Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
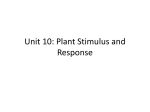
Investigative Ophthalmology & Visual Science, Vol. 31, No. 3, March 1990 Copyright © Association for Research in Vision and Ophthalmology Simultaneous Pattern Reversal ERG and VER Recordings Effect of Stimulus Field and Central Scotoma Hiroshi Sakaue, Osamu Karsumi,* Mehul Mehra, and Torsuo Hirose*t The effects of the sizes of the stimulus field and of an artificially created central scotoma on simultaneously recorded pattern-reversal electroretinogram (P-ERG) and pattern-reversal visual-evoked response (P-VER) were investigated. With an increase in the stimulus field from 4° X 4° to 12° X 12°, the amplitude of the P-ERG increased steadily. The amplitude of the P-VER also showed an increase up to a stimulus field of 6° X 6° or 8° X 8°, but showed no increase with further expansion of the stimulus field. A central scotoma, created by placing a square of black paper at the center of the 12° X 12° stimulus field, was increased from 4° X 4 ° t o l O ° X 10° by 2-degree increments. Amplitudes of both the P-ERG and the P-VER decreased with increasing central scotoma size. The P-VER decreased significantly with a 4° X 4° central scotoma. Although both the P-ERG and the P-VER were influenced by the overall stimulus field and the central scotoma, there was a distinct difference in their behavior. The P-VER showed saturation above a certain stimulus field size and, with a central scotoma of 4° X 4°, much more reduction than the P-ERG, suggesting that the P-VER depends more on the macular area than does the P-ERG. The P-ERG also exhibited a substantial macular dependency, which, however, was not as great as that of the P-VER. The greater macular dependency of the P-VER compared to the P-ERG, as observed in our study, reflects the larger anatomic representation of the macula at the higher visual level. Invest Ophthalmol Vis Sci 31:506-511,1990 The pattern-reversal electroretinogram (P-ERG), originally introduced by Riggs et al,1 was made popular by the work of Maffei and Fiorentini,2 who concluded that the P-ERG originates in the retinal ganglion cells. The origin of the P-ERG is controversial, however; Dodt3 postulated that the P-ERG may be generated in proximal retinal layers and consists of both a local luminance component at high stimulus contrasts and a pattern component at low stimulus contrasts. The nature of the P-ERG remains obscure. P-ERG is not applied in routine clinical settings, although its use in the early detection of glaucoma4"6 and in optic nerve disease7"9 has been studied. Since the original work of Spekreijse,10 numerous studies have been performed on the effects of various stimulus parameters on the recordability of the pattern-reversal visual-evoked response (P-VER). The P-VER is used widely now in ophthalmology clinics, especially to evaluate the visual pathway and macular function."12 The P-VER is influenced significantly by various stimulus parameters, including the overall stimulus field and the presence of a central scotoma.1314 Relatively few investigations have studied the effect of stimulus field and central scotoma on the P-ERG,15 and even fewer have studied the differences between the modes of response in simultaneously recorded P-ERGs and P-VERs.16"18 We believed that before the P-ERG, which is more difficult to record, is applied clinically, the different responses of the P-ERG and the P-VER to these parameter changes should be studied more precisely. Therefore, we compared the responses of the P-ERG and the P-VER to changes in the stimulus field size and the central scotoma size, using different methods from previous work.16"18 From the Eye Research Institute of Retina Foundation and *Retina Associates, and the fDepartment of Ophthalmology, Harvard Medical School, Boston, Massachusetts. Submitted for publication: November 21, 1988; accepted June 12, 1989. Reprint requests: Osamu Katsumi, MD, Eye Research Institute of Retina Foundation, 20 Staniford Street, Boston, Massachusetts 02114. Materials and Methods Four normal adults (three men and one woman ranging in age from 24 to 33 yr) participated. They had no ophthalmologic abnormalities except for a slight refractive error that was corrected optically at the time of the recordings. Prior to the examination, 506 Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017 No. 0 SIMULTANEOUS PATTERN REVERSAL ERG AND VER RECORDINGS / 5ohoue er ol the procedure was explained fully to all subjects, and their informed consent was obtained. P-ERG and P-VER were recorded simultaneously with two-channel recordings. The left eye always was tested with a natural pupil. For the P-ERG, a soft piano contact lens electrode (Model Breath-O; Toray, Tokyo, Japan) developed by Yanashima and Okisaka19 was placed in the subject's left eye after instillation of 1% proparacaine hydrochloride. The image of the checkerboard pattern viewed through this contact lens was sharp. The reference electrode for the P-ERG was placed on the center of the left lower lid, and the earlobes served as grounds. For the P-VER, Ag-AgCl disc type electrodes (Grass Instrument, Quincy, MA) were used. The active electrode was placed at Oz (10% of the inion-nasion distance from the inion on the midline), and the reference electrode was placed at Pz (30% of the inion-nasion distance from the inion on the midline). The ground electrodes were the same as those of the P-ERG. A 9-inch television monitor (model 2640 C9; Conrac, Covina, CA) was used for stimulus display. The overall stimulus field size was 12 cm X 12 cm with a cardboard border to eliminate contamination from distorted peripheral checks. The stimulus field size subtended a visual angle of 12° x 12° from a viewing distance of 57 cm. The mean luminosity level was 50 cd/m2 (1.2 log fL), and the contrast was maintained at 90%. The stimulus pattern was a square-wave checkerboard with a check size of 60 min of arc. The checkerboard pattern alternating speed was 2 Hz (4 reversals per sec), and analysis time was 200 ms. Responses were fed into the averaging computer (Cadwell model Quantum 84; Cadwell Laboratories, Kennewick, WA) after amplification through highcut and low-cut filter settings of 70 Hz and 1 Hz, respectively. The 256 responses were averaged and printed out with a plotter. Figure 1 illustrates the various stimulus modes used in this investigation. To study the effect of the overall stimulus field size, we increased the field from 4 ° X 4 ° t o l 2 ° X 1 2 o b y 2-degree increments, using frames of thick black paper. A small black fixation target was placed at the center of each stimulus field. Then a central scotoma was created by placing thick black paper of various sizes at the center of a 12° X 12° stimulus field. The size was increased from 4° X 4° to 10° X 10° by 2-degree increments. To ensure stable fixation, a small white target was placed at the center of each piece of black paper. The P-ERG and the P-VER were recorded simultaneously in a dark room. The resulting percentage amplitudes for both field and scotoma area were analyzed with three-factor Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017 50? mixed effects analyses of variance (4 subjects X 4 areas X 2 patterns; random subjects) at a preestablished 0.05 significance level. Results Both the P-ERG and the P-VER with a stimulus field of 12° X 12° showed major deflection (Fig. 2). In the P-ERG, an initial negative deflection (Nl) appeared at about 30 ms, and a positive deflection (PI) followed at about 50 ms. The amplitude was measured from Nl to PI. In the P-VER, an initial negative deflection (N70) appeared at about 70 ms, and a positive deflection (PI00) appeared at about 100 ms. The response size was calculated and served as the P-VER amplitude (N70 - PI00). Effect of Stimulus Field Size Figure 3 shows the P-ERG and the P-VER amplitudes with five different stimulus field sizes tested in four subjects. In all subjects, the amplitude of P-ERG continuously increased, up to the largest stimulus field size. The amplitude of P-VER also increased, but only up to a certain stimulus field size; saturation Stimulus Field-Size Central Scotoma Size 12x 12 ( D t g r w Squared) 4x4 (Degrees Squired) 10x10 6x6 8x8 8x8 6x6 10x10 4x4 Fig. 1. Schema of* the various modes of stimulation. 508 INVESTIGATIVE OPHTHALMOLOGY 6 VISUAL SCIENCE / March 1990 P-ERG 1.25 uV Vol. 31 toma; the reduction of P-VER amplitude was much larger than that of the P-ERG amplitude in the four subjects. The relationship between the area of the central scotoma and the P-ERG and the P-VER amplitudes is shown in Figure 6. This difference showed a trend toward statistical significance (F = 4.11, P < 0.053). P-VER 20 msec N70 J |2.5nV 20 msec Fig. 2. Tracings of simultaneous recordings of the P-ERG and the P-VER with a 12° X 12° stimulus field. 1.5" C P-VER 1 "4 -o 1.0- Ainpli was observed at a field size of 6° X 6° in one subject and at 8° X 8° in the remaining three. Figure 4 shows the relationship between the P-ERG and the P-VER amplitudes relative to the area of the stimulus field in four subjects. The amplitude of the P-ERG, expressed as percent of electroretinogram (ERG) at the largest field size, steadily increased; in the P-VER, in contrast, saturation clearly was observed beyond a stimulus field size of 8° X 8°. In the P-ERG, the percent amplitude showed a marked increase with the expansion of stimulus field size. The mean percent amplitudes of both the P-ERG and the P-VER were larger than the actual percentage area of the stimulus field at all stimulus field sizes. For example, with an 11% stimulus field area (equivalent to a 4° X 4° stimulus field), the P-VER showed 63% amplitude, whereas the P-ERG showed 29%. The percent amplitudes of the P-VER were significantly higher than those of the P-ERG at all of the stimulus field sizes tested (F = 86.49, P< 0.001). 3 g. O 0.5- P-ERG OS W a. o.o- Effect of Central Scotoma Size Figure 5 shows the P-ERG and the P-VER amplitudes with four different central scotoma sizes in four subjects. The amplitudes of both the P-ERG and the P-VER decreased in all subjects as central scotoma size increased. In the P-ERG, the amplitude decreased markedly when the scotoma was larger than 6° X 6°; in the P-VER, the amplitude significantly decreased with the 4° X 4° central scotoma, but dropped less precipitously with larger central scotomas. The most striking difference between the P-ERG and the P-VER occurred with a 4° X 4° sco- Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017 2 4 6 8 10 12 Stimulus Field Size (Degrees Squared) Fig. 3. (A) The effect of the stimulusfieldsize tested in subject 1. The abscissa shows the stimulus field size in degrees squared, and the ordinates indicate the amplitudes of the P-ERG (left) and the P-VER (right). (B, C, D) The effect of the stimulusfieldsize tested in subjects 2, 3, and 4, respectively. SIMULTANEOUS PATTERN REVERSAL ERG AND VER RECORDINGS / Sokoue er ol No. 3 509 minimal interference from scattered light. At small field sizes, our squared stimulus field could stimulate only the macular area. Thus, our results indicate slight macular dependency only with a small stimulus field area; with a large stimulus field area, the relationship between the P-ERG amplitude and stimulus field area became more linear, suggesting equal effec- 0 10 20 30 40 50 60 70 80 90 100 % Stimulus Field Area Fig. 4. The relationship between the area of the stimulus field and the amplitudes of the P-ERG and P-VER in four subjects. The abscissa shows the percentage area of stimulusfield,with 12° X 12° expressed as 100%. The ordinate indicates the amplitudes of the P-ERG and the P-VER. The points on the lines show the mean percent amplitudes of the P-ERG (large squares) and the P-VER (large circles) obtained from four subjects (P-ERG, small squares; P-VER, small circles) with five different stimulusfieldsizes. With a central scotoma of 4° X 4° (11% decrease in the full-field stimulus size), the reduction of mean percent amplitude of the P-ERG was only 13%, whereas that of the P-VER was 41%. With a central scotoma of 6° X 6° (area decrease of 25%), the P-ERG and the P-VER decreases were 41% and 48%, respectively. As central scotoma size increased to 8° X 8° (area decrease, 44%), decreases in the P-ERG and the P-VER were 64% and 62%, respectively; at 10° X 10° (area decrease, 69%) decreases in the P-ERG and the P-VER were 77% and 72%, respectively. The percent reductions of the mean percent amplitudes of both the P-ERG and the P-VER were consistently larger than those of percent area decrease at all of the central scotoma sizes, but especially at the central scotoma sizes equal to or smaller than 6° X6°. Discussion Regarding the effect of the overall stimulus field size, we found that with smaller stimulus field sizes the percent amplitude of P-ERG generated was larger than the percentage of stimulus field area (29% amplitude from 11% stimulus field area and 48% amplitude from 25% stimulusfieldarea). At stimulus fields larger than 8° X 8°, the relation became more linear and proportional to the percentage of stimulus field area. These results agree with thefindingsof Armington16 and Hess and Baker15 that P-ERG is fitted by a straight line, indicating linear area summation and Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017 2 4 6 g 10 Central Scotoma Size (Degrees Squared) Fig. 5. (A) The effect of the central scotoma size tested in subject 1. The abscissa shows the central scotoma size in degrees squared and the ordinates indicate the amplitudes of the P-ERG (left) and the P-VER (right). (B, C, D) The effects of the central scotoma size tested in subjects 2, 3, and 4, respectively. 510 INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / March 1990 0 10 20 30 40 50 60 70 80 90 100 (90 80 70 60 50 40 30 20 10 ) % Central Scotoma Area (Remaining % Stimulus Field Area) Fig. 6. The relationship between amplitudes of P-ERG and P-VER and the area of the central scotoma. The abscissa shows the area of central scotoma as a percentage of the full-field stimulus. The number in parentheses indicates the remaining area (percent) of the stimulus field. The ordinate indicates the amplitudes of the P-ERG and the P-VER, with the full-field stimulus (12° X 12° stimulus field) in each subject expressed as 100%. Individual subjects: P-ERG, small squares; P-VER, small circles. Means: P-ERG, large squares; P-VER, large circles. tiveness. In contrast, the P-VER amplitudes (63% from an 11% stimulus field area and 77% from 25% stimulus field area) indicate that the P-VER depends to a greater extent on the macular area. The most striking difference between the P-ERG and the P-VER was saturation in the P-VER. In the P-ERG, there was a weak tendency toward macular dependency, but saturation was not observed in any of the subjects. Katsumi et al14 reported that monocular P-VER with a small check size did not increase beyond a 5° X 5° stimulus field. This saturation can be explained by the total number of elements in the stimulus field and the check size; when the number exceeds a certain level, saturation occurs.20 Perhaps our finding of P-VER saturation with a 6° X 6° or an 8° X 8° stimulus field was due to the relatively large check size (60 min of arc) necessary for reliable PERGs. P-VER was influenced markedly by a 4° X 4° central scotoma, as reported by Katsumi et al,14 whereas P-ERG was less influenced by this size scotoma. With a central scotoma of 4° X 4°, the percentage reduction of the P-ERG amplitude was 13%, while that of the P-VER amplitude was almost 41%. Gronenberg and Teping13 reported that the amplitude of the P-VER from a 4° X 4° stimulus area was larger than that from the peripheral retina outside of it. Our Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017 Vol. 31 study also showed that the P-VER decreased by nearly half, in the presence of the smallest central scotoma. The decreases in the percent amplitude of the P-ERG (41%) and the P-VER (48%) were not significantly different with larger central scotomas, eg, 6° X 6°. Thus, the P-ERG was not as sensitive to a 4° X 4° central scotoma as was the P-VER, suggesting that P-VER has the greater macular dependency of the two recordings. This agrees with Sokol's report that P-VER is a more useful electrodiagnostic index of macular disease than is P-ERG.17 However, our finding that the P-ERG also showed a larger decrease in mean percent amplitude than in percent area may indicate that the P-ERG also has a substantial macular dependency, though not as great as that of the P-VER. This conclusion substantiates the study of Armington and Brigell, who concluded that macular dependency occurred, with a ring stimulus field, because of receptor density and associated anatomic factors of the macula.18 We agree with their explanation. The greater macular dependency of the P-VER compared with that of the P-ERG, as observed in our study, reflects the larger anatomic representation of the macula at the higher visual level. Key words: pattern reversal ERG, pattern reversal VER, stimulusfield,central scotoma, macular function Acknowledgments The authors wish to thank Charles L. Schepens, MD, for his support during this study; Armando Garsd, PhD, for his statistical analysis; and Elizabeth W. Larson and Charlene J. Skladzien for their technical assistance. References 1. Riggs LA, Johnson EP, and Sckick AML: Electrical responses of the human eye to moving stimulus patterns. Science 144:567, 1964. 2. Maffei L and Fiorentini A: Electroretinographic response to alternating gratings before and after section of the optic nerve. Science 211:953, 1981. 3. Dodt E: The electrical response of the human eye to patterned stimuli: Clinical observations. Doc Ophthalmol 65:271, 1987. 4. Papst N, Bopp M, and Schnaudigel OE: Pattern electroretinogram and visually evoked cortical potentials in glaucoma. Graefes Arch Clin Exp Ophthalmol 222:29, 1984. 5. Wanger P and Persson EH: Pattern-reversal electroretinograms and high-pass resolution perimetry in suspected or early glaucoma. Ophthalmology 94:1098, 1987. 6. Weinstein GW, Arden GB, Hitchings RA, Ryan S, Calthorpe CM, and Odom JV: The pattern electroretinogram (PERG) in ocular hypertension and glaucoma. Arch Ophthalmol 106:923, 1988. 7. Dawson WW, Madia MT, and Rubin LM: Human patternevoked retinal responses are altered by optic atrophy. Invest Ophthalmol Vis Sci 22:796, 1982. 8. Seiple W, Price MJ, and Kupersmith M: The pattern electro- No. 3 9. 10. 11. 12. 13. 14. SIMULTANEOUS PATTERN REVERSAL ERG AND VER RECORDINGS / Sokoue er ol retinogram in optic nerve disease. Ophthalmology 90:1127, 1983. Celesia GG and Kaufman D: Pattern ERGs and visual evoked potentials in maculopathies and optic nerve disease. Invest Ophthalmol Vis Sci 26:726, 1985. Spekreijse H: Analysis of EEG Response in Man Evoked by Sine Wave Modulated Light. The Hague, Netherlands, Dr. W. Junk, 1966, pp. 129-140. Sokol S: Visually evoked potentials: Theory, techniques and clinical applications. Surv Ophthalmol 21:18, 1976. Katsumi O, Hirose T, and Larson EW: A new method to measure the pattern reversal visual evoked responses in infants and young children. Jpn J Ophthalmol 30:420, 1986. Gronenberg A and Teping C: Pattern evoked cortical potentials to simultaneous stimulation of both eyes. In Visual Pathways: Electrophysiology and Pathology. Doc Ophthalmol Proc Ser, Vol 27. The Hague, Netherlands, Dr. W. Junk, 1981, pp. 312-321. Katsumi O, Tanino T, and Hirose T: Objective evaluation of Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017 15. 16. 17. 18. 19. 20. 511 binocular function with pattern reversal VER III: Effect of stimulus size and localization. Acta Ophthalmol 64:691, 1986. Hess FR and Baker LC: Human pattern-evoked electroretinogram. J Neurophysiol 51:939, 1984. Armington JC: The electroretinogram, the visual evoked potential, and the area-luminance relation. Vision Res 8:263, 1968. Sokol S: An electrodiagnostic index of macular degeneration. Arch Ophthalmol 88:619, 1972. Armington JC and Brigell M: Effects of stimulus location and pattern upon the visually evoked cortical potential and the electroretinogram. Int J Neurosci 14:169, 1981. Yanashima K and Okisaka S: Design of disposable ERG electrode utilizing a hydrophilic soft contact lens with high water content. Folia Ophthalmol Jpn 37:777, 1983. Katsumi O, Hirose T, and Tsukada T: Effect of number of elements and size of stimulus field on recordability of pattern reversal visual evoked response. Invest Ophthalmol Vis Sci 29:922, 1988.