Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
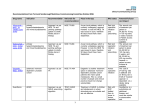
AGENDA ITEM BOURNEMOUTH AND POOLE PRIMARY CARE TRUST PAPER FOR HEALTH AND SCRUTINY PANEL APRIL 2007 HOW THE NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE (NICE) DEVELOPS GUIDANCE ON THE USE OF NEW AND EXISTING DRUGS WITH SPECIFIC RELATION TO THE TREATMENT OF ALZHEIMERS DISEASE (NICE TECHNOLOGY APPRAISAL TA 111, NOVEMBER 2006) 1. BACKGROUND 1.1 This short paper is intended to provide members with an overview of some important issues in relation to the treatment of Alzheimer’s disease with medical therapies. It draws on the recent technology appraisal by the National Institute for Health and Clinical Excellence (NICE). The institute reviewed its guidance in November 2006 on the use of three drugs known as acetyl cholinesterase inhibitors for treatment of Alzheimer’s disease, donepezil, galantamine and rivastigmine, plus a newer drug, memantine, for moderate to severe Alzheimer’s disease. 1.2 The main purpose of this paper is to summarise the NICE guidance, by which all PCTs are bound by in making decisions about effectiveness and cost-effectiveness of health technologies. 2. WHAT DID THE NICE TECHNOLOGY APPRAISAL FIND? 2.1 All three of the acetyl cholinesterase inhibitors (donepezil, rivastigmine and galantamine) appeared to benefit patients with mild to moderately severe Alzheimer’s disease when assessed for signs of improved cognition and global function. But these improvements were small and few trials assessed the effects beyond 26 weeks. In general, higher doses of all the drugs appeared to be more beneficial than lower doses. 2.2 None of the drugs was shown consistently to improve measures of mood, quality of life, improve activities of daily living or behaviour – which may be more important than cognition in terms of overall everyday function. 2.3 Most trials included a range of patients (from extremely mild to severe disease) and drug doses. This meant that it was difficult to compare effects directly between mild patients and those with more severe disease, and between patients on different dose regimens. 2.4 None of the drugs was found to be cost-effective for treatment of mild to moderate Alzheimer’s disease. NICE uses a measure called a QALY (quality adjusted life year) to set a benchmark of cost-effectiveness, which enables different health technologies to be compared. When a QALY costs more than £30,000 the intervention is not considered cost-effective. The three drugs ranged from £58,000-80,000 per QALY. 2.5 The trials suffered from a number of problems with their methods that could lead to biases that may overestimate the effectiveness of the drugs. The most important problems were a lack of blinding (i.e. the investigators were often aware which patients were taking the drugs, and which were not), and drop out of participants because of side effects of the drugs. 2.6 NICE recommended in view of these findings that the drugs are used as options in the management of people with moderately severe Alzheimer’s disease. Only -1- 5 specialists should initiate treatment, and patients should be reviewed at least every six months. Sam Crowe MFP Specialist Trainee in Public Health Bournemouth and Poole PCT 2 BOURNEMOUTH AND POOLE PRIMARY CARE TRUST 3. INTRODUCTION 3.1 The Primary Care Trust has a decision making process for whether NICE technology appraisal is relevant to the organisation. The information about relevance of guidance is entered onto the Primary Care Trust database and a summary is produced on CD for practices and relevant Trust staff. 3.2 At present, Members of the Clinical Governance Committee have responsibility for implementation, in their area as outlined in the NICE Implementation Policy. This requires Action Plans for implementation, and horizon scanning to be in place for all relevant guidance. Arrangements are in place to review and monitor implementation action plans when NICE guidance is applicable to services provided directly by the Trust. 3.3 NSF Local Implementation Teams have been set up and ensure that national guidance is followed as appropriate in the specific disease areas. Independent Contractors 3.4 HSC (2003/011) requires Clinicians to inform the Primary Care Trust Clinical Governance Committee if they intend to introduce new interventional procedures, which he/she has not used before, or has only used outside the NHS. All GPs have been notified of their obligations under HSC 2003/011. 3.5 Practices are asked to complete a questionnaire to notify the Trust of their compliance levels. This data is entered onto the Primary Care Trust database and monitored. 3.6 GMS/GDS Contracts and all new SLAs have incorporated a statement of compliance with national guidance including NICE. Commissioned Service 3.7 All new contracts have compliance with NICE guidance written into them. 3.8 NICE implementation database is under constant review at the Poole Hospital NHS Trust Clinical Governance Committee and Clinical Audit and Effectiveness Group monitor the implementation of NICE guidance. The quality monitoring group reviews the compliance of RBCH with all new interventional procedures. There is cross representation on all these groups. Giselle Thornton Clinical Governance Manager 06 May 2017 3