Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
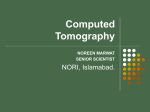
Advanced CT systems and Their Performance Scanner without covers Scanner without covers Scanner with covers SourceSource Detector Generations source detector Advantages Disadvantages collimation collimation Detector movement 1st Gen. 2nd Gen. single single Pencil beam Fanbeamlet Fanbeam single no multiple yes 3rd Gen. single 4th Gen. single Fanbeam Stationary ring no multiple Fanbeam Stationary ring no 5th Gen. 6th Gen. single 7th Gen. single 8th Gen. single Fanbeam Narrow many many Multiple cone- beam arrays wide FPD cone- beam no yes yes Trans.+ Rotates Trans.+ Rotates Faster than 1G Faster Rotates than 2G together Source Higher Rotates efficiency only than 3G No Ultrafast movement for cardiac 3rdGen.+ bed trans. 3rdGen.+ bed trans. no No scatter 3rd Gen. faster 3D imaging faster 3D imaging Large 3D slow Low efficiency High cost and Low efficiency high scatter high cost higher cost higher cost Relatively slow 4th Generation CT Scanners Rotate/Stationary • Fan beam geometry • More than 4800 detectors 6 5th generation: Electron Beam CT (EBCT) - x-ray source is not x-ray tube but a focused, steered, microwave-accelerated EB incident on a tungsten target. - It has no moving parts . - Target covers one-half of the imaging circle; detector array covers the other half. - Images in - less than - 50ms. 7 Electron Beam CT (EBCT) 8 EBCT(CONT’D) 9 Spiral (Helical) CT: Reciprocating rotation (A) versus fast continuous rotation using slip-ring technology (B) 10 12 (A) Pitch =1 (B) Pitch = 2 13 MULTISLICE SPIRAL CT • Introduced at the 1998. • They are based multiple detector. rows ranging between 8, 16, 24, 32 and 64 depending on the manufacturer. • The overall goal is to improve the volume coverage speed performance. • Complete x-ray tube/detector array rotation in less than 1s. • Partial scan images can be obtained in approximately 100ms. 14 256-slice cone-beam CT detector REAL-TIME CT FLUOLOROSCOPY • CT fluoroscopy acquire dynamic images in real time. • Fast continuous imaging, fast image reconstruction & continuous image display. • Patient movement is low during Tube rotation. • Fast image Reconstruction algorithm is required. 16 CT ANGIOGRAPHY (CTA) 17 CT VIRTUAL REALITY IAMAGING • The use of virtual reality is the creation the inner views of tubular structures. • Offers both endoluminal and extra luminal information. • It reduces complication (eg. infection and perforation). • Four requirements: – – – – data acquisition image processing 3D rendering image display and analysis. 18 What is displayed in CT images? T water CT# 1000HU water Water: 0HU Air: -1000HU Typical medical scanner display: [-1024HU,+3071HU], Range: 4096 2 12 12 bit per pixel is required in display. Hounsfield scales for typical tissues +3071 W L For most of the display device, we can only display 8 bit gray scale. This can only cover a range of 2^8=256 CT number range. Therefore, for a target organ, we need to map the CT numbers into [0,255] gray scale range for observation purpose. A 0 255 window level and window width are utilized to specify a display. -1024 0 CT #( L W / 2) Displayed Gray scale I max W I max CT # L W / 2 L W / 2 CT # L W / 2 CT # L W / 2 Windowing in CT image display Scintillator Properties of CT • • • • Transparency X-ray stopping power Light output and efficiency for lower dose Primary speed (Fast decay time or quicker response) • Luminescent afterglow for quicker speed response • Radiation damage PRIMARY SPEED • Primary speed is the rise time of the output signal in response to a constant x-ray input (~10-3-10-6seconds supporting 0.5 second scanning time). • It is also the time constant for the first component of exponential decay of that output after the input is turned off. Clinical Significance: • Primary speed is critical to maintaining high resolution during sub-second scanning. It must be fast enough to prevent blurring especially at the perimeter of the scan FOV. • A slower primary speed can be seen as shading across high contrast edges, such as the skin-air interface. AFTERGLOW • Afterglow is the second time component of the exponential decay of the output after the x-ray source is turned off. • Clinical Significance: Afterglow will result in arcing artifacts extending from low attenuation anatomy into areas of higher attenuation. It also decreases in plane spatial resolution. RADIATION DAMAGE • Radiation damage is the darkening of the material with radiation exposure over time. • It results in a gain or a shift in output for a given x-ray exposure. • It can also cause changes in Z- Axis uniformity. This is especially true for translucent materials. Clinical Significance: • Radiation damage causes changes in gain that require frequent recalibration. • It can result in changes in Z-axis uniformity which are more severe. These can cause rings or spots especially when scanning anatomy that changes rapidly along Z. TRANSPARENCY • A transparent material allows light to be transmitted with very little scatter. Most light rays can pass through with a shorter more direct path for light. • In a translucent material light rays scatter many times as they travel from the creation site to the photodiode. This longer path length can result in more self absorption, lower net light output, and greater susceptibility to radiation damage. Clinical Significance: • Transparency results in higher light output, better signal to noise, better Z-axis uniformity and reduced radiation damage. X-RAY STOPPING POWER • Stopping power is defined as the thickness of material needed to stop 98% of incident x-rays in the typical 140 kVp CT beam (~2-3 mm). Clinical Significance: • The thinner the material needed to stop 98% of the x-rays, the greater the light output at the diode. LIGHT OUTPUT • Relative light signal at the diode for a given x-ray input (~70% at 610nm). Clinical Significance: • Low light output can result in performance due to less electronic noise vs. quantum noise for thin slice, large patient, low dose application. • It can also result in low signal artifacts such as streaking at the shoulders and hips. EMMISSION SPECTRUM • The emission spectrum of a scintillator is the relative intensity of light output at a given wavelength. Clinical Significance: • In addition to diode matching for optimal electronic signal output, the emission spectrum of a scintillator can impact the design flexibility of detector systems and its long term stability. – In addition to x-ray radiation, scintillator emission in the photo active range can impact detector aging. DIODE MATCHING and RELATIVE OUTPUT • Total signal output is a function of how well the emission spectrum of the detector material and sensitivity spectrum of photo diode match. • The closer the output spectrum of the detector matches the sensitivity profile of the photo diode, the higher the resultant electrical signal. Clinical Significance: • Can reduce effective light output with the expected low signal impacts when scanning large patients with thin slices. Relative Diode Sensitivity • HiLight: 60% @ 610nm • Gadolinium Oxysulfide: 40% @510nm • Cadmium Tungstate: 42% @530nm • Relative Output • HiLight: 60% x 70% = 42% • Gadolinium Oxysulfide: 40% x 80% = 32% • Cadmium Tungstate: 42% x 30% = 13% Quality criteria for CT images The slice sensitivity profile (SSP) 1) For conventional CT and spiral/helical CT. 2) SSP is wider for 360-degree linear interpolation algorithms. 35 Scanner performance: technical parameters (I) • CT Number Accuracy – CT number depends on tube voltage, filtration, object thickness – CT number of water is by definition equal to 0 – Measured CT number should be < ± 4 HU in the central ROI • CT Number Linearity – It concerns the linear relationship between the calculated CT number and the linear attenuation coefficient of each element of the object – Deviations from linearity should be < ± 5 HU • CT Number Uniformity – It relates to the fact that a CT number of each pixel in the image of an homogeneous object should be the same over various regions – The difference in the CT number between a peripheral and a central region of an homogeneous test object should be < 8HU – Differences are largely due to beam hardening phenomenon 36 Scanner performance: technical parameters (II) • Spatial Resolution – The high contrast resolution determines the minimum size of detail visualized in the plane of the slice with a contrast >10%. It is affected by: • the reconstruction algorithm • the detector width • the effective slice thickness • the object to detector distance • the X-ray tube focal spot size • the matrix size. 37 Scanner performance: technical parameters (III) • Spatial Resolution – The low contrast resolution determines the size of detail that can be visibly reproduced when there is only a small difference in density relative to the surrounding area • Low contrast resolution is considerably limited by noise. • The perception threshold in relation to contrast and detail size can be determined, for example, by means of a contrast-detail curve. 38 Scanner performance: technical parameters (IV) • Slice Thickness – The slice thickness is determined in the center of the field of view. – The use of post-patient collimation to reduce the width of the image slice leads to very significant increases in the patient dose 39 CT number uniformity Axial image of an homogenous phantom can be assessed at the same time as measuring noise, by placing four additional ROI (N, E, S and W) at positions near the edge of the image of a uniform phantom 40 CT number linearity CT number linearity is assessed using a phantom containing inserts of a number of different materials (materials should 41 cover a wide range of CT numbers Low contrast resolution Typical image of the Catphan LCR insert Low contrast resolution (or low contrast detectability) is often quoted as the smallest visible object at a given 42 contrast for a given dose Spatial resolution (high contrast) The number of line pairs per cm just visible in the image is approximately equivalent to the 2% value of the MTF This result can then be compared with the 2% MTF The resolution is quoted as the spatial frequency (in line pairs / cm) at which the modulation falls to 50%, 10% or 43 2% MTF. Z-Sensitivity (Imaged slice width) Plan view of a test object used to measure imaged slice widths for axial scans, to assess the accuracy of post patient collimation, and to 44 calculate the geometric efficiency for the scanner Dosimetry - CTDI in air (helical) Axial slice positions Helical scan (pitch 1) The Computed Tomography Dose Index (CTDI) in air can be measured using a 10cm pencil ionization chamber, bisected 45 by the scan plane at the isocentre. Dosimetry - CTDI in Perspex Phantoms Insert to plug holes Body phantom (or annulus Head phantom to fit over haed phantom) 46 Dosimetry - CTDI in Perspex Phantoms Central and peripheral CTDI’s are used to calculate weighted CTDI, CTDIw: 1 n CTDI w = C ( 1 2 CTDI 100, c + CTDI 100, p 3 3 ) CTDIws can be compared against diagnostic reference levels for standard scan examinations 47 CT Noise Characteristics • For low mAs values – standard deviation decreases with increasing mAs • For higher mAs values – standard deviation stays fairly constant Transition point mAs should not increase throughout scanner life Standard Deviation mAs CT Noise Characteristics • Excessive noise can be caused by – detector sensitivity – electronic noise in detector amplifier circuits – reduced output per mAs Imaging performance (Noise) Noise is generally assessed using cylindrical phantoms, which are either filled with water or made of a tissue equivalent material Once an axial image of the phantom has been acquired, noise is obtained from the standard deviation in CT number in a region of interest (ROI) placed centrally within the image 50 Imaging performance (Noise) Region of interest (ROI) 51 SNR is dependent on dose, as in X-ray. Notice how images become grainier and our ability to see small objects decreases as dose decreases. There are some similarities with X-ray. But we also see some important differences. Actions that can influence image quality Avoid bad viewing conditions (e.g. lack of monitor brightness or contrast, poor spatial resolution, etc) Improve insufficient skill to use the workstation capabilities to visualize images (window level, inversion, magnification, etc). Reduce artifacts due to incorrect digital post-processing (creation of false lesions or pathologies) Compromise between image quality and compression level in the images 53