Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Idiopathic intracranial hypertension wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
Contact lens wikipedia , lookup
Corrective lens wikipedia , lookup
Macular degeneration wikipedia , lookup
Retinitis pigmentosa wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
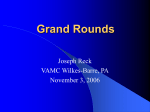
Retina 6th EURETINA Congress Symposium Report Gisbert Richard Peter Barry Roibeard O’hEineachain in Lisbon THIS year’s EURETINA meeting included a joint EURETINA/ESCRS symposium on where anterior segment and posterior segment surgery meet. Commencing the session, co-chairman, Gisbert Richard MD, University Medical Centre Hamburg-Eppendorf, described a combined surgery procedure for cataract patients who require pars plana vitrectomy (PPV) for such indications as epiretinal membranes, macular holes and diabetic retinopathy. He noted that PPV can induce cataract and a progressive myopisation in a high proportion of patients. Combining PPV with cataract surgery can eliminate those problems. However, the two procedures have contradictory requirements. PPV requires a closed system that will tolerate an increased IOP whereas cataract surgery requires opening of the eye, he said. To meet the conflicting requirements of the PPV and cataract surgery, Dr Richard has adopted a combined approach that employs a long corneoscleral tunnel.The procedure commences with the fixation of two eye muscles and the precise creation of a corneoscleral tunnel at least 3.5mm in length through which both PPV and cataract extraction are performed. “A combined approach using a corneoscleral tunnel tolerates the pressure increase while at the same time allowing an opening large enough for cataract surgery,” he said. Results similar to sequential approach Dr Richard presented his results using the combination technique in a wide range of indications His findings suggest the technique can achieve visual outcome comparable to non-combined surgery. He noted that in a consecutive series of 230 patients with epiretinal membranes visual acuity improved postoperatively in 82% of eyes, remained unchanged in 7% and became worse in 11%. Complications included posterior synechiae in four eyes. In 130 eyes with macular holes the combined procedure brought about macular hole closure in 86% of eyes and an improvement of two lines or more in visual acuity in 75%.There were no problems with peeling the internal limiting membrane, he 26 Where anterior segment and posterior segment surgery meet added. Complications included a temporary increase in IOP in 16%, an increase in astigmatism in two per cent, and retinal detachment in four per cent. In 140 eyes that underwent the combined approach for retinal detachment due to diabetic retinopathy, the retina was successfully re-attached in 90% of eyes and visual acuity improved in 73%. However, residual peripheral detachment was present in 10% of eyes; posterior synechiae occurred in 13%; vitreous haemorrhage occurred in 10%; and iris capture in three per cent.There was also an increased incidence of secondary cataract formation. “Opening of the anterior chamber via a corneoscleral tunnel meets the contradictory requirements of anterior and posterior segment surgery, making combined surgery safe and efficient provided there are no severe disturbances of the blood-retinal barrier.” IOL luxation into the vitreous Dr Richard’s associate Oliver Zeitz MD followed with his insights into the management of IOL luxation. Estimates of the incidence of IOL luxation range from around 0.2% to 1.8%, Dr Zeitz noted. Approximately 60% of luxations occur in the first two weeks after cataract surgery. The complication occurs more commonly in IOLs with a plate haptic design and can result from defects of the posterior capsule or zonular fibres,YAG capsulotomy, and trauma. The time to surgery does not appear to influence visual acuity outcome, therefore simple observation is one option to consider, he pointed out. However, possible complications of luxated IOLs include decreased vision, glare, iritis, secondary glaucoma, retinal detachment and cystoid macular oedema. On the other hand, surgery also carries a fairly significant risk of cystoid macular oedema, retinal detachment and secondary glaucoma. Other less common complications of surgery include diplopia, pigmented disciform scar and vitreous haemorrhage, he noted. “There is no strong need to perform surgery, but if you decide to do it, do it completely and without any compromise,” he added. Repositioning or removal Surgical options include re-positioning the lens or removing and replacing it, with or without PPV, he said. Repositioning the IOL has the advantage of being less invasive and having a lower rate of complications. However, repositioning of the luxated IOL also carries a higher risk of recurrence due to insufficient fixation of the repositioned lens. IOL removal and replacement is called for in cases where the IOL has been damaged or it has an incorrect refractive power. In many cases PPV is not required for repositioning and even removal and replacement of a luxated IOL. PPV becomes necessary if the IOL is luxated deeply into the posterior segment or if substantial amounts of vitreous envelope the IOL. Dislocated IOLs can be mobilised by intraocular forceps or other instruments or through elevation in the vitreous cave by the injection of heavy fluids. IOLs can be removed through a limbal or scleral pars plana incision. Dr Zeitz recommended a limbal approach since it is less likely to result in complications. Means of restoring good visual acuity in eyes where the IOL has been removed include contact lenses, retropupillary irisclaw anterior chamber IOLs, scleral-fixated lens and, if a substantial amount of the capsule remains, posterior chamber IOLs. “Visual acuity outcome is equivalent for all visual rehabilitation approaches.The major limiting factors are co-existing ocular pathologies,” he said. The dropped lens Peter Barry FRCS, Dublin, Ireland, discussed strategies for dealing with the dropped lens. “I think all of us have had the experience of dropping a nucleus whilst performing cataract surgery.You all know the sense of despair; you panic and feel somewhat embarrassed.You hope that nobody will really notice what’s happening. But then you actually realise that you’ve made a mistake, you’ve got a problem, and you have to face up to it.” Possible consequences of such events include corneal failure, uveitis, glaucoma, vitritis, cystoid macular oedema, and retinal detachment.The challenge for the surgeon is to avoid those complications and remove the dropped lens and implant an IOL in the capsular bag, Dr Barry said. Experienced cataract surgeons can achieve this by first performing a closed anterior vitrectomy, aspirating the soft lens material while at the same time being very careful to preserve capsular remnants. “Less experienced surgeons are sometimes in a hurry to complete this part of the procedure but it should really be the other way around: slow down, do your anterior vitrectomy and tease out the residual lens cortex with very low infusion and ensure that you preserve the capsular bag remnants in order to achieve lens implantation.” Vitreoretinal surgeons can use the alternative technique of pars plana vitrectomy, again aspirating the soft lens material, using a fragmatome in denser cataracts.The use of viscoelastics should be avoided with this approach because it is difficult to remove following vitrectomy. With both approaches a posterior chamber IOL can usually be successfully implanted although sometimes it will need to be implanted in the sulcus, Dr Barry added. Effects of cataract surgery on the macula Conceição Lobo MD, Coimbra, Portugal discussed the effects of cataract surgery on the macula. She noted that angiographic CME occurs in about 20% of eyes undergoing such procedures, although it becomes symptomatic in only around 1-2%. Dr Lobo recommended mapping of the macula with a multimodal approach to characterise the condition’s features and assess treatment in patients in whom it affects vision. She presented a study in which she and her associates used multimodal macular mapping in 32 patients who had undergone phacoemulsification and IOL implantation. The approach involved a combination and integration of fluorescein angiography, Retinal Leakage Analysis (RLA) Retinal Thickness Analysis (RTA/OCT). The study showed that leakage reached its maximum at 12 weeks and was present in 88%. Retinal thickness peaked at six weeks, when it was increased in 41%. By 30 weeks leakage was present in only 68% and retinal thickness was increased in only 28%.Visual acuity followed a similar pattern.That is, visual acuity of 8/10 or better was achieved by 81% at three weeks, 88% at 12 weeks and 91% at 30 weeks. Prevention of PCO Dr Marie-José Tassignon MD, University Hospital Antwerp, Belgium, followed with a presentation describing the latest results with the bag-in-the-lens IOL.The lens is specifically designed to prevent posterior capsule opacification. Patients who are to be implanted with the lens first undergo anterior and posterior capsulorhexis, Dr Tassignon explained.The rims of the IOL’s specially designed haptics clasp the edges of the remaining capsular bag together. In this way the lens prevents lens epithelial cell migration and PCO. In addition, the anterior and posterior haptics are oriented perpendicularly to each other in order to prevent the tilting, rotation or decentration of the lens. Dr Tassignon has implanted the IOLs in over 600 eyes, 25 of which were paediatric cases. She noted that in all eyes with a follow-up of at least one year the optic portion of the lens has remained clear and none have required a YAG capsulotomy. Furthermore, in a study which compared the results of implantation of the bag-in-the lens IOL in 100 patients and 100 patients implanted with a conventional IOL made of the same hydrophilic acrylic material, none of the eyes with the bag-in-the-lens IOL required YAG laser capsulotomy after a follow-up of four years, compared to YAG capsulotomy rate of 41.18% in the conventional IOL group. “The results make it 100% clear that with the bag-in-the lens IOL you have no PCO whatsoever.” To further optimise the placement of the IOL, Dr Tassignon has designed a ring-shaped calliper to guide the surgeon in the creation of the anterior capsulorhexis.The more precise centration and sizing of the capsulorhexis that the device affords may in turn improve the stability of the IOL. “When IOL rotation and centration is under control spherical aberration and toric correction can be introduced,” she added. A version of the Three years after implantation, no opacification of the central area can be seen lens in which the optic can be light perception or better vitrectomy exchanged in subsequent procedures is now produces better results. under development.The new lens could be of The EVS also showed that intravitreal particular benefit to paediatric patients. antibiotics such as vancomycin and amikacin Future modifications of the lens may make it were effective in bringing about a resolution possible for patients to achieve a degree of of the condition.Another finding was that the accommodation, Dr Tassignon said. systemic intravenous antibiotics used in the study (cephalosporins and aminoglycosides) Treatment of endophthalmitis produced no apparent benefit. William F Mieler MD, University of Chicago, However, recent studies suggest that Chicago, Illinois, US, discussed the current newer, fourth generation fluoroquinolones thinking on the treatment of endophthalmitis. such as gatifloxacin and moxifloxacin may be “This field is rapidly changing and there are effective in the treatment of endophthalmitis many questions that remain unanswered at when administered orally, Dr Mieler pointed this point in time as to our true best out. management.We like to recommend “These are agents that penetrate inside treatment based on evidence-based medicine the eye very readily when given orally even in but in some cases we don’t have all the non-inflamed eyes,” he added. answers.” In a study involving patients undergoing He noted that the Endophthalmitis elective vitrectomy, oral administration of Vitrectomy Study (EVS) showed that vitreous gatifloxacin achieved a maximum vitreous tap and vitrectomy had equivalent results penetration that exceeded the MIC90 for all when the affected patient had hand the Gram-positive microorganisms except movements or better. If the patient’s vision is enterococcus.The agent also achieved the Courtesy of Marie-José Tassignon MD Retina MIC90 levels for most of the Gram-negative organisms except pseudomonas. Gatifloxacin was recently withdrawn from the market as an oral agent due to its adverse effect on blood-sugar control. However, it is still available for topical use as eye drops. Moxifloxacin, which is still on the market for oral use, provides an even better spectrum of control and achieves a concentration in the vitreous cavity that is 38% of that of serum concentration. In addition the agent appears to be safe in the eye at concentrations 500 times as high as the MIC90 for the most commonly encountered microorganisms. “Exciting significant advances have been made in the treatment of proven infection, and in the prophylaxis against development of infection. Numerous additional changes are forthcoming,” he commented. [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] 27