or her. The individual feels too low to motivate him or herself to interact socially, and will often complain of tiredness to cut activities short. Behaviours associated with Apathy: • A person may sit in front of a meal and not touch it until a care provider initiates the activity. • A person spends most of the day in silence with his or her chin on her chest, however, if approached and called by name, will lift his or her head to make eye contact and smile. Further information on depression in dementia is provided in Chapter 6 of this handbook. Effective care strategies for Apathy: • Initiate an activity (e.g. eating) by using verbal cues or hand-over-hand technique. This may be sufficient to enable the person to complete the task or activity independently. BPSD – Handbook for Family Physicians 16 of 16 Pages Summary Physicians have an important role in helping care providers understand how changes in the brain affects behaviour in dementia. They can help to guide caregiver interactions with the individual, and identify supportive care strategies that enable the individual’s functional abilities/potential rather than confront their cognitive losses. In this way, challenges related to the behavioural changes that occur in cognitive impairment will be minimized for the individual and others. Table: Summary of Brain Function and Behaviour Brain area Frontal lobes Î Temporal lobes Î Parietal lobes Î Occipital lobes Î Cerebellum Brain stem Sub-cortical areas Î Limbic Hippocampus Î Function Deficiency Behaviour • Executive function • Problems with planning, initiating, executing in a planned, organized manner • Re-emergence primitive reflexes • Unable to initiate (may appear lazy, uncooperative with requests) • Impulsivity • Can’t plan holiday, activities of the day, dinner party, etc. • Grabbing (Grasp reflex) and Paratonia • Language • Memory • Aphasia • Amnesia • Frustration with aphasia, annoying repetitions, unsafe use of tools, stove, disorientation. • Language analysis Calculations Spatial perception, Sequencing • Difficulty understanding • Visual-spatial planning difficulties • Difficulty sequencing movements • Apraxia • Agnosia • Anosognosia • Vague historian • Unable to manage finances or driving • Dressing, gait or eating difficulties may be present • Failure recognize people/objects • Lacks insight into disease • Vision • Depth perception • May not scan or interpret environment properly • Startled response • Afraid of tub water (appears too deep) • Messy when pouring liquids, etc. • Balance • Voluntary & • Involuntary movements • Abnormal gait/balance Slowness of movement • Swallowing problem • Falls • Slow movements • Aspiration pneumonia • Memory retrieval • Connects behaviour with memories • Regulates sleep, appetite • Misinterprets events • Emotional lability • • • • BPSD – Handbook for Family Physicians Blaming others Irritability and depression Day-night reversal Hot/cold perception changes