Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
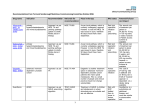
EBR*Summer 2009 25/6/09 08:17 Page 8 BioFinance and Management Market Access in the Wake of NICE: BioPharma’s Friend or Foe? Joshua Cohen at the Tufts Center for the Study of Drug Development reviews the impact of NICE on drug development, considering the effect it has had on the biopharmaceutical industry on a global, as well as national, scale Spending on pharmaceuticals across the Organization for Economic Cooperation and Development (OECD) countries has increased by close to 50 per cent in real terms since 1998. Growth in spending has been driven to a large extent by newer and more expensive drugs replacing older therapies. As a consequence, public and private payers are considering whether to (conditionally) reimburse newer and (usually) more expensive drugs. Effectively, payers are imposing a fourth hurdle that biopharmaceutical firms must clear in order to attain widespread market access, the first three being safety, efficacy and quality of manufacturing practices. The establishment of a fourth hurdle is a phenomenon that began in Australia in the early 1990s, and has since spread to other jurisdictions, particularly in Europe, each with its own ways of conducting technology assessment and implementing results. Even the world’s largest market for biopharmaceuticals, the US, has not been bypassed by the fourth hurdle: although considered to lag behind compared to other nations, a de facto fourth hurdle has been instituted. Among watershed events in the past five years, we have seen the enactment of federal regulations that allow cost and clinical evidence to be considered in outpatient drug reimbursement decisions affecting Medicare beneficiaries. Also, the Centers for Medicare and Medicaid Services (CMS) have stated that FDA authorisation is insufficient to support reimbursement decisions for certain physician-administered drugs, such as the erythropoesis-stimulating agents covered under Medicare Part B. And, in the private sector, the Academy of Managed Care Pharmacy (AMCP) trade group has issued detailed guidelines specifying precise parameters to be included by drug sponsors in the formulary dossiers they submit to payers for the purposes of reimbursement. 8 But of all developments surrounding the fourth hurdle, none has had such farreaching implications as the establishment of the National Institute for Health and Clinical Excellence (NICE) in England and Wales in 1999. NICE has become the world’s most prominent appraiser of new medical technologies, including drugs and biologics. This article will evaluate its decision-making process, the controversial cases that have drawn media attention, and recent initiatives aimed at streamlining NICE assessments, concluding with an analysis of policy implications and the global ramifications of NICE. OVERVIEW OF THE NICE DECISION PROCESS NICE is a governmental organisation that functions in an advisory capacity to the British National Health Service (NHS). It is responsible for providing guidance on the “promotion of good health and the prevention and treatment of ill health” in England and Wales. In particular, NICE produces guidance with respect to: G G Health technologies – the use of new and existing medicines, diagnostics, treatments and procedures Clinical practice – appropriate treatment and care of patients with specific diseases and conditions Broadly, NICE’s stated goals are to rationalise clinical care and eliminate inequities by geographic area. NICE’s raison d’être is premised on the oft-cited ‘tragedy of the commons’: resources are scarce but competing demands on them are infinite. A patient acts rationally in seeking an expensive treatment that produces a benefit (even if small) because the cost falls almost entirely on others. The same can be said for doctors who seek the best care for their patients as the costs, in terms of fewer resources for other patients, fall almost entirely on other doctors’ patients. Ultimately, however, from a societal perspective, to ensure efficient resource allocation, it is required that an intervention’s health benefits are greater than their opportunity cost, or the value of the next best alternative is limited. NICE tackles this resource allocation problem by evaluating the costs, benefits and risks of new medical technologies, and recommending resource allocation accordingly. NICE does not commission primary research; instead, it bases its recommendations on systematic analyses and economic modelling. The costeffectiveness technique used by NICE to assess different treatments – cost-perquality-adjusted-life-year (QALY) – facilitates system-wide comparisons across a wide range of treatments. This ratio incorporates the added cost of a treatment over the current standard therapy, set against the additional health benefits conferred by the treatment. Besides cost-effectiveness, equity considerations such as the burden of disease and the rule of rescue may inform reimbursement and use decisions, with treatments that target more severely impairing diseases generally being prioritised. NICE has published approximately 150 guidances covering over 200 different drugs and medical devices. Approximately 50 per cent of assessed technologies are recommended for reimbursement and use in all licensed indications. About 40 per cent are conditionally recommended (for example, only for specific indications, patient subgroups, or as step therapy), and 10 per cent are not recommended at all for reasons related to lack of clinical or cost-effectiveness (1). Technologies supported by more randomised trial evidence are more likely www.samedanltd.com EBR*Summer 2009 25/6/09 08:18 Page 10 Table 1: Controversial cases Product(s) Date of decision Summary decision Aricept, Exelon, Reminyl 2006 NICE recommends against use of all three cholinesterase inhibitors to treat Alzheimer’s disease Avastin 2008 NICE recommends against first-line use to treat kidney and colorectal cancer Erbitux 2007 NICE recommends against use in colorectal cancer Lucentis 2007 NICE recommends against use to treat wet agerelated macular degeneration Sutent, Revlimid 2008 NICE recommends against use to treat advanced kidney cancer in new patients Tarceva 2008 NICE recommends against use to treat non-small cell lung cancer Tykerb 2009 NICE recommends against use to treat advanced breast cancer Velcade 2006 NICE recommends against use in multiple myeloma to be recommended for reimbursement and use. In addition, the earlier technologies are appraised, the less likely they are to be rejected. Moreover, the higher the burden of disease, the more likely a technology is to be recommended. At the same time, higher cost-effectiveness ratios increase the probability of rejection: the more uncertainty that exists concerning a technology’s cost-effectiveness ratio, the less likely it is to be recommended for reimbursement and routine use (2). NICE as justification for not spending limited resources on that treatment” (3). Moreover, delays between licensing and reimbursement have led to a phenomenon called ‘NICE blight’: NHS trusts hold back decisions to fund technologies pending publication of guidance recommendations by NICE. Herceptin is a case in point. NICE took 18 months to appraise the drug before it recommended its reimbursement and use. During that period many trusts did not fund its use. There is no evidence to suggest that overall drug spending or its growth rate has been reduced in England and Wales. In fact, NICE recommendations have turned out to be largely positive, which has increased the NHS drug budget. This increase is due, in part, to the statutory obligation of the NHS to provide funding for NICE-recommended drugs. Nonetheless, if NICE recommends against reimbursement and use of a pharmaceutical, the practical effect is that it will be unavailable to patients. This is because, in most instances, the 150 primary and 170 acute care NHS trusts, acting as local health care purchasers, will “point to the guidance issued by As we can see from the abbreviated list of controversial cases in Table 1, biotechnology drugs appear especially vulnerable when cost-effectiveness enters the equation, as they are often being compared to relatively old and usually inexpensive medications. In NICE’s preliminary analysis, Velcade, for example, was compared with off-patent dexamethasone. In this respect, NICE can be viewed as less of a foe to traditional pharmaceutical than to biotechnology companies. NICE INITIATIVES A coalition of drug sponsors and citizen groups have appealed against Table 2: NICE changing its tune Product(s) Date of decision Summary decision Aricept, Exelon, Reminyl 2007 NICE recommends reimbursement and use, but only for moderate and severe states of Alzheimer’s Lucentis 2008 NICE recommends reimbursement and use for the first 14 treatments, after which sponsor agrees to pay for treatment Sutent, Revlimid 2009 NICE recommends NHS pay first two years of Revlimid, after which sponsor will pay. NICE recommends NHS pay for follow-up cycles of Sutent after sponsor has paid for the first six-week cycle Velcade 2008 NICE recommends use in treatment of multiple myeloma in individuals who have relapsed after one prior therapy. However, recommendation is accompanied by an agreement that patients with no or minimal response after four cycles of treatment will be taken off Velcade. Sponsor will then rebate the full cost of the drug. 10 approximately 30 per cent of all NICE decisions. To illustrate, all eight decisions summarised in Table 1 were appealed. In response to heightened criticism, NICE is implementing faster appraisals, especially for drugs likely to be major innovators – those given priority status by regulators. Some appraisals are even being conducted in parallel with licensing. NICE is also altering its cost-effectiveness criteria so more biopharmaceuticals for terminally ill patients can be recommended for coverage. The new appraisal criteria effectively raised the cost-effectiveness threshold for certain products; specifically drugs with a costeffectiveness ratio greater than £30,000 per QALY, drugs licensed for a patient population with life expectancy less than 24 months, and drugs targeting a disease in which no more than 7,000 new patients are diagnosed per year. Recent decisions reflect changes at NICE (see Table 2). These decisions illustrate NICE’s role at the forefront of introducing both risk-sharing arrangements and value-based drug pricing. The former concerns schemes in which the payer and manufacturer split the (potential) cost of a new or unproven therapy (4). The latter allows payers to pay more for patients whose likely benefit is greatest and less for indications where there is less potential benefit. LESSONS TO BE DRAWN FROM NICE EXPERIENCE There is consensus among stakeholders that it is useful to make decisions about reimbursement and use of newly approved drugs on a rational, data-driven basis. Also, there is agreement that the technical quality of NICE assessments is world class. Pricing specialists suggest that cutting case-by-case deals with NICE, such as the ones enumerated in Table 2, is a better cost containment option than across-the-board price ceilings. As a result, NICE methods, as well as its organisational model, have become a beacon to governments and payers wrestling with the issues of resource allocation and fairness in healthcare delivery. Even if critics may not appreciate its role in rationing, everyone sees value in having an independent, even-handed and trustworthy body to turn to when different courses of action are being weighed. www.samedanltd.com EBR*Summer 2009 25/6/09 08:19 Page 12 Indeed, we see NICE’s influence already being felt with its impact reaching as far as the comparative effectiveness debate in the US. Technology appraisals have become almost universal in developed countries, partly due to the path blazed by NICE. Nevertheless, there are important limits to NICE’s influence. Firstly, only in England and Wales have the kinds of technology appraisals that NICE conducts been fully integrated with decision making, legally binding, national in scale, and put into practice in a system with a single payer. Secondly, besides Canada and Australia, no other technology assessment authority employs the cost-per-QALY method as extensively as NICE. Though superficially similar to NICE, the German Institute for Quality and Efficiency in Healthcare (IQWiG) does not use QALYs, but instead resorts to other evaluation methods. Its mandate is to address benefits relative to costs for a given indication, and not to set funding priorities across the healthcare system. Likewise, the French National Authority for Health does not utilise the cost-per-QALY method, and applies pricevolume agreements per newly approved drug to contain costs. Detractors point to the cost-per-QALY method as befitting a one-size-fits-all approach, which is tilted against medications targeting life-threatening conditions, such as cancer, in particular when they are labelled for use in advanced or metastatic disease. Indeed, we can observe that the UK lags behind many other European nations in terms of uptake of new cancer drugs, which may have to do with negative decisions by NICE (5). Moreover, what is cost-effective in one country is not necessarily cost-effective in another, due in part to income differences, but also the fact that healthcare priorities inevitably differ. All this makes it highly unlikely that a ‘Euro-NICE’ would be established in the short term. While NICE has been mentioned by policymakers in the US debating comparative effectiveness, it is both premature and inaccurate to suggest that the US will follow NICE’s lead. Cost has not (yet) been permitted to enter the comparative effectiveness equation in the US, nor is any entity entrusted to carry out analyses allowed to make recommendations on 12 About the author Joshua Cohen investigates public policy issues that relate to prescription drug reimbursement. He joined Tufts CSDD in 1999. His specific areas of research include pharmacy benefits management as it relates to the Medicare prescription drug benefit, formulary standards established by the Centers for Medicare and Medicaid Services to ensure adequate access to prescription drugs for Medicare beneficiaries, comparison of formulary management and pharmacoeconomic assessment in the US and Europe, prescription to over-the-counter switches, and the role of follow-on drugs on the World Health Organization’s Essential Drug List. Prior to joining Tufts CSDD, he completed a post-doctoral fellowship at the Veteran Affairs Medical Center in Philadelphia, while simultaneously serving as a Research Fellow at the University of Pennsylvania’s Leonard Davis Institute for Health Economics. He received his doctoral degree in economics from the University of Amsterdam in 1997. Email: [email protected] reimbursement and the use of products yet. There is also an ideological difference. NICE aims to have guidance that applies equitably across NHS trusts in England and Wales. This contrasts sharply with the individualised US approach to formulary management. The cost-per-QALY method delineates an arbitrary cut-off between technologies the NHS can afford for all, as opposed to those it will fund for (virtually) no one (6). As such, it represents an approach, however controversial, to dealing ‘fairly’ with each group of patients, ensuring everyone gets an equal share of the pie. This approach to fairness does not resonate as much in the US. In fact, policymakers may see virtue in variation. To illustrate, if one US insurer does not reimburse a certain drug, a person can theoretically go elsewhere for coverage. In one study we conducted, concerning 71 drugs NICE has evaluated, all nine drugs NICE recommended against were on the formularies of at least one of the US plans we examined (7). CONCLUSION The use of cost-effectiveness evidence in decisions about the adoption of new technologies, such as drugs and biologics, has become widespread internationally over the past decade and a half. The fourth hurdle is seen by some as an onerous barrier, while others see it as a facilitator of equitable access. Its most prominent executor, NICE, has extended its influence beyond the borders of England and Wales. NICE could have more influence if there were less controversy, and, ironically, if contestable decisions were more evidencebased. In this vein, it makes sense to allow access to drugs while the real-world evidence base for their use is augmented. Such a ‘coverage with evidence development’ model, as demonstrated by the novel risk sharing arrangements, for example, would mitigate NICE blight and also expand patient access to potentially innovative treatments. References 1. Raftery J, Review of NICE’s recommendations, 1999-2005, British Medical Journal 332: pp1,266-1,268, 2006 2. Dakin H, Devlin N, and Odeyemi I, “Yes,” “No,” or “Yes, but”? multinomial modeling of NICE decision-making, Health Policy 77: pp352-367, 2006 3. Syrett K, A technocratic fix to the legitimacy problem: The Blair government and health care rationing in the United Kingdom, Journal of Health Politics, Policy and Law 28: pp715-746, 2003 4. Note: NICE has not accepted all compromises offered by drug sponsors. For example, in April 2009 NICE asserted that Tykerb was “not a cost-effective use of NHS resources” at £94,000 per QALY, despite GlaxoSmithKline offering to pay for the first 12 weeks of treatment 5. Jonsson B and Wilking N, A global comparison regarding patient access to cancer drugs, Annals of Oncology, supplement 3: pp1-75, 2007 6. Personal communication, William Looney, Pfizer Corporation 7. Cohen J, Cairns C, Paquette C and Faden L, Comparing patient access to pharmaceuticals in the UK and US, Applied Health Economics and Health Policy 5(3): pp177-187, 2006 www.samedanltd.com WT_Ad