Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
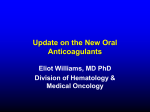
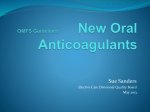
Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review Non-vitamin K antagonist oral anticoagulants (NOACs): clinical evidence and therapeutic considerations Karan Saraf,1 Paul Morris,1,2 Pankaj Garg,1 Paul Sheridan,1,2 Robert Storey1,2 1 Department of Cardiology, Sheffield Teaching Hospitals NHS Foundation Trust, Northern General Hospital, Sheffield, UK 2 Department of Cardiovascular Science, University of Sheffield, Medical School, Sheffield, UK Correspondence to Dr Karan Saraf, Department of Cardiology, Sheffield Teaching Hospitals NHS Foundation Trust, Northern General Hospital, Herries Road, Sheffield S5 7AU, UK; [email protected] Received 1 February 2014 Revised 16 July 2014 Accepted 18 July 2014 Published Online First 1 August 2014 ABSTRACT Warfarin, a vitamin K antagonist, is the most widely used oral anticoagulant in the world. It is cheap and effective, but its use is limited in many patients by unpredictable levels of anticoagulation, which increases the risk of thromboembolic or haemorrhagic complications. It also requires regular blood monitoring and dose adjustment. New classes of drugs, non-vitamin K antagonist oral anticoagulants (NOACs), are now supported as alternatives to warfarin. Three NOACs are licensed: dabigatran, a direct thrombin inhibitor, and rivaroxaban and apixaban, antagonists of factor Xa. NOACs do not require routine blood monitoring or dose adjustment. They have a rapid onset and offset of action and fewer food and drug interactions. Current indications include treatment and prophylaxis of venous thromboembolism and prevention of cardioembolic disease in non-valvular atrial fibrillation. Effective antidotes are lacking and some caution must be used in severe renal impairment, but favourable trial evidence has led to their widespread adoption. Research is ongoing, and an increase in their use and indications is expected in the coming years. INTRODUCTION ▸ http://dx.doi.org/10.1136/ postgradmedj-2013-132474 ▸ http://dx.doi.org/10.1136/ postgradmedj-2014-132950 To cite: Saraf K, Morris P, Garg P, et al. Postgrad Med J 2014;90:520–528. 520 Warfarin remains the most widely used vitamin K antagonist (VKA) for the prevention and treatment of thromboembolic disease. For decades it has remained the gold standard anticoagulant in the treatment of deep venous thrombosis (DVT) and pulmonary embolism (PE), and for the prevention of cardiac thromboembolic disease such as stroke in patients with atrial fibrillation (AF). However, its use is complicated by a variety of food and drug interactions and its narrow therapeutic range and variable patient dose-response require regular laboratory monitoring and careful dose titration. Even with frequent, meticulous monitoring, it can still be difficult to achieve stable anticoagulation in many patients.1 According to the international normalised ratio (INR) monitoring, control in the UK is among the best in the world, with an average time in therapeutic range of approximately 65%.2–4 In the remaining 35%, two-thirds of INRs are below the therapeutic window, predisposing to thromboembolism, and a third are above the therapeutic window, increasing the risk of bleeding.1 Therefore, warfarin is both inconvenient and exposes patients to periods of undertreatment and overtreatment with the subsequent risk of complications. Additionally, regular monitoring of warfarin treatment consumes significant health resources. Over the last decade, several alternative oral anticoagulants have been developed that have a direct and reversible inhibitory effect on either thrombin or factor Xa. A plethora of clinical trials have demonstrated the efficacy and safety of these newer generation anticoagulants. Until recently, they were designated ‘novel oral anticoagulants’, with the abbreviation non-vitamin K antagonist oral anticoagulants (NOACs). However, the European Society of Cardiology Working Group on Thrombosis task force on anticoagulants in heart disease recommends that ‘NOACs’ should denote ‘Non-vitamin K antagonist Oral AntiCoagulants’, when referring to these direct inhibitors of single coagulation factors.5 NOACs are effective alternatives to VKAs for the treatment and prevention of thromboembolic disease. These agents do not require monitoring or dose adjustment and thus represent a more convenient option for both patients and physicians. The UK National Institute of Health and Care Excellence (NICE) has undertaken several technology appraisals that have resulted in three NOACS being recommended as an alternative to VKAs and even first-line oral anticoagulants. It is, therefore, important for physicians to be familiar with the mechanisms of action, efficacy and safety data, cost-effectiveness and current NICE recommendations for the available NOACs. This article examines each of these topics and presents some practical considerations in the use of NOAC drugs as an alternative to warfarin.5 MECHANISMS OF ACTION The mechanisms of action of NOACs differ from that of the VKAs (figure 1), and understanding these differences aids decision making when choosing an anticoagulant for individual patients. Vitamin K antagonists In order to contribute effectively to the coagulation cascade, factors II ( prothrombin), VII, IX and X must first be carboxylated, allowing their binding to the surface of activated platelets and vascular endothelium. This process is dependent upon the enzymatic recycling of vitamin K. By inhibiting this with a VKA, newly synthesised clotting factors are rendered biologically inactive. As the circulating active clotting factors degrade over hours and days, normal coagulation is inhibited and anticoagulation achieved.6 This explains the long VKA half-life (approximately 40 h for warfarin). There is significant heterogeneity in the rate of VKA metabolism (mainly due to genetic variations), which results in Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review Figure 1 Mechanism of action of vitamin K antagonists and non-vitamin K antagonist oral anticoagulants (adapted from Steffel and Braunwald.32 Reproduced with kind permission from Oxford University Press). a variable and unpredictable period until a stable INR is achieved and maintained thereafter.1 VKAs include warfarin, acenocoumarol and dicoumarol. However, in the context of the current article, only warfarin is considered because it is, by far, the most commonly used VKA and is the drug upon which all relevant clinical evidence is based. Non-vitamin K antagonist oral anticoagulants There are currently two main types of NOACs: direct thrombin inhibitors (ie, dabigatran) and factor Xa inhibitors (ie, rivaroxaban, apixaban). Unlike warfarin, NOACs inhibit a single coagulation factor, have short half-lives and do not require either monitoring or dose titration. Dabigatran etexilate (Pradaxa) acts via direct inhibition of thrombin (factor II), leading to potent anticoagulation.7 Thrombin performs several crucial roles in the coagulation cascade. It promotes platelet activation, which in turn facilitates further thrombin generation, and activates multiple factors in the final step of coagulation, including the cleavage of fibrinogen to fibrin, thus having the dominant role in the stabilisation of a clot. Rivaroxaban (Xarelto) and apixaban (Eliquis) are direct inhibitors of factor Xa. In doing so, they disrupt both the intrinsic and the extrinsic coagulation pathways, preventing the formation of thrombin and subsequent clotting.8 Because NOAC effect is determined solely by plasma concentration rather than by inhibition of clotting factor synthesis, they have a rapid onset of action once absorbed into the circulation. The half-life of dabigatran is approximately 12–17 h, rivaroxaban 7–11 h and apixaban 9–14 h. Cessation of administration results in a relatively rapid return to baseline physiology.8 Unlike warfarin, all three NOACs are associated with a consistent and predictable dose-response and time taken to reach steady state. Haematological monitoring and dose adjustment are therefore unnecessary.9 EVIDENCE FOR EFFICACY AND SAFETY OF NOACs In terms of evidence base, warfarin is the current gold standard in the treatment of venous thromboembolism (VTE) and in the prevention of stroke and systemic embolism in patients with AF, reducing stroke rate by two-thirds.2 New anticoagulants must not only have practical advantages (eg, lack of need for monitoring), but must demonstrate at least equal efficacy and safety profiles before they can be considered as alternatives. The following sections review some of the landmark randomised controlled trials that have compared NOACs with warfarin, focusing on the primary efficacy (deleterious events avoided by treatment) and safety (adverse events as a result of treatment) end points in comparison with standard treatment with warfarin. PREVENTION OF STROKE AND SYSTEMIC EMBOLISM IN PATIENTS WITH NON-VALVULAR AF Up to 20% of acute strokes occur as a consequence of AF with cardiac thromboembolism.2 Once identified, those at increased risk should be established on lifelong anticoagulation in order to reduce the risk of this debilitating complication. Trials evaluating NOACs in patients with AF have looked at a primary efficacy end point of reduction in stroke or systemic embolism and primary safety end points of mortality and bleeding, particularly intracranial haemorrhage. RE-LY7 is the largest prospective, multicentre randomised controlled trial comparing dabigatran, at two doses of 110 or 150 mg twice-daily, with standard warfarin therapy. In total, 18 113 patients with AF and at least two risk factors for stroke were enrolled and followed up for 2 years. The lower dose of dabigatran was comparable in efficacy with warfarin (1.53% events per year vs 1.69%, p<0.001). The higher dose was superior (1.11% events per year vs 1.69%, p<0.001) to the lower dose. Major bleeding was reduced in those receiving dabigatran 110 mg (2.71% per year vs 3.36%, p<0.001) and was similar to warfarin in the higher dose group (3.11%, p=0.31). Compared with warfarin, haemorrhagic stroke was also reduced in both the low-dose and high-dose groups (0.12% and 0.1% vs 0.38%, respectively, p<0.001 for both comparisons). There were higher rates of dyspepsia in both dabigatran groups (11.8% in the 110 mg and 11.3% in the 150 mg dabigatran groups vs 5.8% in the warfarin group, p<0.001 for both comparisons). This study was extended for a further 2 years (RELY-ABLE10) in order to gain more data to compare the two doses of dabigatran, and followed up 48% of the original dabigatran-treated groups. Stroke or systemic embolism Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 521 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review occurred in 1.46% (150 mg) and 1.6% per year (110 mg), with major bleeding in 3.74% and 2.99% per year, respectively, confirming that, compared with the lower dose of dabigatran, the higher dose was more efficacious, but resulted in more bleeding. Similar in design to RE-LY, ROCKET-AF11 is the largest trial comparing rivaroxaban 20 mg once-daily with warfarin. In total, 14 264 patients with AF were enrolled, 10% of whom had at least two risk factors, and 90% of whom had at least three risk factors for stroke. Rivaroxaban was comparable with warfarin in preventing stroke or systemic embolism (1.7% vs 2.2% per year, p<0.001). While there were no significant differences in the rates of major and non-major bleeding, there were fewer intracranial (0.5% vs 0.7%, p=0.02) and fatal haemorrhages (0.2% vs 0.5%, p=0.003) with rivaroxaban. ARISTOTLE,8 the last of these three landmark trials, compared warfarin with apixaban 5 mg twice-daily in 18 201 patients with AF and at least one risk factor for stroke. Stroke or systemic embolism was reduced in the apixaban group (1.27% vs 1.6% per year), showing superiority ( p<0.01) over warfarin therapy. Furthermore, there were fewer major bleeding events (2.13% vs 3.09%, p<0.001) and haemorrhagic strokes (0.24% vs 0.47%, p<0.001) in the apixaban group. Apixaban was also better tolerated than warfarin, with fewer drug discontinuations. In contrast to the other studies, all-cause mortality was significantly reduced in the apixaban group (3.52% vs 3.94%, p=0.047). Apixaban was, therefore, superior to warfarin in preventing stroke, embolic events, bleeding of any kind and death. In summary, in these trials, NOACs were either comparable with (dabigatran 110 mg and rivaroxaban) or superior (dabigatran 150 mg and apixaban) to warfarin in preventing stroke or systemic embolism and demonstrated either a similar (dabigatran 150 mg and rivaroxaban) or superior (dabigatran 110 mg and apixaban) safety profile, with reductions in major and minor bleeding rates. A significant concern with using any anticoagulant is the risk of intracranial haemorrhage because even a modest bleed can result in significant and permanent morbidity or even death. However, all three agents were associated with a statistically significant reduction in the rates of intracranial haemorrhage compared with warfarin. VENOUS THROMBOEMBOLISM Prospective trials evaluating the treatment of VTE or VTE prophylaxis following high-risk procedures such as orthopaedic surgery have demonstrated similarly positive results in favour of NOACs. Treatment of VTE Suboptimal INR control in patients with DVT or PE is associated with recurrent thrombosis and increased morbidity and mortality, all of which places a significant burden upon limited healthcare resources. In VTE (acute DVT or PE) treatment, NOACs were compared with standard care, that is, acute subcutaneous low-molecular-weight heparin (enoxaparin) followed by warfarin. Enoxaparin was discontinued when the patient was established on warfarin with a therapeutic and stable INR; treatment in both groups continued for a standardised period. The primary end points were recurrent DVT or PE within the treatment period. The RE-COVER II trial found dabigatran 150 mg twice-daily to be comparable with standard treatment ( p<0001), with similar major bleeding event rates and lower overall bleeding rates.12 Rivaroxaban was evaluated in two studies. In EINSTEIN-DVT,13 rivaroxaban (15 mg twice-daily for 3 weeks, then 20 mg once-daily) was comparable with standard treatment for acute DVT (2.1% vs 3%, p<0.001) with a 522 similar safety profile. The EINSTEIN-PE trial14 involved a similar comparison, this time for the treatment of acute PE. Rivaroxaban was again comparable with standard therapy in preventing the primary end point. Major or clinically relevant non-major bleeding rates were similar between the two groups, but there were significantly fewer major bleeds in the rivaroxaban group. The AMPLIFY trial15 showed that apixaban (10 mg twice-daily for 1 week, then 5 mg twice-daily) demonstrated comparable efficacy to standard therapy in treatment of acute DVT and PE. Apixaban had a superior safety profile with major bleeding occurring in 0.6% of patients compared with 1.8% in the conventional treatment group ( p<0.001). Prophylaxis of VTE following orthopaedic surgery Many orthopaedic operations, particularly procedures involving the hip and lower limb, increase the risk of thromboembolism in the postoperative period. Appropriate patients, therefore, receive a once-daily administration of low-molecular-weight heparin (enoxaparin) for a standardised period determined by the nature of the procedure. In the RE-MODEL trial,16 dabigatran 150 or 220 mg once-daily was found to be comparable with enoxaparin with a similar safety profile. The RECORD trials17 18 compared rivaroxaban 10 mg once-daily with enoxaparin and demonstrated superiority of rivaroxaban with similar rates of bleeding. In ADVANCE-2, apixaban 2.5 mg twice-daily was superior in preventing VTE, with similar bleeding rates.19 Although not exhaustive, this review includes the most significant ‘landmark’ trials that are representative of the trial evidence to date in these areas. Similarly positive results have been demonstrated for dabigatran, rivaroxaban and apixaban in almost all other large-scale trials not highlighted by our review.20–24 LICENSING AND COST-EFFECTIVENESS Since February 2013, all three NOACs have been licensed by NICE for the following indications: ▸ The prevention of VTE in adults undergoing elective total hip or knee replacement surgery. ▸ The prevention of stroke or systemic embolism in adults with non-valvular AF and one or more of the following risk factors: previous stroke, transient ischaemic attack or systemic embolism; left ventricular ejection fraction <40%; symptomatic heart failure≥New York Heart Association class 2; age ≥75 years; age ≥65 years associated with one of the following: diabetes mellitus, coronary artery disease or hypertension. In addition, rivaroxaban is licensed for both the treatment of acute DVT and chronic prophylaxis of recurrent DVT and/or PE in adults following an initial diagnosis of DVT. Full technology appraisals for the three NOACs undertaken by NICE25–28 resulted in their recommendation as first-line agents for the indications listed above, on the basis that they provide a superior or at least equal efficacy and safety profile to warfarin, while providing a more convenient treatment regimen with fewer limitations (monitoring, dose adjustment, interactions). NOACs are significantly more expensive than warfarin. However, several economic evaluations have deemed their use as first-line agents to be cost-effective in the long term, given that patients treated with NOACs require fewer healthcare resources, due to a reduction in adverse events (bleeding, stroke and VTE) and the lack of need for monitoring and dose adjustment compared with warfarin.29–32 However, few of these reports are based on prospective trial data with most being Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review generated by decision analysis models and further work is required to provide a definitive answer. Importantly, NICE concludes that NOACs are indeed cost-effective alternatives to warfarin and that cost should not be a barrier to the initiation of, or conversion to, an NOAC.25–28 POTENTIAL COMPLICATIONS WITH NOACs There are a number of considerations before prescribing an NOAC. Side effects In addition to the risk of bleeding (common with all anticoagulants), NOACs are uncommonly associated with nausea, vomiting, diarrhoea and dizziness. There is stronger association between dabigatran and dyspepsia (approximately 11%) and, although not an absolute contraindication, it should be used with caution in those with gastroesophageal reflux disease.7 33 Chronic kidney disease Warfarin does not require dose modification in renal impairment. However, all NOACs are at least partially renally excreted (dabigatran 80%, rivaroxaban 35%, apixaban 27%). Considerable trial data support their use in mild-to-moderate chronic kidney disease (CKD), with dose reduction in some cases (table 1). Limited data are available regarding use in patients with advanced CKD or severe acute kidney injury. Consequently, NOACs are not licensed for use in severe renal impairment and should be discontinued if significant acute kidney injury develops while on the medication. Dabigatran is contraindicated in patients with a creatinine clearance <30 mL/ min. Rivaroxaban is also contraindicated, for the specific indication of VTE, if creatinine clearance is <30 mL/min but can be used for AF with dose reduction. Apixaban is considered the safest drug for use in patients with renal impairment because it has the lowest dependency upon renal excretion. It can be continued until creatinine clearance declines to 15 mL/min.9 NOAC trials are yet to generate long-term follow-up data, but many patients require lifelong anticoagulation. Renal impairment may develop or deteriorate over time, resulting in drug accumulation and increased risk of haemorrhage. Monitoring of renal function should be undertaken in patients receiving these drugs to ensure their safety profile remains at least equivalent to warfarin over time (yearly in most patients; 6 monthly in CKD3; 3 monthly in CKD4).9 Drug interactions NOACs are associated with far fewer drug interactions than warfarin and have no known interactions with foods. The combination of NOAC therapy with certain antiepileptic, antifungal, macrolide antibiotic and antiarrhythmic drugs can result in increased NOAC plasma levels that necessitates either dose modification or contraindicates their use (see table 1). A detailed list of contraindications is included in the European Heart Rhythm Association practical guide to NOACs.9 Emergency management of bleeding or overdose The principles of managing major bleeding in patients receiving warfarin therapy are well established. When required, VKA-associated anticoagulation can be readily reversed with vitamin K and/or prothrombin complex concentrate. Currently, there are no antidotes for NOAC-induced anticoagulation and only little experience in the management of overdose or haemorrhage when urgently reversing the anticoagulant effect becomes necessary. However, NOACs have comparatively short half-lives, and a combination of local measures, such as compression, and cessation of drug administration are often Table 1 NOAC dosing recommendations and considerations9 Licensed dose Stroke prevention in AF VTE prophylaxis VTE treatment Kidney disease CrCl >50 mL/min CrCl 30–49 mL/min CrCl 15–29 mL/min CrCl <15 mL/min Caution Dabigatran Rivaroxaban Apixaban 150 mg BD 220 mg OD N/A 20 mg OD 10 mg OD 15 mg BD 21 days, then 20 mg OD 5 mg BD 2.5 mg BD N/A No dose modification Consider 110 mg BD (AF) Consider 150 mg OD (VTE) Not recommended No dose modification 15 mg OD (AF) No modification (VTE) 15 mg OD (AF) Not recommended (VTE) Not recommended No dose modification No dose modification Age >80 Weight <60 kg Macrolide antibiotics Amiodarone Age >80 Weight <60 kg Macrolide antibiotics Carbamazepine Phenytoin Age >80 Weight <60 kg Diltiazem Ketoconazole Itraconazole Carbamazepine Phenytoin Dronedarone Ketoconazole Itraconazole Ketoconazole Itraconazole Carbamazepine Phenytoin Not recommended 2.5 mg BD Not recommended Contraindicated AF, atrial fibrillation; BD, twice-daily regimen; CrCl, creatinine clearance as calculated by Cockcroft–Gault formula; NOAC, non-vitamin K antagonist oral anticoagulant; OD, once-daily regimen; VTE, venous thromboembolism. Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 523 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review Figure 2 European Society of Cardiology guidelines on management of bleeding in patients taking non-vitamin K antagonist oral anticoagulant (adapted from Heidbuchel et al.9 Reproduced with kind permission from Oxford University Press). aPCC, activated prothrombin complex concentrate; NOAC, non-vitamin K antagonist oral anticoagulant; PCC, prothrombin complex concentrate; RBC, red blood corpuscles; rFVIIa, recombinant activated factor VII. sufficient to reverse the anticoagulant effect in the context of non-life-threatening bleeding, with normal coagulation being achieved within 24 h. This is a slightly longer time course when compared with the administration of vitamin K for a patient anticoagulated with warfarin (approximately 12 h). Evidence supporting anticoagulation reversal with these agents in major life-threatening bleeding is limited to controlled trials conducted in healthy human subjects largely yielding mixed results.34 Dabigatran elimination may be achieved via haemofiltration or charcoal haemoperfusion. The effects of the factor Xa inhibitors (rivaroxaban and apixaban) may be, at least partially, reversed with the co-administration of prothrombin complex concentrate (25–50 UI/kg) and recombinant factor VIIa (90 μg/kg). These measures need further evaluation, particularly in the setting of major bleeding (figure 2). At least one specific antidote to factor Table 2 Effect of NOACs on coagulation tests (adapted from Gavillet and Angelillo–Scherrer.35 Reprinted with kind permission from EMH Swiss Medical Publishers Ltd.) PT APTT INR D-Dimer Fibrinogen Anti-Xa Antithrombin Dabigatran Rivaroxaban Apixaban Decreased Increased Increased Same Same Same Increased Decreased Increased Increased Same Same Increased Same Decreased Increased Increased Same Same Increased Same INR, international normalised ratio; NOAC, non-vitamin K antagonist oral anticoagulant. 524 Xa inhibitors has been shown to be effective in early animal models, and more sophisticated agents are in development, but further evidence is required before these can be made available for clinical use.35 36 Hospitals should issue local protocols for the management of bleeding associated with NOAC treatment. While routine monitoring is not required, there are situations where quantitative evaluation of anticoagulant effect may be desirable, for example, preoperatively. This is possible with new assays for antithrombin and antifactor Xa. Widespread availability of these tests remains limited at the current time. A further consideration is the effect these drugs have on standard laboratory coagulations assays that are outlined in table 2.35 CURRENT RESEARCH AND THE FUTURE Evidence now supports NOAC use for treatment and prevention of VTE in certain patients with non-valvular AF and in those undergoing elective hip or total knee replacement. Current research is focused on identifying other potential roles in conditions such as the acute coronary syndromes (ACSs), AF with associated valvular heart disease and in those who require anticoagulation because of a mechanical prosthetic heart valve. It is likely that the range of indications for NOAC use will widen over time. Acute coronary syndromes Trials evaluating the efficacy of NOACs in ACSs when added to standard therapy have produced mixed results. In the placebocontrolled ATLAS ACS 2-TIMI 51 study, low-dose rivaroxaban (2.5 or 5 mg twice-daily) was associated with a reduction in stroke and cardiovascular mortality when added to standard medical therapy ( p=0.008), but increased the rate of major bleeding ( p<0.001).37 The APPRAISE-2 trial for apixaban was aborted prematurely due to a significant increase in major Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review Table 3 NOAC overview1 9 Mechanism of action Half-life Renal excretion Renal failure (table 1) Clinical trials AF VTE prophylaxis VTE treatment Outcomes (vs gold standard)* Efficacy in AF Efficacy in VTE prophylaxis Efficacy in VTE treatment Bleeding in AF Bleeding in VTE Licence date (NICE) Stroke prevention in AF VTE Indications (NICE) Stroke prevention in AF VTE prophylaxis (preoperative/postoperative) VTE treatment (DVT/PE) Drug cost/month (warfarin=£1) Dabigatran Rivaroxaban Apixaban Direct thrombin inhibitor 12–17 h 80% Caution Direct factor Xa inhibitor 7–11 h 35% Caution Direct factor Xa inhibitor 9–14 h 27% Best Re-LY RE-MODEL RE-COVER RE-COVER II ROCKET-AF RECORD I-IV EINSTEIN-DVT EINSTEIN-PE ARISTOTLE ADVANCE I-III AMPLIFY Better (150 mg) Equal (110 mg) Equal Equal Better Equal Equal Better Better Equal Equal Equal Better Better Better Better 15 March 2012 24 September 2008 21 May 2012 22 April 2009 27 February 2013 25 January 2012 ✓ ✓ × 110 mg BD=£65.90 150 mg BD=£65.90 ✓ ✓ ✓ 10 mg OD=£63 15 mg OD=£58.80 15 mg BD (21 days)=£88.20 20 mg OD=£58.80 ✓ ✓ × 2.5 mg BD=£65.90 5 mg BD=£61.50 *Gold standard = warfarin (stroke prevention in AF), enoxaparin (VTE prophylaxis) or both (VTE treatment). AF, atrial fibrillation; DVT, deep venous thrombosis; NICE, National Institute of Health and Care Excellence; NOAC, non-vitamin K antagonist oral anticoagulant; PE, pulmonary embolism; VTE, venous thromboembolism; BD, twice-daily regimen; OD, once-daily regimen. bleeding events without a decrease in ACS events.38 Phase III trial development for dabigatran in ACS has also ceased because of safety concerns. The future role of NOACs in ACS therefore remains uncertain, and further research is underway. NICE guidance on the prevention of adverse outcomes in the management of ACS is expected in March 2015, including recommendations for the role of NOACs (table 3). Valvular heart disease Although the original ARISTOTLE trial8 excluded patients with significant mitral stenosis or valve prosthesis, those with mitral regurgitation, less significant mitral stenosis, aortic stenosis, aortic regurgitation, tricuspid regurgitation or previous valve surgery were included. In a post hoc subanalysis, the results in these patients were consistent with the positive overall results, that is, apixaban was associated with a similar reduction in stroke, major bleeding events and all-cause mortality in those with or without valve disease (excluding significant mitral stenosis and/or prosthetic valve).39 Given that patients with valve disease and AF are known to suffer worse outcomes with respect to thromboembolism than those without, it is, therefore, likely that this group will also gain a recommendation for NOAC therapy in the near future. The role for NOACs in those with prosthetic valves also requires further evaluation. Prosthetic valve patients anticoagulated with dabigatran were shown to be at increased risk of valve thrombosis and haemorrhage compared with warfarin in the RE-ALIGN trial.40 It is hoped that the role of NOACs in this group will be further clarified by the DAWA study, which is currently assessing the efficacy and safety of dabigatran in patients with prosthetic heart valves.41 Other NOACs The desire for effective, convenient and safe anticoagulants and the large potential market size has driven research in this area, which is now very active and dynamic. Other NOACs are being developed and assessed. Edoxaban, another factor Xa inhibitor, has been tested in stroke prevention for AF and for VTE prophylaxis with favourable outcomes, and indeed has already been licensed for VTE prophylaxis in orthopaedic surgery in Japan.42 43 In addition, a host of novel inhibitors, targeted at factors IX and XII, are under development and it is almost certain that the number of NOACs and their indications will increase over the coming years.44 CONCLUSION In appropriate patients, NOACs offer safe, efficacious and predictable anticoagulation. Efficacy and safety are at least equivalent to warfarin and in certain groups appear superior. Because NOACs do not require monitoring or dose titration to achieve optimal anticoagulation, and have fewer food and drug interactions, shorter half-lives and simpler dosing regimens, they are far more convenient for doctors and patients compared with warfarin. NOACs are redefining how we approach VTE prophylaxis and treatment. In line with NICE guidance, many centres have already adopted NOACs as first-line anticoagulants. In Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 525 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review patients who are well established on warfarin, with stable INRs in the therapeutic range, there may be little or no additional clinical benefit from changing to NOAC therapy. Patients in whom over-anticoagulation or under-anticoagulation is particularly risky or those with labile INRs, poor drug compliance or difficulty attending for INR monitoring may benefit from conversion from warfarin to NOAC therapy. Antidotes for NOACs are still not available and there remain concerns about use in those with severe renal impairment. Therefore, NOACs are not a ‘one size fits all’ solution, and patients should be carefully selected in order to maximise benefit while minimising the risk of adverse events. These decisions should be aided by the use of risk analysis tools such as the CHA2DS2VASc and HASBLED scores, which can be used to balance potential benefit versus risk.25–28 Uptake and adoption of NOACs is accelerating. They are quickly becoming the first-choice anticoagulant for many patients and for many doctors. It is important that clinicians are familiar with the presented topics to enable appropriate anticoagulant prescribing. Furthermore, physicians should be aware that the literature concerning this class of drugs is expanding, as are the indications for NOAC use. Main messages ▸ Warfarin, the most commonly used anticoagulant, is limited by multiple food and drug interactions, the necessity for regular monitoring and dose adjustment and an often unpredictable anticoagulant effect. ▸ Non-vitamin K antagonist oral anticoagulants (NOACs) (dabigatran, rivaroxaban and apixaban) have fewer interactions, require no monitoring, have simple dosing regimens and predictable anticoagulation and are more convenient to use than warfarin. ▸ NOACs are at least as effective as warfarin at preventing thromboembolic events and have fewer associated bleeding events. ▸ There is no antidote for these NOACs. In non-life-threatening bleeding, local measures and cessation of drug is enough to achieve haemostasis. Hospitals should have their own protocols for management of life-threatening bleeding. ▸ Choice of anticoagulant must be tailored to the individual patient—NOACs are particularly useful in those with poor compliance with healthcare appointments, labile international normalised ratios and those in whom bleeding is of greater concern. Management of patients on NOACs4 When to choose an NOAC over warfarin: Clinicians are at present more comfortable with prescribing warfarin, but NOACs need not just be considered as second-line agents. They may be initiated as first-line anticoagulation. However, certain patient groups that may benefit from NOAC therapy over warfarin include those who may not be presented with regular international normalised ratio (INR) checks, those with cognitive impairment who may not be able to remember variable dosing with warfarin, those already on warfarin who have labile INRs and those whose stroke and bleeding risks may be similar (as calculated using the CHA2DS2VASc and HASBLED scores), therefore requiring agents that are associated with fewer bleeds to increase benefit over risk. Cautions for starting NOAC therapy: at least moderate chronic kidney disease (CKD) and specific drug–drug interactions (table 1). What to check at follow-up appointments: Compliance, thromboembolic or bleeding events, side effects, other medications that may interact with NOAC (table 1), and blood testing (FBC, LFT, U&E): 1 yearly (CKD1–2); 6 monthly (CKD3) or 3 monthly (CKD4). To switch from warfarin to NOAC (eg, labile INR, drug interactions): Stop warfarin and check INR. Start apixaban/dabigatran when INR <2, rivaroxaban when INR <3. To switch from NOAC to warfarin (eg, new or worsening renal function): Administer NOAC and warfarin concomitantly until INR >2. Ensure INR checks done prior to NOAC dose, and 24 h post monotherapy with warfarin. Advice to patient if missed a dose: Take missed dose up to 6 h (in twice daily regimen) or 12 h (in once daily regimen) after scheduled dose. Otherwise, continue from next scheduled dose. No double doses. 526 Current research questions ▸ Are NOACs suitable for the primary/secondary prevention of acute coronary syndrome? ▸ Do patients with atrial fibrillation (AF) and valve disease derive similar benefit from NOAC therapy as those with non-valvular AF? ▸ Are NOACs a safe replacement for warfarin in patients who require anticoagulation prior to cardioversion for AF? Data are only available for dabigatran currently, which has shown equal efficacy to warfarin. ▸ Can a safe NOAC antidote be developed for use in NOAC-associated haemorrhage? ▸ Are NOACs efficacious and safe for use in patients who require a greater level of anticoagulation, for example, those with prosthetic heart valves? Key references ▸ Heidbuchel H, Verhamme P, Alings M, et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace 2013;15:625–51. ▸ Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–51. ▸ Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981–2. ▸ Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883–91. Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review REFERENCES Self assessment questions 1 1. Which statements are true regarding the safe use of an NOAC with the respective renal function (as expressed as creatinine clearance)? A. Dabigatran at normal dose in a patient with AF and creatinine clearance 51 mL/min B. Dabigatran at reduced dose in a patient with AF and creatinine clearance 28 mL/min C. Rivaroxaban at normal dose in a patient with acute DVT and creatinine clearance 31 mL/min D. Apixaban at reduced dose in a patient with AF and creatinine clearance 15 mL/min 2. The following drugs are safe to prescribe (but must be monitored closely) in patients taking phenytoin or carbamazepine: A. Dabigatran B. Warfarin C. Rivaroxaban D. Apixaban 3. The following drugs are currently licensed for use in anticoagulation of patients with AF who are awaiting direct-current cardioversion: A. Rivaroxaban B. Warfarin C. Apixaban D. Warfarin 4. The following are recommended methods for reversal of anticoagulation in the context of major bleeding: A. Intravenous vitamin K in a patient anticoagulated with warfarin B. Intravenous prothrombin complex concentrate in a patient anticoagulated with a NOAC C. Intravenous prothrombin complex concentrate and recombinant factor VIIa in a patient anticoagulated with a NOAC D. Intravenous vitamin K and prothrombin complex concentrate in a patient anticoagulated with warfarin 5. The following statement are true regarding efficacy and safety of NOACs when compared with warfarin: A. Apixaban has largely been shown to be superior in both efficacy and safety when compared with warfarin for the prevention of stroke and systemic embolism in patients with AF B. Rivaroxaban has been shown to be superior to warfarin in efficacy, and comparable in safety for the prevention of stroke and systemic embolism in patients with AF C. Rivaroxaban was equal in both efficacy and safety when compared with warfarin in the treatment of acute DVT or PE D. Dabigatran high dose (150 mg twice daily) was superior to warfarin in both efficacy and safety for prevention of stroke or systemic embolism in patients with AF 2 Contributors All authors conducted a literature review, formulated the first draft and were all involved in subsequent revisions and alterations to the manuscript. Competing interests RS declares receiving institutional grants from AstraZeneca, Eli Lilly/Daiichi Sankyo, and Merck; research support from Accumetrics; honoraria from AstraZeneca, Eli Lilly/Daiichi Sankyo, Merck, Novartis, Iroko, Sanofi-Aventis, Bristol Myers Squibb, Accumetrics and Medscape; and consultancy fees from AstraZeneca, Merck, Novartis, Accumetrics, PlaqueTec and Roche. Provenance and peer review Not commissioned; externally peer reviewed. 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the seventh ACCP conference on anti- thrombotic and thrombolytic therapy. Chest 2005;127:415–16. Connolly SJ, Pogue J, Eikelboom J, et al. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation 2008;118:2029–37. Mitka M. FDA advisory decision highlights some problems inherent in pragmatic trials. JAMA 2011;306:1851–2. Rose AJ, Ozonoff A, Henault LE, et al. Warfarin for atrial fibrillation in community-based practise. J Thromb Haemost 2008;6:1647–54. Husted S, de Caterina R, Andreotti F, et al. Non-vitamin K antagonist oral anticoagulants (NOACs): no longer new or novel. Thromb Haemost 2014;111:781–2. Whitlon DS, Sadowski JA, Suttie JW. Mechanism of coumarin action: significance of vitamin K epoxide reductase inhibition. Biochemistry 1978;17:1371–7. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–51. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981–2. Heidbuchel H, Verhamme P, Alings M, et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace 2013;15:625–51. Connolly SJ, Wallentin L, Ezekowitz MD, et al. The long term multicentre observational study of dabigatran treatment in patients with atrial fibrillation (RELY-ABLE) study. Circulation 2014;128:237–43. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883–91. Schulman S, Kakkar AK, Schellong SM, et al. A randomized trial of dabigatran versus warfarin in the treatment of acute venous thromboembolism (RE-COVER II). American Society of Hematology 2011 Annual Meeting; 12 December, 2011; San Diego, CA. Abstract 205. Bauersachs R, Berkowitz SD, Brenner B, et al.; EINSTEIN Investigators. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010;363:2499–510. Buller HR, Prins MH, Lensin AW, et al.; EINSTEIN-PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012;366: 1287–97. Agnelli G, Buller HR, Cohen A, et al. Apixaban for the treatment of acute venous thromboembolism. N Engl J Med 2013;369:799–808. Eriksson BI, Dahl OE, Rosencher N, et al. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trial. J Thromb Haemost 2007;5:2178–85. Lassen MR, Ageno W, Borris LC, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty. N Engl J Med 2008;358:2776–86. Eriksson BI, Borris LC, Friedman RJ, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med 2008;358:2765–75. Lassen MR, Raskob GE, Gallus A, et al. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): a randomised double blind trial. Lancet 2010;375:807–15. Conolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patients with atrial fibrillation. N Engl J Med 2011;364:806–17. Lassen MR, Gallus A, Raskob JE, et al. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med 2010;363:2487–98. Eriksson BI, Dahl OE, Rosencher N, et al. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double-blind, non-inferiority trial. Lancet 2007;370:949–65. Cohen AT, Spiro TE, Buller HR, et al. Rivaroxaban for thromboprophylaxis in acute ill medical patients. N Engl J Med 2013;368:513–28. Romualdi E, Donadini MP, Ageno W. Oral rivaroxaban after symptomatic venous thromboembolism: the continued treatment study (EINSTEIN extension study). Expert Rev Cardiovasc Ther 2011;9:841–4. http://guidance.nice.org.uk/TA249 (accessed 23 May 2014). http://guidance.nice.org.uk/TA256 (accessed 23 May 2014). http://guidance.nice.org.uk/TA261 (accessed 23 May 2014). http://guidance.nice.org.uk/TA275 (accessed 23 May 2014). Kansal AR, Sorensen SV, Gani R, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in UK patients with atrial fibrillation. Heart 2012;98:573–8. Harrington AR, Armstrong EP, Nolan PE, et al. Cost-effectiveness of apixaban, dabigatran, rivaroxaban and warfarin for stroke prevention in atrial fibrillation. Stroke 2013;44:1676–81. Lee S, Anglade MW, Pham D, et al. Cost-effectiveness of rivaroxaban compared to warfarin for stroke prevention in atrial fibrillation. Am J Cardiol 2012;110: 845–51. Steffel J, Braunwald E. Novel oral anticoagulants: focus on stroke prevention and treatment of venous thrombo-embolism. Eur Heart J 2011;32:1968–76. http://www.ema.europa.eu/ema (accessed 19 Nov 2013). 527 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Review 34 35 36 37 38 39 40 41 42 528 Eerenberg ES, Kamphuisen PW, Sijpkens MK, et al. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation 2011;124:1573–9. Gavillet M, Angelillo-Scherrer A. Quantification of the anticoagulatory effect of noval anticoagulants and management of emergencies. Cardiovasc Med 2012;15:170–9. Lu G, DeGuzman FR, Karbarz MJ, et al. Reversal of rivaroxaban mediated anticoagulation in animal models by a recombinant antidote protein (r-antidote, PRT064445). Eur Heart J 2011;32:640–1. Mega JL, Braunwald E, Wiviott S, et al. Rivaroxaban in patients with recent acute coronary syndrome. N Engl J Med 2012;366:9–19. Alexander JH, Lopes RD, James S, et al. Apixaban with antiplatelet therapy after acute coronary syndrome. N Engl J Med 2011;365:699–708. http://news.bms.com/press-release/partnering-news/new-eliquis-apixaban-posthoc-subanalysis-phase-iii-aristotle-trial-de (accessed 23 May 2014). Eikelboom JW, Conolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med 2013;369:1206–14. http://clinicaltrials.gov/ct2/show/NCT01868243 (accessed 23 May 2014). Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;369:2093–104. 43 Kawaji H, Ishii M, Tamaki Y, et al. Edoxaban for prevention of venous thromboembolism after major orthopedic surgery. Orthop Res Rev 2012;4:53–64. De Caterina R, Husted S, Wallentin L, et al. General mechanisms of coagulation and targets of anticoagulants (section i). Position paper of the ESC working group on thrombosis—task force on anticoagulants in heart disease. Thromb Haemost 2013;109:569–79. 44 Answers 1. 2. 3. 4. 5. A-T, B-F, C-T, D-T A-F, B-T, C-T, D-F A-F, B-T, C-F, D-T A-F, B-F, C-T, D-T A-T, B-F, C-T, D-F Saraf K, et al. Postgrad Med J 2014;90:520–528. doi:10.1136/postgradmedj-2014-132605 Downloaded from pmj.bmj.com on September 4, 2014 - Published by group.bmj.com Non-vitamin K antagonist oral anticoagulants (NOACs): clinical evidence and therapeutic considerations Karan Saraf, Paul Morris, Pankaj Garg, et al. Postgrad Med J 2014 90: 520-528 originally published online August 1, 2014 doi: 10.1136/postgradmedj-2014-132605 Updated information and services can be found at: http://pmj.bmj.com/content/90/1067/520.full.html These include: References This article cites 36 articles, 6 of which can be accessed free at: http://pmj.bmj.com/content/90/1067/520.full.html#ref-list-1 Email alerting service Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/