Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Quantium Medical Cardiac Output wikipedia , lookup
Aortic stenosis wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
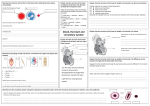
Case study: Complex congenital cardiac lesions… Introduction MDCT and Cardiac MRI has stimulated the interest of radiologists in the diagnosis of congenital heart disease and encouraged the reappraisal of classifications and definitions used by cardiologists and cardiac surgeons. The segmental analysis of congenital heart disease was introduced 25 years ago and is now used worldwide. Radiographics April 2010 3 Step segmental review: Step 1: Visceroatrial situs is determined. Step 2: left- or rightward orientation of the ventricular loop is evaluated, and the positions of the ventricles are identified on the basis of their internal morphologic features. Step 3: The position of the great vessels is determined first, and any abnormalities are noted. 1 1 1 2 1 1 3 1 (1,2,3) (S,–,–), (I,–,–), (A,–,–). Three step Review: Assessment of Connecting Segments Step 4 Atrioventricular :The relationships between the atria and ventricles. Step 5 Ventriculoarterial :The ventricles and great vessels. Step 6 Associated abnormalities : Cardiac chambers, septa, outflow tract, and great vessels. 4 4 6 5 6 6 Step 1 Step 1: Determining the Visceroatrial Situs (S,–,–), (I,–,–), (A,–,–). Step 1: Describe the position of the heart in the thorax 3 types of cardiac malposition: (determined by the orientation of the cardiac base-apex axis) Dextrocardia Mesocardia Levocardia (It is therefore important to detect any thoracic or pulmonary anomalies that might lead to displacement of the heart) Step 1: Situs Liver Stomach Spleen Step 1:Situs There are three types of situs: solitus (S,–,–), inversus (I,–,–), and ambiguus (A,–,–). The type of situs is determined by the relationship between the atria and the adjacent organs. Step 1: Situs Solitus Right atrium and liver on the right side; Lhe left atrium, stomach, and spleen on the left side; Right-sided trilobed lung with an early origin of the upper lobe bronchus from the right main stem bronchus; Left-sided bilobed lung with a more distal origin of the upper lobe bronchus. The right pulmonary artery lies in front of the right bronchus, and the left pulmonary artery crosses above the left bronchus. Situs Ambiguus When the situs is neither solitus nor inversus, it is referred to as situs ambiguus or heterotaxy. Two subsets: right isomerism (asplenia) left isomerism (polysplenia) Situs Ambiguus Left isomerism is usually indicated by bilateral bilobed lungs, interruption of the IVC, multiple spleens, and pulmonary veins that drain into both the right and the left atria Step 1: Tracheo-Bronchial tree Bilateral trilobed lungs Step 1:Atrium Locate and identify the left and right atria. Anatomically, the atrial chamber differentiation is based on the morphologic aspect of the atrial appendages. Right atrial appendage is broad and blunt (triangular) Left atrial appendage is narrow, pointed, and tubular (fingerlike). Most of the time, the appendages are not reliably identifiable at radiologic imaging, and the localization of noncardiac organs is more helpful for determining the situs Step 1:Atrium Supradiaphragmatic portion of the IVC also provides a reliable landmark for locating the anatomic right atrium (rule of venoatrial concordance) Supradiaphragmatic IVC IVC RA RA LA RA Step 1: Systemic venous structures Main venous abnormalities that should be sought: (a) a left superior vena cava with or without an innominate vein that drains either into the right atrium via the coronary sinus or directly into the left atrium (b) a retroaortic position of the brachiocepahlic vein, behind the ascending aorta (c) an interrupted inferior vena cava with azygos vein continuation. SVC 1 SVC 2 SVC 1 AZV SVC 2 SVC 1 SVC 2 SVC 1 SVC 2 SVC 1 SVC 1 SVC 2 Step 1 summary Levocardia Situs ambiguous/inversus(spleen present) Bilateral Trilobed lungs Abnormal tracheo bronchial tree ? Common atrium TAPVC Bilateral SVC Bowel malrotation ? unsure Step 2 Step 2: Determining the Orientation of the Ventricular Loop (–,D,–) (–,L,–). Step 2: Determining the Orientation of the Ventricular Loop The ventricular may tend rightward (dextro-loop) (–,D,–) or leftward (levo-loop) (–,L,–). Step 2: Identification of Right and Left Ventricles Morphologic features:. Right ventricle: Coarse trabeculae, apical moderator band. Left ventricle: Thin and delicate trabeculae, septal surface is smooth Step 2: Identification of Right and Left Ventricles Loop rule: The identification may be based on the assumption that in the presence of: a right-sided aortic valve, the right ventricle is located to the right of the left ventricle (d-loop), a left-sided aortic valve, the right ventricle is located to the left of the left ventricle (l-loop). Step 2: Atrio ventricular valves In general, the mitral valve is associated with the morphologic left ventricle, and the tricuspid valve is associated with the morphologic right ventricle D-loop, the tricuspid valve is located to the right of the mitral valve. L-loop, it is to the left of the mitral valve. RV ?LV Step 2 summary: Single right ventricle ?Hypoplastic left ventricle D-Loop Step 3 Step 3: Determining the Origin and Position of the Great Vessels (–,–,S); (–,–,I); (–,–,D-TGV) (–,–,L-TGV); (–,–,D-MGV), (–,–,L-MGV). Step 3: Determining the Origin and Position of the Great Vessels 6 variants: Normal position (solitus) (–,–,S); Inverted position (inversus) (–,–,I); D-transposition (–,–,D-TGV) L-transposition (–,–,L-TGV); D-malposition (–,–,D-MGV) L-malposition (–,–,L-MGV). Step 3: Determining the Origin and Position of the Great Vessels Malposition: If the ventricular origin of an abnormal vessel cannot be determined or if the great vessels arise from a single ventricle Transposition usually applies when the aorta arises from the right ventricle and the pulmonary artery arises from the left ventricle Step 3: Great vessels Two types of transposition exist: d-transposition (S,D,D-TGV) and l-transposition (S,L,L-TGV). In L-transposition: aorta and pulmonary artery switch positions In L-transposition: Great vessel and ventricular swich(physiologically corrected transposition) Normal relationship of the great vessels Aorta PA Step 3 summary D – MGV Aorta is positioned anterior and to the right of a hypoplastic pulmonary artery Three step Review:Assessment of Connecting Segments Assessment of Connecting Segments: Atrioventricular Connections 5 types of atrioventricular connection: 2 ventricles present Normal (RA – RV and LA – LV) discordant (RA – LV and LA to RV) Ambiguous(in cases of heterotaxy) Single Ventricle double inlet absent right or left connection Assessment of Connecting Segments: Ventriculoarterial Connections 4 types: Normal (the pulmonary artery arises from the right ventricle, and the aorta arises from the left ventricle); Transposition of the great vessels (the pulmonary artery arises from the left ventricle, and the aorta arises from the right ventricle); Double outlet right ventricle (the great vessels arise from the right ventricle); Double outlet left ventricle (the great vessels arise from the left ventricle) Assessment of Connecting Segments: Associated Malformations ASD, VSD, size of the ventricles, and the presence and degree of any ventricular outflow tract stenosis. The aorta and pulmonary artery also should be carefully examined for evidence of hypoplastic and stenotic lesions (eg, aortic coarctation and hypoplasia of the aortic arch) + PDA. The Report The report Images from thoracic CT angiography show situs ambiguous (step 1), with the liver in the midline and towards the left, the stomach and spleen on the right. There is a common atrium with bilateral SVC’s and a TAPVC. Abnormal tracheobronchial tree with bilateral right lungs. (step 2) Only one ventricle is seen, and its trabecular inner surface is characteristic of a right ventricle; this finding is suggestive of left ventricular hypoplasia. A normal aorta is seen anterior and to the right of a hypoplastic pulmonary artery (step 3). The final report showed A,D, D-MGV, with an absent left atrioventricular connection and with a double outlet right ventricle. Discussion Heterotaxy syndromes DORV (Great vessels originate from the RV,VSD, RARE) Single Ventricle( Most common LV,MPGV, RARE, High morbidity) Hypoplastic left heart/Shone(PDA,ASD,dead in 1 week,large RA, pulm oedema)