Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Vision therapy wikipedia , lookup
Keratoconus wikipedia , lookup
Visual impairment wikipedia , lookup
Contact lens wikipedia , lookup
Corrective lens wikipedia , lookup
Blast-related ocular trauma wikipedia , lookup
Corneal transplantation wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
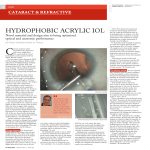
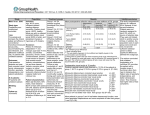
Comparative Study of the Aspheric Akreos Adapt AO IOL Versus the Spherical Akreos Adapt IOL Maghizh Anandan Martin Leyland Purpose • Standard IOL’s provide good visual acuity but they often increase spherical aberration and reduce contrast sensitivity. • This study compares the optical performance of the aberration free Akreos Advanced Optic IOL (AO) with the conventional spherical Akreos Adapt IOL (AA). Methods • Twenty five patients requiring bilateral cataract surgery were enrolled in to this prospective, intra-individual comparative study. • One eye received the AO lens and the other eye the AA control lens according to the randomisation table. • Study was double masked. Neither the patients nor the examiner at the post-op visit knew which eye had the aspherical IOL. • Quality of vision was tested by visual acuity, contrast sensitivity and ‘quality of vision’ questionnaire • All patients were operated on by the same surgeon (M.L) using the same technique and were followed up for at least 3 months • Written informed consent was obtained from all patients before surgery, and the study was approved by the local ethics committee. • Preoperative and postoperative evaluations included uncorrected distance visual acuity, (BSCVA), spherical equivalent (SE), slitlamp biomicroscopy, applanation tonometry, fundus examination, B-scan biometry • Clinical data were collected preoperatively and 1 and 3 months postoperatively. – Unaided and best spectacle-corrected visual acuity , contrast sensitivty Contrast sensitivity • Contrast sensitivity was measured using SIFIMAV test screen, containing sinusoidal gratings of 5 spatial frequencies with 8 contrast sensitivity levels each. • The examinations were performed unilaterally at a distance of 2.5 m with BSCVA and an un-dilated pupil. All measurements were performed under the same conditions by an examiner who was unaware of the type of IOL implanted. Questionnaire • All patients were given a questionnaire at the last follow-up • The questionnaire was designed to determine whether a patient was experiencing any form of dysphotopsia in any of the eye (Light-caused glare, Increase in eye sensitivity, Unwanted images) • If the patients said yes to the above in any/both eye they will answer further questions to determine the nature and level of dysphotopsia by points system. • Light related glare was scored as 0 if none, 1 for minimal, 2 for annoying and 3 for debilitating. – This questionnaire was been developed by Tester and co authors (Dysphotopsia in phakic and pseudophakic patients : incidence and relation to intraocular lens type.J. Cataract Refract Surg 2000; 26: 810-816) Analysis • For statistical analysis of visual acuity, logarithm of minimum angle of resolution (logMAR) acuity values were used. • Similarly, the recorded contrast sensitivity values were transformed into log values. • The 2 IOLs were compared between eyes intra-individually. • P value less than 0.05 was considered statistically significant. Results • 46 eyes of 23 patients were included in the study • 2 patients died after bilateral surgery but before assessment were completed and hence excluded from study • 7 patients(30%) were men, and 16 (70 %) were women • The mean age was 77 years (range 68 to 90 years). • All patients completed the 3-month follow-up. • There were no intra-operative complications • 16 eyes underwent limbal relaxing incisions (7 in AO group and 9 in AA group) Visual acuity Pre-operative Mean logMAR BSCVA was 0.49 AA and 0.45 AO (P = 0.67) Post-operative (3 months) Mean logMAR unaided VA was 0.20 AA and 0.24 AO (P = 0.60) Mean logMAR BSCVA was 0.06 AA and 0.07 AO (P = 0.57) Mean sperical equivalent refraction -0.37 AA and -0.20 AO (P = 0.60) Contrast sensitivity AA IOL AO IOL P value 1.5 cpd 1.37 1.32 0.22 3 cpd 1.59 1.63 0.46 6 cpd 1.64 1.65 0.89 12 cpd 1.20 1.25 0.61 18 cpd 0.87 0.91 0.74 There was no statistical differences in any of the spatial frequencies Questionnaire - Analysis • No statistical difference in light-related glare score in either of the IOL • Both lens performs well and patients were generally very satisfied • Two out of 11 patients who drive found it difficult to drive at night due to glare ( One in each IOL type). AO IOL AA IOL Glare scoring 1.94 1.78 Glare % 42.1% 42.1% Sensitivity % 36.8% 36.8% Unwanted images % 31.5% 21% Conclusion • No statistically significant differences were found between aspherical and spherical IOLs in postoperative VA and refraction. • Contrast sensitivity was performed with an un-dilated pupil and best spectacle correction in normal room light condition to create a more real life situation. There were no statistical differences at any of the spatial frequencies. • The questionnaire analysis showed that the patients in our study were very satisfied with the quality of vision with both IOLs, with a low incidence of adverse visual phenomena. Discussion • Standard intraocular lenses have a positive spherical aberration (SA) that, when added to the positive SA in the normal cornea, increases ocular SA. Aspherical IOLs have been designed to compensate for the positive SA of the cornea • Advanced Optics (AO) aberration-free aspheric intraocular lens is a Hydrophilic acrylic lens with a 360-degree square edge. Both the anterior and posterior surfaces are aspheric and are designed so that the lens itself has no spherical aberration. • Theoretical advantages of this IOL – Does not contribute to any pre-existing higher-order aberrations as its surface is aspherical – If the IOL is decentered it does not induce other aberrations, such as coma or astigmatism • There are other lenses on the market with negative spherical aberration, which are designed to offset the average corneal spherical aberration. • One has to remember when using such lenses, that in some cases of highly prolate corneas, the patient will have an end result of considerable negative spherical aberration rather than a neutral offset. Discussion • We made a significant effort to reduce the bias that can occur in comparative clinical studies by making our study an intra-individual comparison, using the same IOL material manufactured by the same company, and having the same surgeon perform bilateral surgery using an identical surgical technique. • Many studies have shown better contrast sensitivity measurements with aspherical IOL especially in mesopic conditions. We performed the contrast sensitivity with an un-dilated pupil and best spectacle correction only in normal room light condition. This may be the reason why we did not show any statistical difference in contrast sensitivity but when asked which eye the patient preferred in terms of overall vision, only 33.3% were AO IOL’s. Therefore, it remains questionable whether any significant differences in contrast sensitivity have clinical relevance and what it means for the patient. • In a recent large multicenter study Akreos Adapt Advanced Optics (SA 0.00 μm, Bausch & Lomb Inc) and Tecnis Z9000 (SA −0.27 μm, Advanced Medical Optics, Inc.), were compared. The differences in eye preference and visual disturbance between the 2 IOLs favored the Akreos AO. This was interesting considering the results of the wave-front analysis, in which the total higher order aberration, in particular the spherical aberration, was significantly lower in eyes with the Tecnis Z 9000 IOL. They concluded that maximum reduction of spherical aberration does not correlate with the perceived visual quality of the eye having surgery. Discussion • Limitations of our study are that, we could not perform wave front analysis on all patients and hence not included in the analysis. However this would have been only theoretical as several studies have shown that better final spherical aberration does not correspond to better vision. • Contrast sensitivity was not performed in mesopic conditions for comparison but we included specific questions about night vision including driving at night, in the questionnaire to ascertain the quality of vision and contrast in mesopic conditions and found no statistical differences. • Another limitation is that this study assumed that the IOLs were well centered and not tilted; decentration of IOLs induces coma, which may affect the final outcome in that eye. Discussion • The design of this study, with bilateral surgery and randomized implantation of the 2 IOLs, was chosen to minimize the effects of factors other than the IOLs such as ocular dominance or refraction deviations, which could affect the outcomes. The double-masking also likely minimized bias, particularly in the results of the patient questionnaires. • Despite this, we found no differences between the IOLs in low-contrast visual acuity or contrast sensitivity. • The patients' awareness of having different IOLs in the right eye and left eye may have increased their awareness of minor differences between the eyes. Still, about half the patients reported no difference between the eyes, which is probably because of the patients' high level of overall satisfaction with the surgical results, visual improvement, and IOL performance. • In summary, the Akreos AO IOL and Akreos IOL gave similar contrast visual acuities as well as photopic contrast sensitivities. • • • Refrences: L. Wang et al, Optical aberrations of the human anterior cornea, J Cataract Refract Surg 29 (2003), pp. 1514–1521. Visual and optical performance of the Akreos Adapt Advanced Optics and Tecnis Z9000 intraocular lenses Swedish multicenter study, Journal of Cataract & Refractive Surgery , Volume 33, Issue 9, September 2007, Pages 1565-1572 Custom optimization of intraocular lens asphericity Journal of Cataract & Refractive Surgery , Volume 33, Issue 10, October 2007, Pages 1713-1720 Optical performance of 3 intraocular lens designs in the presence of decentration, J Cataract Refract Surg 31 (2005), pp. 574–585. Effect of decentration of wavefront-corrected intraocular lenses on the higher-order aberrations of the eye, Arch Ophthalmol 123 (2005), pp. 1226–1230. Ocular aberrations and contrast sensitivity after cataract surgery with AcrySof IQ intraocular lens implantation Clinical comparative study.J Cataract Refract Surg. 2007 Nov;33(11):1918-24. • • • •