Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
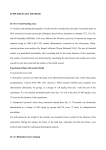
Am J Physiol Heart Circ Physiol 279: H2456–H2463, 2000. Preserved ventricular contractility in infarcted mouse heart overexpressing 2-adrenergic receptors XIAO-JUN DU, XIAO-MING GAO, GARRY L. JENNINGS, ANTHONY M. DART, AND ELIZABETH A. WOODCOCK Baker Medical Research Institute and Alfred Heart Centre, Alfred Hospital, Melbourne 8008, Victoria, Australia Received 8 March 2000; accepted in final form 2 June 2000 echocardiography; heart failure; hemodynamics; transgenic mice rimental in the development of HF remains controversial. Clinical studies provide evidence that excessive -adrenergic activity is detrimental in the heart with compromised structure and function (5). Long-term -blockade treatment significantly improves cardiac function and prognosis in HF patients (5, 11, 18), and hence a downregulated -adrenergic system could be interpreted as adaptive and self-protective. However, treatment with -blockers simultaneously improves both contractile function and -adrenergic signaling (4, 11–13, 16), suggesting the possibility that restoration of the latter, with or without upregulation of 1-AR, might contribute to the improved function. The controversy extends to the experimental situation. Transgenic strains that overexpress 1-AR and Gs␣ have a cardiac phenotype of hypertrophy and dysfunction (3, 8, 14, 23). In contrast, transgenic (TG) mice that overexpress 2-AR, ARK inhibitor, or AC have markedly enhanced cardiac contractility without significant cardiac pathology at least up to 8 mo of age (9, 15, 19, 25, 29). While overexpression of 2-AR at a high level accelerates the development of HF induced genetically or by pressure overload (6, 7, 24), expressing 2-AR at a low level (⬃30-fold) or expressing a ARK inhibitor prevented cardiac hypertrophy and dysfunction in two genetic HF models (6, 24). TG mice (TG4) with cardiac-specific overexprssion of 2-AR have constitutively activated -adrenergic signaling due to an ⬃200-fold increase in 2-AR concentration (19). In this study, we sought to determine whether overexpression of 2-AR was beneficial or detrimental following experimentally induced myocardial infarction (MI). -ADRENERGIC SYSTEM plays a key role in heart failure (HF) (5). In response to chronically elevated cardiac sympathetic drive, -adrenergic signaling is suppressed with 30–50% loss of 1-adrenergic receptors (1-AR), reduced adenylyl cyclase (AC) activity, and a lower ratio of Gs/Gi proteins (5). Meanwhile, the expression and the activity of -AR kinase 1 (ARK1), which is involved in -AR downregulation and desensitization, are elevated (5). However, whether these changes in -adrenergic activity are beneficial or det- Mice, genotyping, and 2-AR binding. Parent TG mice (TG4) that overexpress 2-AR by ⬃200-fold were generated at the Howard Hughes Medical Institute, Duke University Medical Center (Durham, NC) (19). TG mice were crossed with F1 mice from C57BL ⫻ SJL strains. The genomic DNA was extracted from tail biopsy, and expression of the trans- Address for reprint requests and other correspondence: X.-J. Du, Baker Medical Research Institute, St Kilda Road Central, PO Box 6492, Melbourne 8008, Victoria, Australia (E-mail: xiaojun.du @baker.edu.au). The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. THE H2456 METHODS 0363-6135/00 $5.00 Copyright © 2000 the American Physiological Society http://www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017 Du, Xiao-Jun, Xiao-Ming Gao, Garry L. Jennings, Anthony M. Dart, and Elizabeth A. Woodcock. Preserved ventricular contractility in infarcted mouse heart overexpressing 2-adrenergic receptors. Am J Physiol Heart Circ Physiol 279: H2456–H2463, 2000.—Effects of cardiac specific overexpression of 2-adrenergic receptors (2-AR) on the development of heart failure (HF) were studied in wildtype (WT) and transgenic (TG) mice following myocardial infarction (MI) by coronary artery occlusion. Animals were studied by echocardiography at weeks 7 to 8 and by catheterization at week 9 after surgery. Post-infarct mortality, due to HF or cardiac rupture, was not different among WT mice, and there was no difference in infarct size (IS). Compared with the sham-operated group (all P ⬍ 0.01), WT mice with moderate (⬍36%) and large (⬎36%) IS developed lung congestion, cardiac hypertrophy, left ventricular (LV) dilatation, elevated LV end-diastolic pressure (LVEDP), and suppressed maximal rate of increase of LV pressure (LV dP/dtmax) and fractional shortening (FS). Whereas changes in organ weights and echo parameters were similar to those in infarcted WT groups, TG mice had significantly higher levels of LV contractility in both moderate (dP/dtmax 4,862 ⫾ 133 vs. 3,694 ⫾ 191 mmHg/s) and large IS groups (dP/dtmax 4,556 ⫾ 252 vs. 3,145 ⫾ 312 mmHg/s, both P ⬍ 0.01). Incidence of pleural effusion (36% vs. 85%, P ⬍ 0.05) and LVEDP levels (6 ⫾ 0.3 vs. 9 ⫾ 0.8 mmHg, P ⬍ 0.05) were also lower in TG than in WT mice with large IS. Thus 2-AR overexpression preserved LV contractility following MI without adverse consequence. 2-AR OVEREXPRESSION AND MYOCARDIAL INFARCTION occlusion of the aorta. This procedure was repeated three times, and the averages of the peak levels of dP/dtmax and LVSP were used as indexes for the maximal contractile reserve. Morphometry and organ weights. Animals were killed by pentobarbitone overdose. The chest was opened to determine whether pleural effusion was present before isolation of the heart. The heart was immersed in saline on ice. The LV, right ventricle (RV), and atria were separated and weighed. When organic thrombus was present in the left atrium, the weight of thrombus was subtracted. The lungs and liver were weighed, and the tibial length was measured. LVs were fixed in 10% formalin in PBS for sectioning. Infarct size determination. The LV was embedded in paraffin and serially cut from the apex to the base. A 5-m transverse section was collected every 0.8 mm, and 5–7 sections were obtained from each LV. Sections were stained with hematoxylin and eosin, and images were digitized. The lengths of the entire endo- and epicardial circumferences and portions of infarcted segments from both sides were measured using the Optimas 6.5 program. Percentages of infarcted LV of the endo- and epicardial circumferences were calculated, and the averages were used (10, 21). Statistics. Results are expressed as means ⫾ SE or as percentages. For parametric data, between-group comparison was made by analysis of variance followed by unpaired Student’s t-test. The chi-square test or Fisher’s exact test was used to compare percentages between groups. The leastsquare method was used for linear correlation and regression. RESULTS Outcome of surgery. Of 125 operated mice, 20 (11 WT and 9 TG) died within 24 h due to surgical reasons. All sham-operated mice survived until the time of functional study. Of 83 mice with coronary artery occlusion that survived longer than 24 h, 35 (21 WT and 14 TG) Fig. 1. Transverse sections of the left ventricle (LV) from mice without (A) and with (B and C) myocardial infarction (MI) for 9 wk. D: left atrium with chronic thrombi from a mouse with large infarct. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017 gene was detected by Southern blot hybridization with the use of a 32P-labeled Hinc II fragment of the transgene construct (19). Both male and female animals, ages 12–18 wk, were used. 2-AR density in the left ventricle (LV) was measured in a separate group of TG and WT mice (n ⫽ 6 each). Saturation curves were generated by incubating myocardial membrane proteins with [125I]-(l)-iodocyanopindalol (125I-CYP; 2,200 Ci/ mmol; NEN) at 12–400 pmol/l for 1 h to determine the affinity of receptors. Nonspecific binding was determined by the presence of l-isoproterenol at 20 mol/l. The binding assay was performed by incubating membrane proteins with 100 pmol/l 125I-CYP for 1 h in the presence of ICI-118551 (Sigma) at 10⫺11 –10⫺5 mol/l. 2-AR density was 300-fold higher in TG than in WT hearts (1,506 ⫾ 274 vs. 5 ⫾ 2 fmol/mg protein). Microsurgery. Experimental procedures were approved by the local animal experimentation ethics committee. Mice were anesthetized (mixture of 8 mg/100 g ketamine, 2 mg/ 100 g xylazine, 0.06 mg/100 g atropine, and 0.1 mg/100 g temgesic as a pain reliever), intubated, and ventilated. Under a surgical microscope, a left thoracotomy was performed to expose the heart. The location of the left coronary artery was identified and then occluded with a 7-0 silk suture, as described previously in detail (10). Sham-operated mice underwent similar surgery without occlusion of the coronary artery. Echocardiography. Transthoracic echocardiography was performed with the use of a Hewlett-Packard Sonos 5500 ultrasound machine with a 12-MHz phased-array transducer (0.5- to 0.7-cm standoff added), as described previously (10). Mice were anesthetized with the anesthetic mixture as used for surgery and placed on a heating pad. A standard lead II electrocardiogram was recorded for heart rate (HR) measurement. After a short-axis two-dimensional (2D) image of the LV was obtained at a level close to the papillary muscles, a 2D guided M-mode image crossing the anterior and posterior walls was recorded (sweep speed 100 mm/s). Parameters measured digitally on the M-mode trace were LV inner dimensions of diastole and systole (LVIDd, LVIDs), LV external dimension of diastole (LVEDd), and fractional shortening [FS ⫽ (LVIDd ⫺ LVIDs)/LVIDd] (10). Cardiac catheterization. Cardiac function was assessed by cardiac catheterization. Mice were anesthetized (pentobarbitone 8 mg/100 g and atropine 0.06 mg/100g ip) and placed supine on a heating pad. A 1.4-F Millar microtipped transducer catheter was inserted into the LV via the right carotid artery. The aortic blood pressure, LV pressures, and the maximal rate of increase or decay of LV pressure (dP/dtmax or dP/dtmin, respectively) were recorded. HR was derived from pulse signals. To further characterize the murine MI model of HF, in sham-operated and infarcted WT mice, a 1-agonist, dobutamine, was infused intravenously at increasing doses of 7.5– 480 ng/min per mouse for 1–3 min (0.028–1.8 g/kg), and the functional response was monitored. To assess the cardiac functional reserve, in some WT and TG mice with MI, the peak levels of LV systolic pressure (LVSP) and dP/dtmax were measured during a brief occlusion of the aorta by following the method previously applied to the rat (21). While the Millar catheter remained in the LV, mechanical ventilation was commenced, and the chest was opened by a midline incision via the sternum. The ascending aorta was dissected, and a fine suture enclosed the aorta. After stabilization, the aortic blood flow was stopped by tightening the suture for 3 s, and LV pressure and dP/dt were continuously recorded immediately before and during the H2457 2-AR OVEREXPRESSION AND MYOCARDIAL INFARCTION H2458 Table 1. Body weight, infarct size, and organ weights in mice with sham-operation and with MI for 9 wk Group (n, M/F) Wild type Sham (12, 4/8) m-IS (11, 4/7) l-IS (13, 6/7) Transgenic Sham (10, 4/6) m-IS (12, 5/7) l-IS (11, 4/7) IS, %LV BW1, g BW2, g Tibia Length, mm 28.3 ⫾ 2.2 46.4 ⫾ 1.3‡ 24 ⫾ 2 25 ⫾ 1 28 ⫾ 1 26 ⫾ 2 27 ⫾ 1 28 ⫾ 1 17.9 ⫾ 0.2 17.8 ⫾ 0.1 17.6 ⫾ 0.2 25.0 ⫾ 2.5 44.3 ⫾ 1.8‡ 24 ⫾ 1 27 ⫾ 1 25 ⫾ 2 27 ⫾ 1 29 ⫾ 1 27 ⫾ 1 17.7 ⫾ 0.2 18.1 ⫾ 0.1 17.8 ⫾ 0.2 LV Weight, mg RV Weight, mg Atria Weight, mg Lung Weight, mg Pleural Effusion 122 ⫾ 8 164 ⫾ 7* 195 ⫾ 7*‡ 89 ⫾ 6 119 ⫾ 4* 136 ⫾ 5*‡ 22 ⫾ 2 28 ⫾ 2* 37 ⫾ 3*‡ 12 ⫾ 1 17 ⫾ 2* 22 ⫾ 2*‡ 133 ⫾ 4 178 ⫾ 14* 203 ⫾ 15* 0/12 2/11 11/13* 127 ⫾ 8 158 ⫾ 9* 184 ⫾ 12*‡ 93 ⫾ 6 116 ⫾ 7* 124 ⫾ 8* 22 ⫾ 1 25 ⫾ 1 36 ⫾ 4*‡ 12 ⫾ 1 17 ⫾ 1* 25 ⫾ 3*‡ 142 ⫾ 4 154 ⫾ 5 209 ⫾ 21*‡ Heart Weight, mg 0/10 2/12 4/11*† Values are means ⫾ SE; n ⫽ no. of animals. M/F, male/female; IS, infarct size; BW1 and BW2, body weight at the time of surgery and 9 wk afterward, respectively; LV and RV, left and right ventricle; m-IS and l-IS, moderate (⬍36%) and large (⬎36%) IS; MI, myocardial infarction. * P ⬍ 0.05 vs. respective sham group; † P ⬍ 0.05 vs. respective wild-type group; ‡ P ⬍ 0.05 vs. respective m-IS group. Cardiac function in WT mice. Echocardiography was performed at 7–8 wk, and LV catheterization was done at 9 wk after surgery. In WT and TG mice, HR levels recorded at echo test were higher than those recorded during catheterization (Table 2), most likely because of the different anesthetic regimes used (see METHODS). LV dimensions of systole and diastole were significantly increased, and FS was reduced in infarcted mice compared with control levels (Table 2 and Fig. 2). At 9 wk after surgery, mean arterial pressure (MAP) and LV end-diastolic pressure (LVEDP) were significantly elevated (Table 2) and LVSP, dP/dtmax, and dP/dtmin were reduced in MI groups versus controls (Fig. 3A). These changes were more pronounced in animals with large IS (Table 2). We tested the LV functional response to dobutamine given intravenously. In sham-operated animals, dobutamine induced a dose-dependent increase in dP/dtmax, LVSP, and HR. The inotropic responses were significantly depressed in mice with moderate and large IS (Fig. 4), whereas HR responses were attenuated only in the large IS group. These results indicate downregulation of -adrenergic signaling in the infarcted mouse heart. Differences between TG and WT mice. Pleural effusion, a sign of left HF (7), was less frequent in TG than in WT mice with large IS (36% vs. 85%, P ⬍ 0.05, Table 1). Increases in weights of heart or LV, RV, and atria were similar between WT and TG mice with MI. In Table 2. Functional measures by echocardiography and by catheterization in mice with sham-operation or MI Group Wild type Sham m-IS l-IS Transgenic Sham m-IS l-IS HR1, beats/min LVIDd, mm LVIDs, mm FS, % LVEDd, mm HR2, beats/min MAP, mmHg LVSP, mmHg 310 ⫾ 16 384 ⫾ 21* 380 ⫾ 21* 3.3 ⫾ 0.2 4.6 ⫾ 0.2* 5.8 ⫾ 0.3*‡ 1.8 ⫾ 0.2 3.6 ⫾ 0.3* 4.8 ⫾ 0.4*‡ 46 ⫾ 2 23 ⫾ 4* 17 ⫾ 3*‡ 5.2 ⫾ 0.2 6.2 ⫾ 0.2 7.2 ⫾ 0.3*‡ 346 ⫾ 20 332 ⫾ 15 327 ⫾ 13 72 ⫾ 3 58 ⫾ 5* 61 ⫾ 4* 96 ⫾ 3 86 ⫾ 2* 80 ⫾ 4* 3 ⫾ 0.3 6 ⫾ 0.8* 9 ⫾ 0.8*‡ 499 ⫾ 29† 528 ⫾ 26† 528 ⫾ 26† 3.6 ⫾ 0.2 4.6 ⫾ 0.3* 5.2 ⫾ 0.3* 2.0 ⫾ 0.2 3.3 ⫾ 0.4* 4.2 ⫾ 0.3* 47 ⫾ 3 31 ⫾ 5* 21 ⫾ 3*‡ 5.2 ⫾ 0.2 6.1 ⫾ 0.2* 6.8 ⫾ 0.3*‡ 458 ⫾ 15† 461 ⫾ 9† 431 ⫾ 23† 84 ⫾ 5 67 ⫾ 2* 66 ⫾ 3* 112 ⫾ 5† 91 ⫾ 2* 87 ⫾ 4* 3 ⫾ 0.4 5 ⫾ 0.6* 6 ⫾ 0.3*†‡ LVEDP, mmHg Values are means ⫾ SE. HR1 and HR2, heart rates measured at the time of echocardiography (7–8 wk) and cardiac catheterization (9 wk), respectively; LVIDd and LVIDs, LV internal dimension at diastole or systole, respectively; FS, fractional shortening; MAP, mean arterial pressure; LVSP, LV systolic pressure; LVEDP, LV end-diastolic pressure. * P ⬍ 0.05 vs. respective sham group; † P ⬍ 0.05 vs. respective wild-type group; ‡ P ⬍ 0.05 vs. respective m-IS group. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017 died of cardiac rupture or acute and chronic HF with a mortality of 46% for WT and 38% for TG groups (P ⫽ not significant). Mice that died of HF had a threefold increase in lung weight versus sham-operated mice (405 ⫾ 15 vs. 137 ⫾ 3 mg, P ⬍ 0.001), and the incidences of atrial thrombus and pleural effusion were 87% and 100%, respectively. Infarct size (IS) was measured in the 27 mice that died and was 52.0 ⫾ 2.5% (n ⫽ 17) in the mice that died of HF and 41.4 ⫾ 2.4% (n ⫽ 10) in the mice that died of rupture. Infarct size and grouping of surviving mice. All mice that survived coronary artery occlusion had a transmural infarct localized to the LV free wall and apex. The RV and septum were not involved (Fig. 1). IS ranged from 8% to 54% of LV and was not significantly different between WT and TG groups (36 ⫾ 2% vs. 33 ⫾ 3%). To compare cardiac function of WT and TG mice with different IS, we divided animals into subgroups with moderate and large IS by the median IS of 36% (Table 1). Organ weights in WT mice. Since body weights and tibial length were similar in all groups of WT and TG mice, the organ weights are presented as absolute values (Table 1). At 9 wk, weights of whole heart or LV, RV, and atria were significantly increased in WT mice, with MI indicating the development of hypertrophy in noninfarcted myocardium. Lung weights increased significantly, implying chronic pulmonary congestion. The degree of these changes was dependent on IS (Table 1). 2-AR OVEREXPRESSION AND MYOCARDIAL INFARCTION H2459 Fig. 2. Two-dimensional echocardiographic images (A and B) and M-mode traces (C and D) from a control mouse (A and C) and a mouse with large MI (B and D). Echo test was performed 7 wk after surgery. Infarct size in the infarcted mouse was 47% of the LV. The akinesis at the infarcted region (anterior wall) was evident. The LV inner dimension at diastole (LVIDd) was 3.6 mm for the sham-operated mouse and 5.7 mm for the infarcted mouse. Sweep speed ⫽ 100 mm/s. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017 Fig. 3. A: maximal rates of increase (dP/dtmax) and decrease in LV pressure (dP/dtmin) in sham-operated (SH) mice and mice with MI of moderate (m-IS; ⬍36%) and large infarct size (l-IS; ⬎36%) measured at 9 wk after surgery. Data are means ⫾ SE; n ⫽ 10–13 per group. *P ⬍ 0.01 vs. respective SH group; ⫹P ⬍ 0.01 vs. wild-type (WT) group. TG, transgenic group. B: changes in LV systolic pressure (LVSP) and dP/dtmax during brief periods of occlusion of the ascending aorta (AO) in infarcted WT (n ⫽ 6) and TG mice (n ⫽ 7) under open-chest conditions with mechanical ventilation. *P ⬍ 0.05 vs. WT group. infarcted mice surviving to the time of study, nine (4 TG, 5 WT) had chronic thrombus in the left atrium. All but one (32.6%) had IS ⬎36% (38.2–50.5%, average 44 ⫾ 2%). There was no significant difference among shamoperated and infarcted WT and TG groups in any of the echocardiographic parameters (Table 2), except that TG mice had a higher HR. The TG mice with large IS had significantly lower LVEDP compared with the respective WT group (P ⬍ 0.05). Although infarcted TG and WT mice had similar percent reduction in LV dP/dtmax and dP/dtmin versus respective sham-operated groups, dP/dt levels were significantly higher than those in the respective WT groups (P ⬍ 0.01, Fig. 3A). HR itself is known to influence the measurement of LV dP/dt (20). The possibility that higher levels of LV dP/dt in TG mice was due to higher HR was examined in a separate group of infarcted WT mice (n ⫽ 5) under conditions of ventilation and rapid atrial pacing by following the method described by Palakodeti et al. (20). Increasing HR from 350 ⫾ 10 to 450 to 500 beats/min led to an 18% fall in dP/dtmax (P ⬍ 0.05) from a basal level of 3,350 ⫾ 250 mmHg/s. A similar change was also observed for dP/dtmin. This suppression of dP/dt levels with rapid atrial pacing was immediately reversed when atrial pacing was stopped. Thus the difference between WT and TG mice in LV dP/dt cannot be attributed to the difference in HR levels. The contractile response to acute aortic occlusion was tested in randomly selected infarcted WT (n ⫽ 6) and TG mice (n ⫽ 7) with similar IS (38 ⫾ 3% vs. 35 ⫾ 3%, P ⫽ NS). Under conditions of open chest and ventilation, baseline LVSP (P ⫽ 0.069) and dP/dtmax (P ⬍ 0.05) were higher in TG than in WT mice. LVSP and dP/dtmax increased in both groups in response to temporary aortic occlusion. While the peak LVSP was not significantly different between groups, TG mice H2460 2-AR OVEREXPRESSION AND MYOCARDIAL INFARCTION had higher levels of dP/dtmax than WT mice did (P ⬍ 0.05, Fig. 3B). Correlation of morphometric and functional parameters. Lung weights correlated well with weights of heart (r ⫽ 0.704), LV (r ⫽ 0.523), RV (r ⫽ 0.848), and atria (r ⫽ 0.766; all P ⬍ 0.001). Furthermore, when IS exceeded a certain level (⬃30%), weights of the heart, LV, RV, atria, and lungs were increased (Table 1). IS correlated positively with LVIDd, LVIDs, and LVEDP and negatively with FS, LVSP, dP/dtmax, and dP/dtmin (all P ⬍ 0.01; Fig. 5). FS modestly correlated with dP/dtmax in either WT (r ⫽ 0.421) or TG mice (r ⫽ 0.369; both P ⬍ 0.05). The extent of LV dilatation, estimated from the LVEDd correlated negatively with FS (r ⫽ ⫺0.781, P ⬍ 0.0001). LVEDP correlated significantly with weights of the RV ( r ⫽0.466), atria (r ⫽ 0.408), and lungs (r ⫽ 0.526; all P ⬍ 0.01). DISCUSSION In this study, the development of HF in WT mice with MI was evidenced by pulmonary congestion, pleu- Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017 Fig. 4. Cardiac functional responses to increasing doses of dobutamine in WT mice subjected to sham operation or MI for 9 wk. The increase in LV dP/dtmax (A) and LVSP (B) was depressed in both infarcted groups. The increase in heart rate was also blunted in the l-IS group (C). Data are means ⫾ SE; n ⫽ 9–10 per group. *P ⬍ 0.05 vs. SH group by ANOVA. ral effusion, LV dilatation, elevation in LVEDP, and reduction in both LV contractility (dP/dt) and FS. The blunted inotropic and chronotropic responses to dobutamine indicate downregulation of the -adrenergic system in this model. Similarly to that in other species, including humans (21, 22), IS in mice is a major determinant of the extent of cardiac dysfunction, morphometric abnormalities, incidence of pathological events, and mortality. These data elucidate the features of the murine model of MI. We observed that, 9 wk after MI, TG mice with large IS had lower LVEDP and a lower incidence of pleural effusion compared with the WT group. Although dP/dt fell significantly in TG mice to the extent comparable to that in the infarcted WT mice, dP/dt levels were significantly higher in infarcted TG mice than in respective WT mice irrespective of IS. Furthermore, the peak levels of dP/dtmax caused by a brief occlusion of the ascending aorta were also significantly higher in TG than in WT mice with infarct. These findings suggest that the noninfarcted myocardium in TG mice maintained the phenotype of an enhanced inotropy. Therefore, these data demonstrate that overexpressing 2-AR in the heart provides inotropic support to the infarcted and failing ventricle. It might be expected that markedly enhanced 2adrenergic activity under conditions of MI would increase the risk of arrhythmias. In the present study, MI did not lead to excessive death in TG mice, with mortality slightly lower than that in WT mice. There was no evidence to indicate arrhythmic death in either WT or TG mice, although arrhythmias were recorded occasionally during the functional experiments. Thus overexpression of 2-AR at a high level did not cause adverse consequences in mice following MI. We recently observed facilitated onset of HF and higher mortality due to critical HF in 2-AR transgenic mice following thoracic aortic constriction (7). The different outcomes from HF models of pressure overload and MI raise the possibility that the effect of 2-AR overexpression is not only dependent on the receptor number, as suggested by recent studies (6), but also on the etiology of HF. Interestingly, it is known that the extent of -adrenergic downregulation and desensitization is more severe in pressure-overloaded heart than in ischemic disease (5). The mechanism responsible for such differences remains unclear, and potential differences in some key molecules, such as ARK1 and Gi protein, require further investigation. In infarcted TG and WT mice, the percent reduction in LV dP/dt from the respective sham-operated control levels was comparable. However, the absolute levels of dP/dtmax and dP/dtmin were significantly higher in infarcted TG than in WT groups. This finding indicates that, in TG mice, the noninfarcted myocardium maintained its hyperdynamic phenotype supported by the genetically overexpressed 2-AR. Interestingly, although infarcted TG mice had LV dP/dt levels similar to those of sham-operated WT mice, the extent of LV dilatation measured by echocardiography did not significantly improve compared with that of the infarcted 2-AR OVEREXPRESSION AND MYOCARDIAL INFARCTION H2461 WT groups. The average levels of FS in TG groups were 20–30% higher than those in WT groups, but such differences were statistically not significant. It is not clear why cardiac 2-AR overexpression differentially influences LV contractility and echocardiographic measures. We found similar FS levels in sham-operated WT and TG groups, although LV contractility was much higher in the latter. Unchanged echo indexes were also previously observed in mice with cardiac overexpression of adenylyl cyclase or 2-AR, although the basal LV dP/dt was significantly higher compared with that of WT littermate controls (9, 27). TG mice overexpressing 2-AR have markedly enhanced inotropy and chronotropy (19, 29) without deleterious changes in function and histology up to 8 mo of age, except for a mild increase in collagen content in the LV myocardium (7). In contrast, a TG line overexpressing 1-AR by 15-fold exhibits early mortality, cardiac hypertrophy, and failure (8, 23). The reasons for the differences in these TG lines remain to be elucidated and may be related to some important differences between 1-AR and 2-AR in downstream coupling and signaling, such as coupling to Gi proteins by 2-AR but not by 1-AR and the compartmentalization of 2-AR-activated AC/cAMP signaling (2, 15a, 29). 2-AR overexpression (⬃200-fold) in mice with disruption of muscle lim protein (MLP⫺/⫺) leads to worsening of HF and higher mortality (24). In another HF model caused by overexpression of Gq␣, overexpressing 2-AR at a high level worsened the outcome, whereas a low level overexpression (⬃30-fold) reversed ventricular dysfunction and suppressed cardiac hypertrophy (6). Expressing a ARK inhibitor enhanced ventricular contractility in normal mice (1, 15) and rescued the cardiomyopathic phenotype in MLP⫺/⫺ mice (24) but not in Gq␣-overexpressing mice (6). Overexpressing adenylyl cyclase in Gq␣ mice by crossbreeding improved ventricular function (26). These studies and the findings from the present study indicate that enhanced -adrenergic activity is not always associated with adverse consequences. Rapid pacing per se is able to induce the development of HF in large animals (28). It is therefore possible that higher HR in TG mice may confound the findings of the present study. The 2-AR TG strain is unique for the high HR level with the ionic mechanism Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017 Fig. 5. Correlation between infarct size and functional parameters in sham-operated control and infarcted mice. The data were combined if there was no significant different between WT and TG groups. E, WT mice; 䊐, TG mice. LVEDP, LV end-diastolic pressure; LVIDs, LV inner dimension at systole; FS, fractional shortening; LVEDd, LV external dimension at diastole. H2462 2-AR OVEREXPRESSION AND MYOCARDIAL INFARCTION We thank Dr. Robert J. Lefkowitz for supplying the transgenic line. We thank the staff at the Biological Research Unit, Elodie Percy, Binghui Wang, Rodney Dilley, and Brian Jones, for help in animal breeding, transgene screening, and image analysis. This work was supported by the National Health and Medical Research Council of Australia and a grant from the Merck Sharp & Dohme Research Fund (Australia). X.-M. Gao is the recipient of a scholarship from the Australia/China/Indonesia/Singapore Heart Foundation via Prof Y. M. Lim, Director, Singapore National Heart Center. REFERENCES 1. Akhter SA, Eckhart AD, Rockman HA, Shotwell K, Lefkowitz RJ, and Koch WJ. In vivo inhibition of elevated myocardial -adrenergic receptor kinase activity in hybrid transgenic mice restores normal -adrenergic signaling and function. Circulation 100: 648–653, 1999. 2. An RH, Heath BM, Higgins JP, Koch WJ, Lefkowitz RJ, and Kass RS. 2-Adrenergic receptor overexpression in the developing mouse heart: evidence for targeted modulation of ion channels. J Physiol (Lond) 516: 19–30, 1999. 3. Asai K, Yang GP, Geng YJ, Takagi G, Bishop S, Ishikawa Y, Shannon RP, Wagner TE, Vatner DE, Homcy CJ, and Vatner SF. -Adrenergic receptor blockade arrests myocardial damage and preserves cardiac function in the transgenic Gs␣ mouse. J Clin Invest 104: 551–558, 1999. 4. Böhm M, Deutsch HJ, Hartmann D, Rosee KL, and Stablein A. Improvement of postreceptor events by metoprolol treatment in patients with chronic heart failure. J Am Coll Cardiol 30: 992–996, 1997. 5. Bristow MR. Mechanism of action of -blocking agents in heart failure. Am J Cardiol 80: 26L–40L, 1997. 6. Dorn, GW II, Tepe NM, Lorenz JN, Koch WJ, and Liggett SB. Low- and high-level transgenic expression of 2-adrenergic receptors differentially affect cardiac hypertrophy and function in G␣q-overexpressing mice. Proc Natl Acad Sci USA 96: 6400– 6405, 1999. 7. Du XJ, Autelitano DJ, Wang BH, Dart AM, and Woodcock EA. 2-Adrenergic receptor overexpression exacerbates develop- ment of heart failure following aortic stenosis. Circulation 101: 71–77, 2000. 8. Engelhardt S, Hein L, Wiesmann F, and Lohse MJ. Progressive hypertrophy and heart failure in 1-adrenergic receptor transgenic mice. Proc Natl Acad Sci USA 96: 7059–7064, 1999. 9. Gao MH, Lai NC, Roth DM, Zhou J, Zhu J, Anzai T, Dalton N, and Hammond HK. Adenylylcyclase increases responsiveness to catecholamine stimulation in transgenic mice. Circulation 99: 1618–1622, 1999. 10. Gao XM, Dart AM, Dewar E, Jennings GL, and Du XJ. Serial echocardiographic assessment of left ventricular dimensions and function after myocardial infarction in mice. Cardiovasc Res 45: 330–338, 2000. 11. Gilbert EM, Abraham WT, Olsen S, Hattler B, White M, Mealy P, Larrabee P, and Bristow MR. Comparative hemodynamic, left ventricular functional, and antiadrenergic effects of chronic treatment with metoprolol versus carvedilol in the failing heart. Circulation 94: 2817–2825, 1996. 12. Heibrunn SM, Shah P, Bristow MR, Valantine HA, Ginsburg R, and Fowler MB. Increased -receptor density and improved hemodynamic response to catecholamine stimulation during long-term metoprolol therapy in heart failure from dilated cardiomyopathy. Circulation 79: 483–490, 1989. 13. Iaccarino G, Tomhave ED, Lefkowitz RJ, and Koch WJ. Reciprocal in vivo regulation of myocardial G protein-coupled receptor kinase expreession by -adrenergic receptor stimulation and blockade. Circulation 98: 1783–1789, 1998. 14. Iwase M, Bishop SP, Uechi M, Vatner DE, Shannon RP, Kudej RK, Wight DC, Wagner TE, Ishikawa Y, Homc CJ, and Vatner SF. Adverse effects of chronic endogenous sympathetic drive induced by cardiac Gs␣ overexpression. Circ Res 78: 517–524, 1996. 15. Koch WJ, Rockman HA, Samama P, Hamilton R, Bond RA, Milano CA, and Lefkowitz RJ. Cardiac function in mice overexpressing the -adrenergic receptor kinase or a ARK inhibitor. Science 268: 1350–1353, 1995. 15a.Kuschel M, Zhou YY, Cheng H, Zhang SJ, Chen Y, Lakatta EG, and Xiao RP. Gi protein-mediated functional compartmentalization of cardiac 2-adrenergic signaling. J Biol Chem 274: 22048–22052, 1999. 16. Liang CS, Frantz RP, Suematsu M, Sakamoto S, Sullebarger JT, Fan TM, and Guthinger L. Chronic -adrenoceptor blockade prevents the development of -adrenergic subsensitivity in experimental right-sided congestive heart failure in dogs. Circulation 84: 254–266, 1991. 17. Maurice JP, Hata JA, Shah AS, White DC, McDonald PH, Dolber PC, Wilson KH, Lefkowitz RJ, Glower DD, and Koch WJ. Enhancement of cardiac function after adenoviralmediated in vivo intracoronary 2-adrenergic receptor gene delivery. J Clin Invest 104: 21–29, 1999. 18. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure. Lancet 353: 2001–2007, 1999. 19. Milano CA, Allen LF, Rockman HA, Dolber PC, McMinn TR, Chien KR, Johnson TD, Bond RA, and Lefkowitz RJ. Enhanced myocardial function in transgenic mice overexpressing the 2-adrenergic receptor. Science 264: 582–586, 1994. 20. Palakodeti V, Oh S, Oh BH, Mao L, Hongo M, Peterson KL, and Ross J Jr. Force-frequency effect is a powerful determinant of myocardial contractility in the mouse. Am J Physiol Heart Circ Physiol 273: H1283–H1290, 1997. 21. Pfeffer MA, Pfeffer JM, Fishbein MC, Fletcher PJ, Spadaro J, Kloner RA, and Braunwald E. Myocardial infarct size and ventricular function in rats. Circ Res 44: 503–512, 1979. 22. Pfeffer MA and Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation 81: 1161–1172, 1990. 23. Port JD, Weinberger HD, Bisognano JD, Knudson OA, Bohlmeyer TJ, Pende A, and Bristow MR. Echocardiographic and histopathologic characterization of young and old transgenic mice overexpressing the human 1-adrenergic receptor (Abstract). J Am Coll Cardiol 31, Suppl A: 177A, 1998. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017 undefined. Patch-clamp studies have shown that there are no significant changes in slow delayed rectifier K⫹ current but that the density of L-type Ca2⫹ current is increased because of modulation by the activated AC/ cAMP system (2, 29). Higher HR would increase energy expenditure and shorten the diastolic filling time. It is likely that, in TG mice with genetically induced cardiomyopathy or pressure overload, the higher energy demand and restricted usage of Frank-Starling mechanism, due to shortened diastolic filling time, compromise the cardiac function and that this contributes to the adverse outcome (7, 24). It is also possible that a higher energy demand partially offsets the beneficial effect, observed in the present study, of 2-AR overexpression in TG mice with MI. Our results demonstrate a preserved ventricular contractility in 2-AR TG mice following chronic MI. This finding implies that an improved 2-adrenergic activity by 2-AR overexpression in the infarcted and failing heart could provide inotropic support to the overall ventricular contractility and is in keeping with the view for 2-AR expression or transfection as a potential approach for HF gene therapy (6, 17, 24). However, considering the diverse effects of 2-AR overexpression observed in other HF models (6, 7, 24), it is likely that the effect of transgenic overexpression of 2-AR on HF is dependent on the etiology of HF. 2-AR OVEREXPRESSION AND MYOCARDIAL INFARCTION 24. Rockman HA, Chien KR, Choi DJ, Iaccarino G, Hunter JJ, Ross J Jr, Lefkowitz RJ, and Koch WJ. Expression of a -adrenergic receptor kinase 1 inhibitor prevents the development of myocardial failure in gene-targeted mice. Proc Natl Acad Sci USA 95: 7000–7005, 1998. 25. Rockman HA, Choi D, Akhter SA, Jaber M, Giros B, Lefkowitz RJ, Caron MG, and Koch WJ. Control of myocardial contractile function by the level of -adrenergic receptor kinase 1 in gene-targeted mice. J Biol Chem 273: 18180–18184, 1998. 26. Roth DM, Gao MH, Lai NC, Drumm J, Dalton N, Zhou JY, Zhu J, Entrikin D, and Hammond HK. Cardiac-directed adenylyl cyclase expression improves heart function in murine cardiomyopathy. Circulation 99: 3099–3102, 1999. H2463 27. Tanaka N, Dalton N, Mao L, Rockman HA, Peterson KL, Gottshall KR, Hunter JJ, Chien KR, and Ross J Jr. Transthoracic echocardiography in models of cardiac disease in the mouse. Circulation 94: 1109–1117, 1996. 28. Vatner DE, Sato N, Galper JB, and Vatner SF. Physiological and biochemical evidence for coordinate increases in muscarinic receptors and Gi during pacing-induced heart failure. Circulation 94: 102–107, 1996. 29. Xiao RP, Avdonin P, Zhou YY, Cheng H, Akhter SA, Eschenhagen T, Lefkowitz RJ, Koch WJ, and Lakatta EG. Coupling of 2-adrenoceptor to Gi proteins and its physiological relevance in murine cardiac myocytes. Circ Res 84: 43–52, 1999. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.3 on June 17, 2017