Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
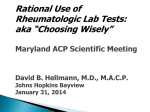
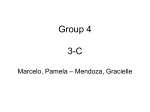
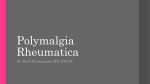
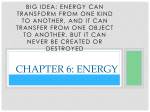
Vasculitis Syndromes Polymyalgia Rheumatica,Giant Cell Arteritis, Wegener’s Granulomatosis, Polyarteritis Nodosa What is Vasculitis? • Disease characterized by inflammation of blood vessel walls, leading to altered blood flow through obstructed walls. This causes ischemia and tissue damage. • In addition there is an intense inflammatory rxn causing further systemic signs and symptoms • Can be fatal You Should Suspect Vasculitis • • • • • • • • • • • Unexplained signs and sxs Multisystem disease Unexplained elevated ESR/CRP Skin lesions (palpable purpura) Ischemic vascular changes (Raynaud’s, gangrene, livedo, claudication) Glomerulonephritis Mononeuritis multiplex Intestinal angina Inflammatory ocular diease Arthalgias/arthritis, myalgias Sudden visual loss/headache Select Vasculitides • Polymyalgia Rheumatica • Giant Cell or Temporal Arteritis • Wegener’s Granulamatosis • Polyarteritis Nodosa Polymyalgia Rheumatica (PMR) • Most ‘benign‘ of the group • Common: 50/100,000, age > 50, average age 75. Highest prevalence in northern European ancestry, females>>males • Cause unknown PMR Clinical Presentation • Usually abrupt onset • Intense morning stiffness and pain that can last all day involving the shoulders and hip girdle area • No small joint involvement • Muscle strength normal • Fatigue and anorexia common • Elevated CRP and ESR; anemia of chronic disease, elevated platelets • 15% get GCA (more later) PMR Treatment • Low Dose Steroids (10-20 mg/day) – The only drug that works – Look to normalize the CRP and ESR; if they continue to be elevated, rethink the dx (?paraneoplastic syndrome or GCA) – Usually self-limited: 65% of patients able to taper off Prednisone by 1 year, >85% in 2 years – Disease flares not uncommon as prednisone is tapered and may require dose adjustments Giant Cell Arteritis • • • • • Can occur exclusively but often seen with PMR Rare: 15/100,000 Age >50 Cause unknown Involves the medium/large blood vessels of the head and neck including the blood vessels that supply the optic nerve GCA Pathophysiology • Unknown trigger causes inflammatory response with the release of IL-1 and IL-6. • This leads to systemic symptoms and the infiltration of inflammatory cells into the adventitia of the temporal and other involved arteries • Typical histologic pattern: Giant Cells GCA Clinical Presentation • • • • • • • Variable Scalp tenderness Temporal headaches Jaw Claudication Sudden loss of vision +/- PMR sxs Rare- upper extremity claudication due to subclavian involvement • Constitutional sxs: FUO, wt loss, fatigue • Bounding OR absent temporal artery pulses • Rarely subclavian bruits GCA Diagnostic Studies • Temporal Artery Biopsy is the gold standard • Elevated ESR and CRP, usually levels higher than in PMR • Anemia • Elevated LFTs not uncommon Treatment of GCA • High dose Steroids (60 mg/day) is the only drug that works • Slow taper over time usually 1-2 years. Some patients require low dose (<10 mg/day) chronically GCA Complications • • • • Blindness Scalp Necrosis Lingual Infarction Aortic Dissection/Aneurysm • Complications from high dose steroids: osteoporosis, cataracts, elevated blood sugars, wt. gain etc. Wegener’s Granulomatosis (WG) • Potentially fatal vasculitis involving small vessels • Rare: 3-14/million, more common in whites, any age but rare in children • Pathology shows necrotizing granulomas usually in upper airways, lungs and kidneys WG Pathophysiology • Complex immunopathogenic events in which the production and activity of ANCAs (usually c-ANCA) play a central role. These autoantibodies interact with primed neutrophils to cause vascular injury and necrosis. • Histologic lesions show granulomas WG Clinical Presentation • Variable, multisystem involvement • Organs: – Eyes: episcleritis/scleritis, proptosis due retro-orbital mass – CNS: rare mass lesion – Upper airway: otitis media, nasal chondritis, sinusitis with purulent drainage and epistaxis, ulcerations, subglottic stenosis – Kidney: neprotic syndrome, proteinuria, renal failure – Skin: palpable purpura due to leukocytoclastic vasculitis, pyoderma gangrenosum, panniculitis – Lung: cough, hemoptysis, hemorrhage, resp failure – Cardiac: pericarditis, conduction abnormalities – Systemic: fever, night sweats, wt loss, fatigue Palpable Purpura Eye Involvement Face Involvement WG Diagnostic Studies • Presence of c-ANCA (cytoplasmic staining pattern antineutrophil cytoplasmic antibodies + clinical picture is often enough to make the diagnosis. It is + 80-90% of generalized WG. • If the c-ANCA is -, tissue biopsy of lung or kidney is recommended. • “Limited” refers to disease limited to the airways; c-ANCA often is -. Additional labs • • • • Elevated CRP and ESR Anemia, leukocytosis, & thrombocytosis Elevated Cr Active urine sediment with red cell casts, hematuria and proteinuria WG Clinical Course/Progression • Prior to immunosuppression therapies, WG was uniformly fatal. Now survival rates almost 90% with aggressive treatment. • High dose steroids and Cyclophosphamide are cornerstone of therapy. Methotrexate or Azathioprine sometimes used as steroid sparing agents. Polyarteritis Nodosa (PAN) • • • • Medium vessel vasculitis Can be caused by Hep B 5/million cases Peak incidence 50’s & 60’s, slightly more common in males PAN Pathophysiology • In Hep B assoc cases immune complexes play significant role • In non Hep B cases, the pathophysiology is less understood PAN Clinical Presentation • Systemic: fever, fatigue, wt loss • Abdominal pain due to mesenteric angina/ischemia • Mononeuritis multiplex • Myalgias/arthalgias/mild arthritis • Hypertension • Skin: livedo reticularis, palpable purpura, fingertip ulceration, subcutaneous nodules • Testicular pain or tenderness Livedo reticularis Subcutaneous Nodules Complications of PAN • • • • Chronic renal failure Bowel perforation Stroke/cerebral hemorrhage due to HTN Foot/wrist drop Wrist Drop Labs of PAN • Elevation of acute phase reactants (ESR, CRP etc) • Absence of ANCA • Elevated transaminases, decreased albumin • +/- Hep B • Urine: proteinuria and hematuria without casts Imaging Studies of PAN • Mesenteric and/or renal angiography is the test of choice • Biopsies seldom done Angiogram PAN Treatment • High dose steroids and Cyclophosphamide • Methotrexate or Azathioprine is used as steroid sparing agents later once the disease is controlled • Treatment for Hep B with antivirals. Sometimes plasma exchange is used to remove immune complexes